
Abstract
Labrador Retrievers with elevated hepatic copper levels have been reported; however, it is unclear whether primary copper-associated hepatitis occurs in this breed. The objective of this study was to determine whether copper-associated hepatitis could be identified in Labradors by reviewing cases from the Diagnostic Center for Population and Animal Health, Michigan State University. Sixteen Labrador Retrievers (3 male, 12 female, and 1 of undetermined sex) between 4 and 11 years old, had multifocal and coalescing, centrilobular hepatitis characterized by macrophages with abundant intracytoplasmic copper and hemosiderin. Other lesions included multifocal, centrilobular and random, pigmented granulomas, hepatocellular necrosis, intrahepatic cholestasis, centrilobular or bridging fibrosis, and occasionally, pseudolobule formation. In rhodanine-stained sections, copper was concentrated in the cytoplasm of centrilobular and midzonal hepatocytes and in macrophages, which is consistent with copper-associated hepatitis. In 12 of the dogs, quantitative liver copper levels were available, and in all but 2 dogs the levels were greater than 2,000 parts per million dry weight (ppm dw). One dog had a liver copper level of 1,990 ppm dw and one dog with advanced hepatic cirrhosis had a level of 1,490 ppm dw. The findings suggest that primary copper-associated hepatitis likely occurs in Labrador Retrievers.
There are three causes of hepatic copper accumulation. First, a hereditary metabolic defect that inhibits biliary excretion of copper, resulting in hepatocellular lysosomal copper accumulation, has been shown to cause the primary form of copper storage disease in human beings (Wilson's disease), Long-Evans Cinnamon rats, toxic milk mice, and Bedlington Terrier dogs. 4, 6, 20, 21, 23, 28, 32 Altered biliary excretion of copper due to hepatic inflammation, fibrosis, and/or cholestasis is suggested to cause secondary copper storage disease, although this has not been definitively proven in the dog. 6, 9, 15, 18, 23 A third cause is excessive dietary intake. 6, 23, 29 In secondary copper storage disease, copper accumulation is mainly restricted to periportal areas and hepatic copper concentrations are usually less than 2,000 parts per million dry weight (ppm dw). 9, 15, 23 In proven primary hereditary copper storage disorders, copper accumulation is always centrilobular, and hepatic copper concentrations are usually greater than 2,000 ppm dw. 9, 10, 12, 15, 23, 26, 28 Breed-associated hepatic copper accumulation, with reports of copper concentrations greater than 2,000 ppm dw, has been identified in Bedlington Terriers, West Highland White Terriers, Skye Terriers, Dalmatians, Doberman Pinschers, and Labrador Retrievers.∗ In Bedlington Terriers, copper-associated hepatitis has been identified as an autosomal recessive disease. 11 A deletion in the COMMD1 gene (formerly MURR1) results in reduced biliary excretion of copper and marked accumulation of copper within hepatocytes. 5, 12, 18, 30 Ions act as catalysts for free radical formation, which cause cleavage of nucleic acids and oxidative damage to lipids and proteins, resulting in chronic hepatitis. 5, 7, 18, 28 A genetic mutation in copper metabolism has not been identified in any other canine breed; thus, the Bedlington Terrier is the only breed for which primary copper-associated hepatitis has been definitively proven. 5, 18 It remains to be determined whether Labrador Retrievers are affected by primary or secondary copper storage disease. 9, 17 A recent study supports primary copper storage disease in Labradors; however, no studies have been performed that quantify the amount of copper within affected livers of dogs of this breed. 9 The objective of this study was to determine whether primary copper-associated hepatitis occurs in Labrador Retrievers based on histologic lesions, degree of copper staining using a rhodanine stain, location of copper accumulation, and copper concentrations determined by inductively coupled plasma atomic emission spectroscopy.
Materials and Methods
A retrospective study was performed using archived data from case submissions to the Diagnostic Center for Population and Animal Health (DCPAH) in Lansing, Michigan, between 1 January 1985 and 9 May 2008. Cases were initially identified by electronically searching for biopsy and necropsy reports involving Labrador Retrievers for which sections of liver were histologically examined. The complete microscopic description and the available reported history were then reviewed, and any case with evidence of hepatitis, cirrhosis, nodular regeneration, and/or copper accumulation was selected for further evaluation.
