
Abstract
A 2-month-old female Persian cat that had been showing episodes of anorexia and diarrhea for the previous 4 weeks was presented in shock and died 2 days later. Numerous Gram-positive cocci were located along the brush border of small intestinal villi, without significant inflammatory infiltration. Similar bacteria were present within hepatic bile ducts and pancreatic ducts and were associated with suppurative inflammation and exfoliation of epithelial cells. Culture of the liver and lung yielded bacteria identified as Enterococcus hirae. Fecal culture from an asymptomatic adult female from the same cattery also yielded large numbers of E. hirae. To our knowledge, this is the first report of E. hirae enteropathy in a cat and the first report of ascending cholangitis and ductal pancreatitis caused by an Enterococcus spp.
Diarrhea associated with attachment of Enterococcus durans or E. hirae to the intestinal brush border has previously been reported in suckling rats, 6 foals, 11 puppies, 2 , 8 calves, 9 and piglets. 1 , 6 This report describes a case of intestinal enterococcal infection in a kitten that had additional lesions in the liver and pancreas.
A 2-month-old female Persian cat was submitted to the pathology service of the University of Montreal veterinary school for necropsy. It came from a commercial breeding colony that had a history of anorexia and diarrhea in kittens at weaning time and of weight loss in queens at the end of gestation. The kitten had had intermittent anorexia for 4 weeks following weaning, developed diarrhea a few days before presentation, and was brought to the referring veterinarian in systemic shock. Fluid and antibiotic therapy was instituted, and the kitten partially recovered but then showed signs of neurologic impairment and died soon thereafter.
At necropsy, the perineum was lightly soiled with feces. Little content was present in the gastrointestinal tract. The lung was multifocally congested. All abdominal organs were pale, and the spleen was small. Samples from all major organs were fixed in 10% neutral buffered formalin, and sections were cut at 4 µm and stained with hematoxylin–phloxin–saffron (HPS). Sections of intestine, liver, and pancreas were also Gram stained.