The 44 cases fulfilling the aforementioned criteria were retrieved from the archives and routinely stained with HE and rhodanine stains. Two of the authors (T. Mullaney and R. Smedley) then examined these cases microscopically to more definitively classify them as suspected copper-associated hepatitis cases based on the findings of centrilobular hepatitis and centrilobular copper accumulation. The severity of copper accumulation was designated as mild, moderate, or marked, which corresponded to the staining grades 3, 4, and 5, respectively, as defined in a previous publication. 27 Four liver samples from Labradors with mild nonspecific hepatitis and minimal or no histochemical staining for copper were selected as controls.
Sixteen livers were histologically consistent with copper-associated hepatitis. Formalin-fixed, deparaffinized sections of liver from each of these 16 dogs and the 4 control livers were submitted for quantitative copper and iron analysis using inductively coupled plasma atomic emission spectroscopy (ICP-AES). 3 The procedures for deparaffinization and biopsy analysis have been previously published by Braselton et al. 2, 3 However, there was a slight modification in the biopsy analysis procedure. Briefly, the procedure of Braselton et al. 3 was followed with the exception that a newer, more sensitive instrument (Vista Axial ICP-AES, Varian Inc., Palo Alto, CA) with a standard cyclonic nebulizer was used instead of the ultrasonic nebulizer. This procedure is validated and is routinely used for simultaneous analyses of both formalin-fixed biopsy samples and deparaffinized specimens for quantifying calcium, copper, iron, and zinc according to standard operating procedures on file at the DCPAH. Because each one emits light at specific wave lengths characteristic of each element, ICP-AES is able to detect and simultaneously measure these elements.
Medical records that were available for the dogs in which copper-associated hepatitis was identified were gathered and reviewed for any information regarding signalment; clinical history; diagnostic test results, including clinicopathologic findings, gross findings, treatment plans; and case outcome.
Results
Sixteen dogs had histologic lesions and histochemical staining patterns consistent with copper-associated hepatitis. Liver sections from these dogs had multifocal to coalescing, centrilobular hepatitis (Fig. 1) characterized primarily by an infiltration of macrophages with abundant amounts of intracytoplasmic copper and hemosiderin (Fig. 2). Small numbers of neutrophils and other mononuclear inflammatory cells were also present in some sections. In addition, all cases had smaller, multifocal, centrilobular to random, pigmented granulomas with scattered individual necrotic hepatocytes (Fig. 3). Other findings included centrilobular to bridging fibrosis (8 dogs), lobular collapse (4 dogs), occasional pseudolobule formation (3 dogs), and nodular regeneration (3 dogs) (Fig. 4). Six cases also exhibited intrahepatic cholestasis. In Rhodanine-stained sections from these 16 affected dogs, copper was concentrated in centrilobular and midzonal hepatocytes and within Kupffer cells or other macrophage-type cells (Fig. 5). In HE-stained sections of liver from 4 dogs (dog Nos. 6, 9, 11, and 14) it was initially difficult to determine a pattern of hepatitis because of distortion of the lobular architecture by marked cirrhosis (dog Nos. 6 and 9), progression to cirrhosis with small section size (dog No. 11), and marked vacuolar change with small section size (dog No. 14). However, when rhodanine-stained sections were compared with HE-stained sections, the authors were better able to discern the lobular architecture and centrilobular pattern of the hepatitis and moderate to marked copper accumulation.
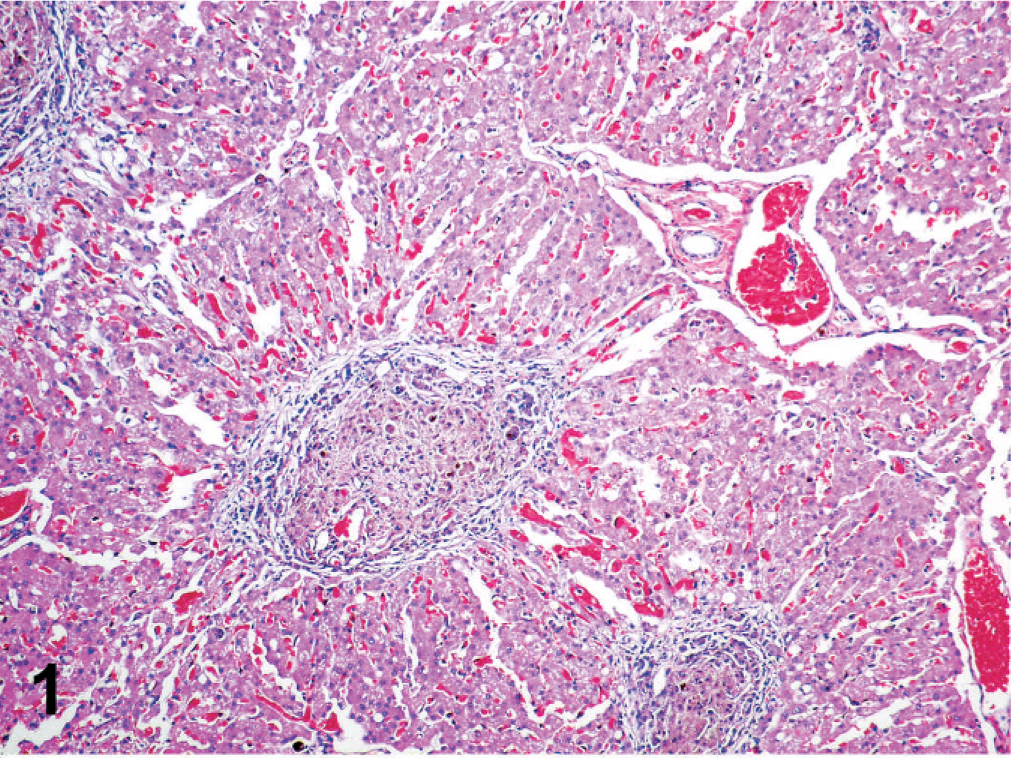
Canine liver; dog No. 4. There is multifocal to coalescing, centrilobular hepatitis. HE.
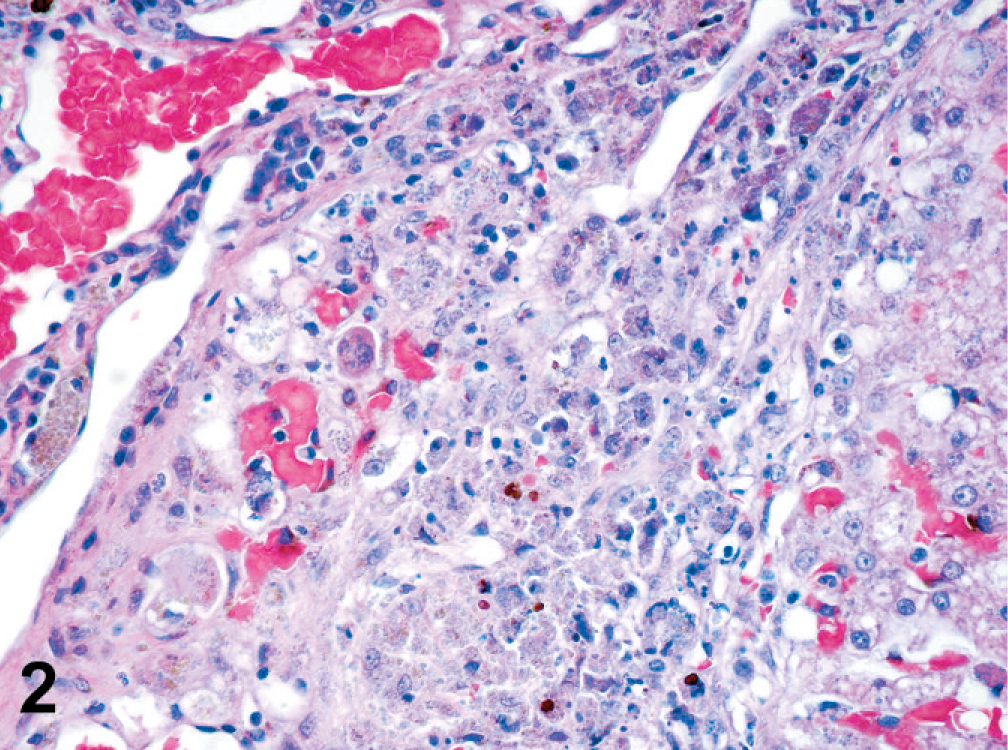
Canine liver; dog No. 4. The centrilobular hepatitis is characterized by an infiltration of macrophages with abundant amounts of intracytoplasmic copper and hemosiderin. Copper granules stain grey-blue. Hemosiderin is globular and stains golden brown. HE.