Histologic examination revealed significant changes in the small intestine, pancreas, and liver. Sections of duodenum, jejunum, and ileum revealed numerous large Gram-positive cocci adherent multifocally to the brush border of villous enterocytes, forming mats of bacteria along the villi (Fig. 1). In a section of duodenal papilla, similar bacteria were present in the lumen of the papilla, often adhered to the apex of exfoliated epithelial cells. There was no perceptible inflammatory infiltration or structural alteration of the intestinal mucosa.
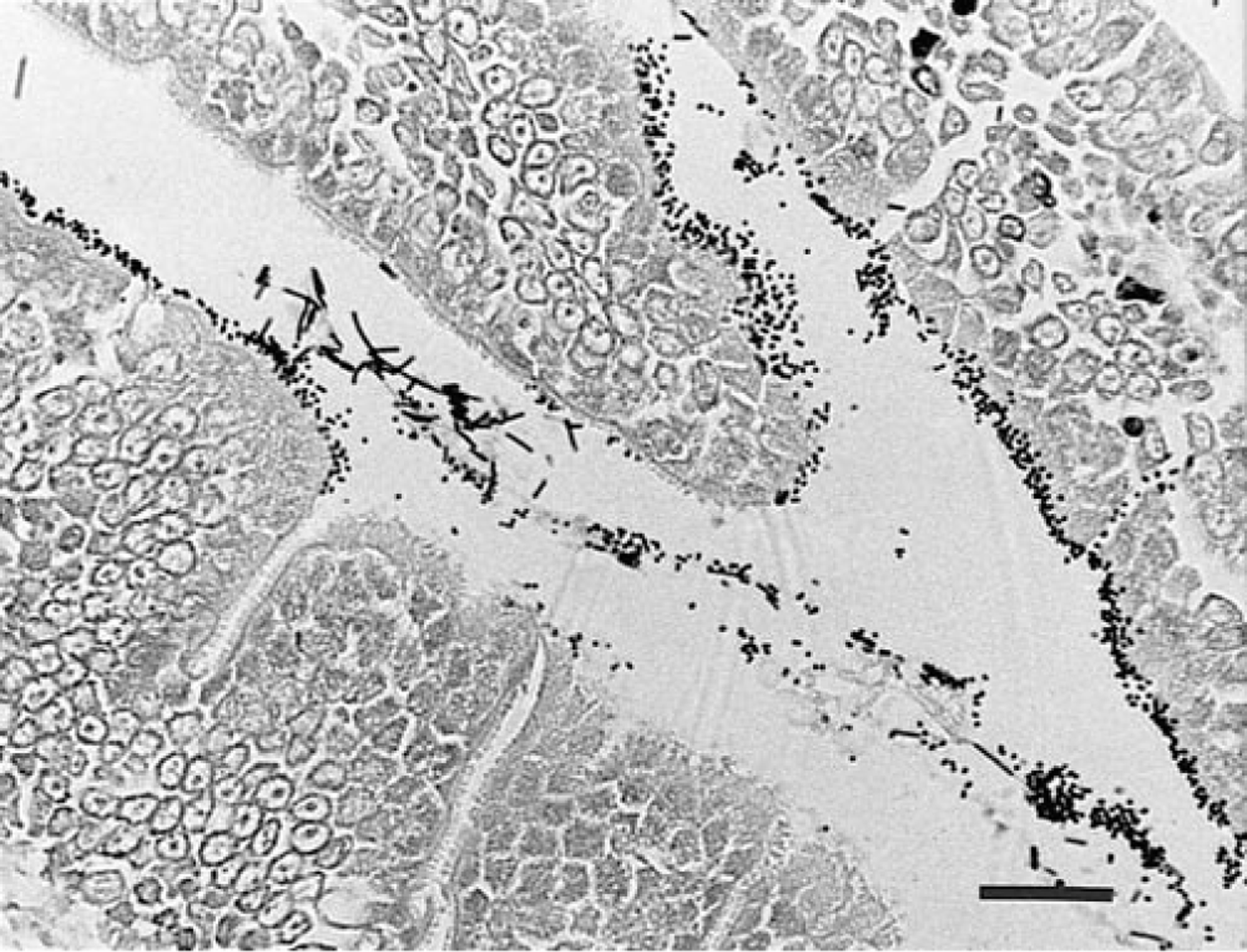
Jejunum; cat. Numerous Gram-positive cocci adhered to the brush border of villous enterocytes. Cocci are also present in the lumen, mixed with large bacilli (likely postmortem growth of normal flora). Gram stain. Bar = 250 µm.
In the liver (Fig. 2), numerous bile ducts showed inflammatory changes consisting of infiltration of ductal epithelium with neutrophils and lymphocytes, presence of luminal neutrophils, macrophages, and exfoliated epithelial cells, and periductal edema and inflammatory infiltration. In some areas, the changes were severe enough to obliterate the ductal architecture. In many affected ducts, Gram-positive cocci were observed, often adhered to the apex of epithelial cells. Similar bacteria also infiltrated some periportal bile canaliculi without associated inflammation.

Liver; cat. Cholangitis, associated with the presence of Gram-positive cocci in the ductal lumen. Gram stain. Bar = 200 µm.
In the pancreas, several pancreatic ducts were distended with luminal neutrophils. Ductal epithelial cells sometimes were exfoliated in the lumen among the inflammatory infiltrate, with Gram-positive cocci observed in association with the cells. Small numbers of neutrophils infiltrated the periductular stroma.
In the lung, an abundant proteinaceous fluid filled the alveolar lumina throughout most of the parenchyma. There was no evidence of pneumonia. No significant lesion was observed in the brain.