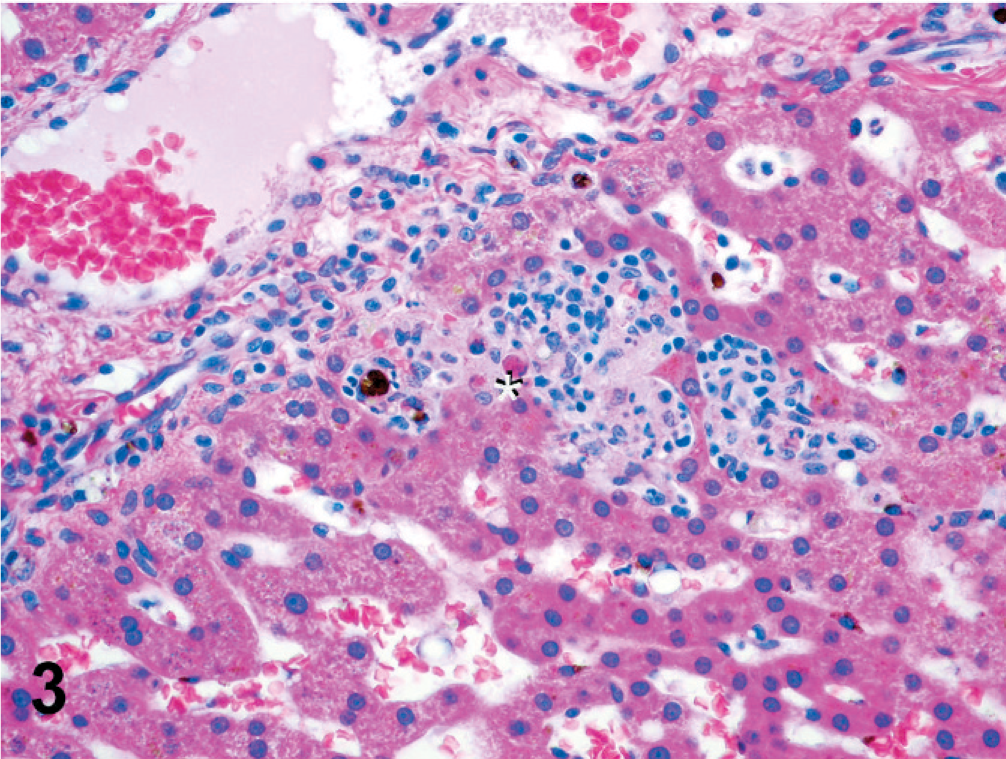
Canine liver; dog No. 8. There are multifocal, centrilobular pigmented granulomas with scattered individual necrotic hepatocytes. An asterisk is present just below a necrotic hepatocyte. HE.
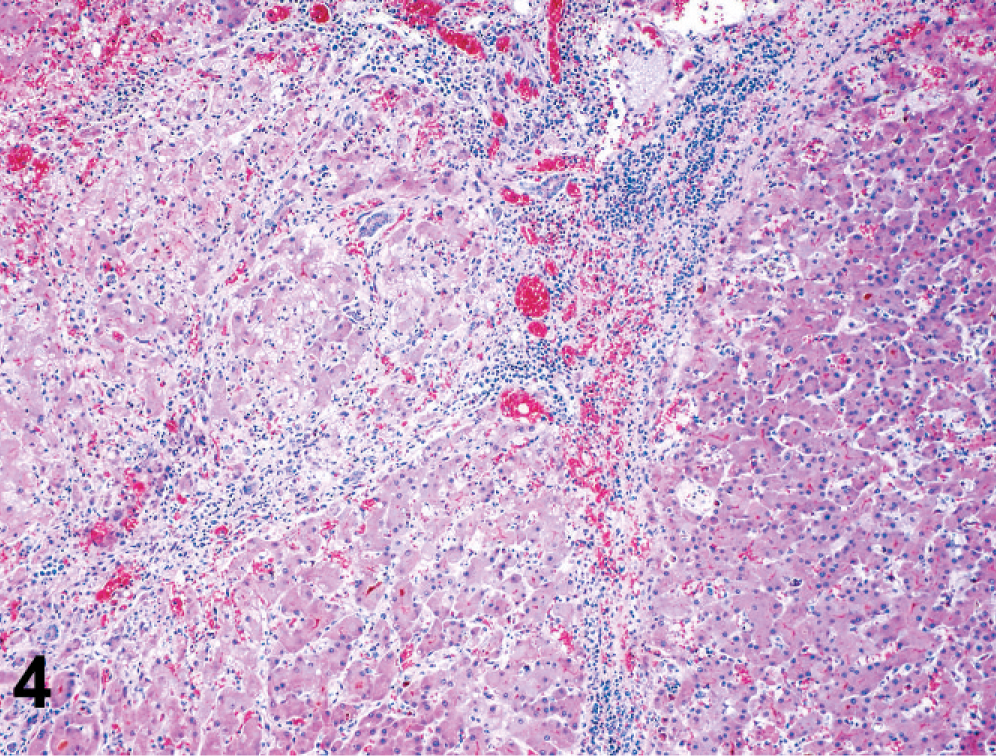
Canine liver; dog No. 6. There is centrilobular to bridging fibrosis, lobular collapse, and occasional pseudolobule formation and nodular regeneration. HE.
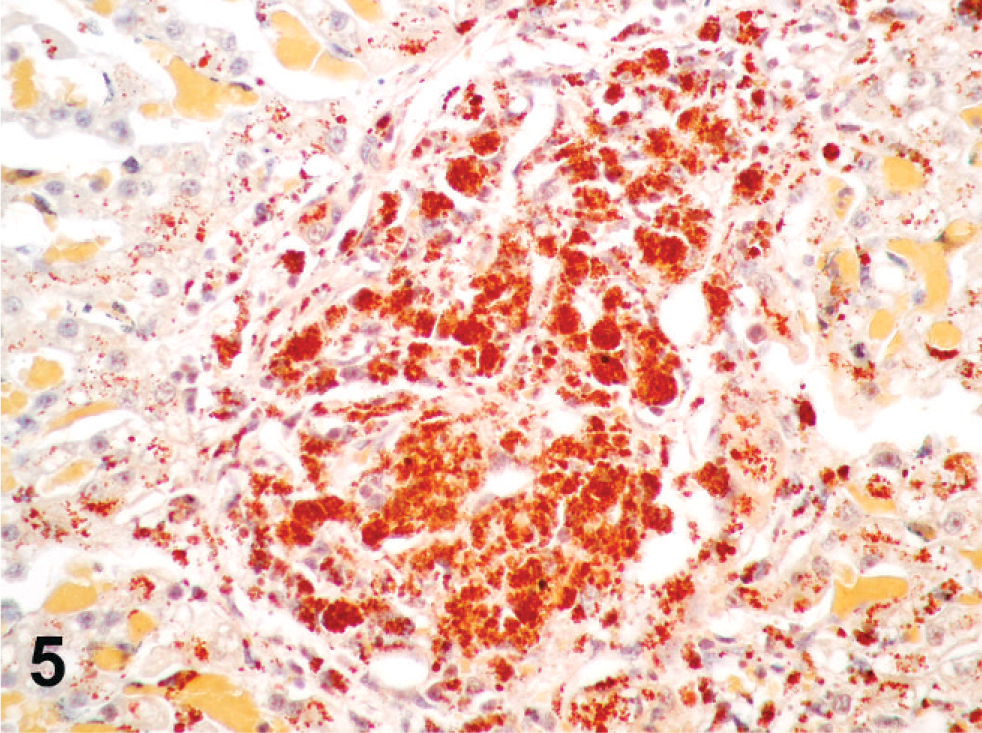
Canine liver; dog No. 4. Copper is concentrated in the cytoplasm of centrilobular and midzonal hepatocytes as well as within Kupffer cells or other macrophage-type cells. Rhodanine.
Quantitative hepatic copper concentrations were determined for 16 of the 20 submitted cases (Table 1). The remaining four cases (dog Nos. 11, 12, 13, and 14) did not have enough liver available for quantitative analysis. Of the 12 livers with lesions of primary copper-associated hepatitis that were able to be analyzed, 10 had copper levels greater than 2,000 ppm dw, with a range of 2,375 to 4,972 ppm dw and a mean of 3,369 ppm dw (reference interval 120–400 ppm dw). The eleventh liver (dog No. 9) had a copper level of 1,490 ppm dw and histologically exhibited marked cirrhosis. The twelfth liver (dog No. 16) had a copper level of 1,990 ppm dw, and this dog did not exhibit clinical signs of liver disease at the time of liver biopsy. The four control livers had copper levels between 163 and 345 ppm dw, which is in agreement with the reference interval. Among the 12 dogs with lesions of copper-associated hepatitis and enough liver available for quantitative analysis, 11 dogs also had elevated iron levels (Table 1) with a mean of 4,117 ppm dw (reference interval 350–1,750 ppm dw).
Labrador Retrievers with copper-associated hepatitis.