Samples of liver and lung were submitted for bacterial culture at the time of necropsy. Aerobic culture of the liver yielded abundant growth of alpha-hemolytic colonies. The isolate grew in the presence of 6.5% sodium chloride, had the capacity to hydrolyse esculin, and did not produce acid from arabinose, mannitol, raffinose, or sorbitol, but did produce acid from melibiose and sucrose. According to those characteristics, this isolate was identified as E. hirae. Escherichia coli was also isolated from the liver in smaller numbers. Culture of the lung also yielded small numbers of the same two isolates.
At the time this kitten was submitted for necropsy, feces from an adult female cat from the same cattery were submitted for bacteriological analysis. On a direct smear, the flora consisted predominantly of Gram-positive cocci. Culture yielded a large number of E. hirae. However, 5 weeks later, this bacteria could not be cultured from any of 15 adult or kitten fecal samples in the cattery.
Although culture of the intestinal tract was not performed in this case, the isolation of enterococci from liver and lung and the histological similarity of the bacteria observed in the different tissue sections make it a likely assumption that the bacteria adhered to the intestinal mucosa were enterococci as well. Enterococci have been associated with diarrhea in suckling animals of several species; in all reports, the histological findings in the intestine are similar to those of this case, with numerous enterococci adhered to the brush border, and mild or absent inflammation or structural changes to the enterocytes. The disease has been reproduced in foals and pigs by oral inoculation. 11 The mechanism of the diarrhea is unclear. The bacteria attach to the brush border with fimbriaelike structures, 11 but there is no structural damage to the brush border, and no enterotoxin production has been demonstrated. However, the infection does lead to a decrease in the activity of brush border digestive enzymes, suggesting maldigestion as a mechanism of diarrhea. 11 Mechanical interference with absorption has also been suggested. 1 The bacterial isolates have been reported variably as E. durans and E. hirae; however, using a revised identification scheme, 5 three isolates originally reported as E. durans were later re-classified as E. hirae. 4 The two species are closely related; E. hirae can be differentiated from E. durans by its positive melibiose reaction and usually also by its positive sucrose and alpha- and beta-galactosidase reactions. Recent work using molecular biology techniques confirms that the two are indeed genetically distinct species. 10 Recently, diarrhea associated with intestinal attachment of Enterococcus faecium has been reported in an adult cat, 7 suggesting that other species of enterococci may cause diarrhea in animals. Enterococcal diarrhea is probably underdiagnosed in veterinary medicine, because it is often nonlethal and transitory; in many of the reported cases, the lesions were observed in animals euthanatized for herd health monitoring 1 or in intestinal surgical biopsies. 8
It is unclear what factors lead to development of the disease in infected animals. E. hirae can be isolated from intestinal contents or anal swabs of normal adult animals of many species, including cats. 3 , 5 The young age of the animals affected suggests that there may be an age susceptibility, perhaps a vulnerability of enterocytes of juveniles to adherence by enterococcal fimbriae; however, intestinal attachment of enterococci has also been observed in adults. 8 Strain differences may also exist in the virulence of enterococci; the fact that this colony had recurrent problems in kittens and that the agent was isolated from a healthy adult suggests that a virulent strain may be carried chronically by adults and passed on to subsequent litters.
This kitten had extraintestinal lesions associated with the enterococcal infection. The pancreatic and hepatic bile ducts were invaded by enterococci, which appeared to adhere to the apex of epithelial cells and caused a suppurative inflammatory reaction. This infection was in all likelihood ascending, as indicated by the presence of enterococci within the lumen of the duodenal papilla. As both the common bile duct and the minor pancreatic duct open into the duodenal papilla, bacteria ascending through the papilla would be expected to lead to both pancreatic and biliary infections. Such lesions are not described in any of the other reports, but in those cases, the liver or pancreas were rarely examined. Ascending infections may be an important aggravating factor in animal death from enterococcal infections. The evidence of extension of the infection to the bloodstream (visible enterococci in hepatic sinusoids and isolation of E. hirae from the lung) indicates that a terminal bacteremia probably occurred, and the kitten's terminal neurological signs and death were probably due to septic shock.