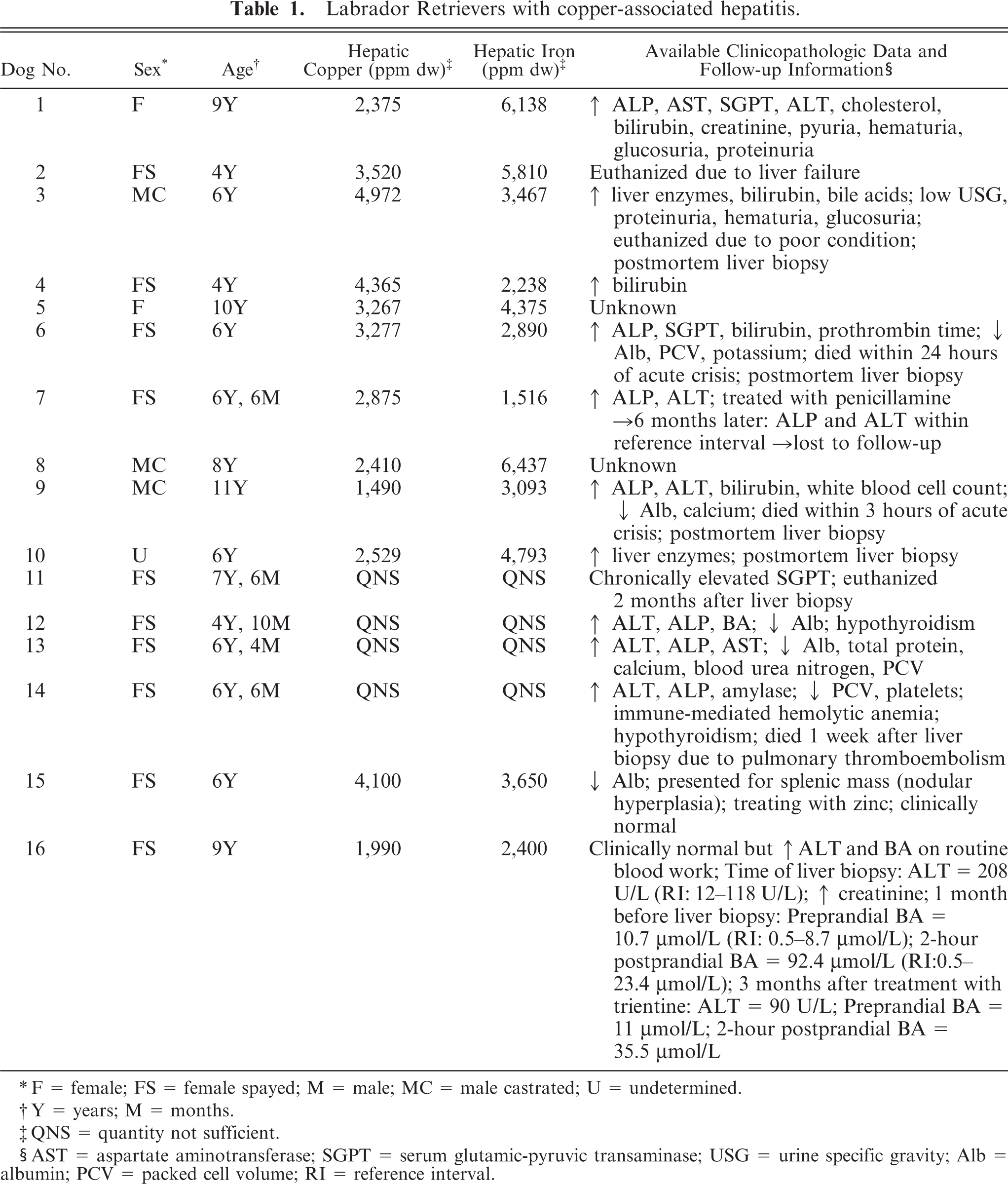
∗ F = female; FS = female spayed; M = male; MC = male castrated; U = undetermined.
† Y = years; M = months.
‡ QNS = quantity not sufficient.
§ AST = aspartate aminotransferase; SGPT = serum glutamic-pyruvic transaminase; USG = urine specific gravity; Alb = albumin; PCV = packed cell volume; RI = reference interval.
Available medical record information was reviewed for the 16 affected dogs. Signalment information is listed in Table 1. Results from available data indicated that anorexia (n = 7) and vomiting (n = 6) were the two most common presenting clinical signs in affected dogs. Two of the dogs (dog Nos. 15 and 16) did not exhibit any clinical signs of liver disease at the time of diagnosis. Elevated alkaline phosphatase (ALP) and alanine aminotransaminase (ALT) were the most common abnormal clinicopathologic findings in all dogs. Other clinicopathologic abnormalities are listed in Table 1. Reported gross findings ranged from microhepatica to hepatomegaly with or without multifocal hepatic nodules and/or mottling. Available follow-up information is listed in Table 1 as well.
Discussion
A total of 16 dogs were initially diagnosed with primary copper-associated hepatitis based on centrilobular hepatitis and moderate to marked rhodanine staining in centrilobular areas. Of these 16 dogs, 10 had hepatic copper levels greater than 2,000 ppm dw (range, 2,375–4,972 ppm dw). One of these 16 dogs (dog No. 9) had a copper level of 1,490 ppm dw but had marked hepatic cirrhosis. The proliferation of scar tissue during the development of cirrhosis dilutes the hepatocyte copper resulting in an apparent decrease in hepatic copper concentration. 23, 25 Also, regenerative nodules within cirrhotic livers do not accumulate copper. 23 Dog No. 16 had a liver copper level that was very close to 2,000 ppm dw and measured 1,990 ppm dw. This dog did not exhibit any clinical signs of liver disease. The 4 remaining dogs did not have large enough liver samples available for quantitative analysis. Histologic findings in affected dogs included multifocal to coalescing centrilobular hepatitis characterized primarily by an infiltration of macrophages with abundant amounts of intracytoplasmic copper and hemosiderin. Small numbers of neutrophils and mononuclear inflammatory cells were also present. In addition, all cases had smaller, multifocal, centrilobular and random, pigmented granulomas with scattered individual necrotic hepatocytes. Other findings included centrilobular to bridging fibrosis, lobular collapse, occasional pseudolobule formation, nodular regeneration, and intrahepatic cholestasis in many cases. Based on the centrilobular location of the inflammation and copper accumulation, the degree of rhodanine staining, and quantitative hepatic copper levels greater than 2,000 ppm dw, the authors conclude that copper-associated hepatitis in Labrador Retrievers is consistent with a primary form of copper storage disease. To conclusively state that primary copper storage disease occurs in Labradors, however, a genetic defect in copper metabolism needs to be identified.
These conclusions support those in a recently published study in which 15 Labradors were retrospectively diagnosed with copper-associated chronic hepatitis based on histopathologic and rubeanic acid stains showing primarily centrilobular copper accumulation and inflammation. 9 Sections of liver from those dogs also exhibited varying degrees of hepatocellular apoptosis and necrosis, mononuclear inflammation, regeneration and fibrosis. 9 However, that study did not confirm the diagnoses with quantitative copper analysis. Instead, the researchers determined quantitative hepatic copper levels in 8 clinically normal Labradors that were related to 2 of the 15 affected dogs. 9 Those 8 dogs had quantitative copper levels ranging from 402 to 2,576 ppm (mean, 1,317 ppm) and, histologically, copper was present in centrilobular areas. 9 These dogs were judged to have subclinical copper accumulation. Based on the centrilobular accumulation of copper in affected and related dogs, and the elevated copper levels in subclinical relatives of the affected dogs, the researchers concluded that copper-associated hepatitis is familial and most likely caused by an inherited genetic defect in the Labrador Retriever, but the genetic defect remains to be elucidated. 9 In the present study, none of the affected Labradors were known to be related. However, 2 Labradors with copper-associated hepatitis were recently identified as littermates. The findings of the present study confirmed that 10 of 12 affected dogs for which large enough sections of liver were available did indeed have hepatic copper levels greater than 2,000 ppm dw, a criterion that is generally accepted in the current literature as indicative of a primary form of copper storage disease, in conjunction with centrilobular hepatitis. 9, 15, 23 In Hoffman 9 and the current study, age distribution, sex ratios, gross lesions, the most commonly identified clinical signs (anorexia and vomiting), and clinicopathologic findings (elevated liver enzymes) were comparable. An interesting finding is the predominance of affected female dogs compared with male dogs. In the Hoffman study, 9 11 of the affected 15 dogs (73.3%) were female, and in the current study, 12 of 15 (80%) dogs with a known gender were female. At this time, sample sizes are too small to speculate on a sex-linked inheritance, and complete pedigrees are not available. Two dogs (dog Nos. 15 and 16) in the current study were diagnosed with copper-associated hepatitis but did not exhibit any clinical signs of liver disease. One of these Labradors had a hepatic copper level of 4,100 ppm dw (dog No. 15) and the other had a hepatic copper level of 1,990 ppm dw (dog No. 16).
Currently, it is unknown why copper can accumulate without causing hepatitis or clinical signs of liver disease, in Labradors. In one study, Bedlington Terriers with a deletion in the COMMD1 gene had hepatic copper accumulation by 1 year of age, but there were no histologic lesions of hepatitis until 2 years of age (cited by Hoffman 9 ). In that study, it was suggested that there was a prolonged delay period before lesions were seen. One suggested hypothesis was that the storage and accumulation of the nontoxic form of copper may occur in both affected and related Labradors until protective cellular systems are exhausted or there is an additional stress factor resulting in oxidative damage by occasional free reactive copper and subsequent hepatitis. 9
Another interesting finding was the elevated hepatic iron levels in 11 of 12 affected dogs. This sequestration of iron may simply be secondary to chronic inflammation or it may be directly related to the suspected abnormal copper metabolism, depending on where the defect lies in the copper absorption and excretion pathways. In one study using dogs of various breeds, it was found that dogs can have a wide range of hepatic iron concentrations and liver copper concentrations were reported to increase as liver iron concentrations increased; however, they did not appear to increase in direct proportion to each other. 16 This study also stated that if a dog has clinically normal hepatic copper levels, the hepatic iron will either be normal or increased, but if the hepatic copper concentration is high, the hepatic iron concentrations will most likely be high as well. 16 In addition, both hepatic iron and hepatic copper concentrations were significantly higher in dogs with an abnormal histologic grade and were often associated with inflammation. 16 Whether iron, an oxidant, interacts with copper to contribute to the lesions seen in these dogs is currently unknown. Hemolytic anemia is generally not a sequel to copper storage disease in most breeds of dogs. One dog (No. 14) in this study had been previously diagnosed with immune-mediated hemolytic anemia (IMHA). Unfortunately, a large enough liver sample was not available from this dog for quantitative analysis.
Based on the results of this study and the study by Hoffman et al., 9 primary copper-associated hepatitis should be considered in Labrador Retrievers with clinical and/or histologic signs of liver disease so that appropriate therapy can be implemented. The prognosis for affected Labradors is uncertain; however, there is evidence to suggest that chelation therapy can be curative. 9 In the Hoffman et al. study, 9 5 dogs treated with penicillamine had resolution of clinical signs and histopathologic lesions; one patient treated with penicillamine had a histologic and clinical “cure” and penicillamine was stopped. 9 This dog developed clinical disease within 1 year of treatment cessation but was again responsive to penicillamine. No additional follow-up information was available for the one dog in the current study that had been treated with penicillamine. At the time of writing, one of the most recently diagnosed dogs (No. 15) in the study had begun chelation therapy with zinc and reportedly was “doing well.” The other recently diagnosed dog (No. 16) was being treated with trientine and was going to begin zinc treatment soon. This dog has also remained clinically normal and, as listed in Table 1, ALT and post-prandial bile acid values have decreased since beginning treatment.
The authors conclude that primary copper-associated hepatitis does occur in Labrador Retrievers based on the described histologic lesions, centrilobular pattern of inflammation and copper accumulation, degree of copper staining with a rhodanine stain, and quantitative copper levels in affected dogs that were greater than 2,000 ppm dw; however, a genetic defect remains to be elucidated. Primary copper-associated hepatitis can be diagnosed by routine HE and rhodanine staining of liver sections, but quantitative determination of hepatic copper levels is recommended to confirm this diagnosis. It is also possible for affected dogs to have elevated quantitative hepatic copper levels that are less than 2,000 ppm dw if significant cirrhosis is present. In this situation, there must still be evidence of primarily centrilobular inflammation and copper accumulation to warrant a diagnosis of copper-associated hepatitis. Again, the prognosis for copper-associated hepatitis in Labradors is uncertain at this time; however, preliminary data suggests that chelation therapy is beneficial. A response to chelation therapy is also consistent with a primary form of copper storage disease in this breed. 15 Based on the results of this study, future directions include obtaining fresh liver samples from affected Labradors to identify the suspected genetic defect in copper metabolism. Also, it is hoped that this study will aid in the early recognition of copper storage disease and subclinically affected Labradors so that, with treatment, survival intervals will improve.
Footnotes
Acknowledgements
We would like to acknowledge the histology and toxicology laboratories at the Diagnostic Center for Population and Animal Health for technical support and Dr. Matti Kiupel for assistance with photomicrographs. We also thank the referring veterinarians who provided us with clinical and follow-up information.