
Abstract
Purpose
Clavicle fractures are treated conservatively in the paediatric age group, except in rare types of fractures. We investigated whether there was a difference between using shoulder-arm sling and figure-of-eight bandage in this age group.
Methods
This study was designed as a retrospective study. In all, 41 children among 53 who underwent conservative treatment with a shoulder-arm sling or figure-of-eight bandage between 2014 and 2019 were included in the study and divided into two groups. Treatment results were compared clinically with respect to pain intensity, muscle strength and radiological examinations.
Results
Group A comprised 20 children with a figure-of-eight bandage and group B comprised 21 children with shoulder sling. According to the Robinson classification, ten fractures were displaced in group A and 12 in group B (p = 0.647). The mean time until the first appointment after the index visit that started the management course was 25.5 days (21 to 31) in group A and 24 days (20 to 30) in group B (p = 0.129). Fracture healing was observed in all patients at the first follow-up and the treatment was discontinued. There was no difference between the groups in the muscle strength examination and shoulder joint range of movement examination at the first-year follow-up (p = 1.00).
Conclusion
In the paediatric age group, there was no significant difference between shoulder-arm sling and figure-of-eight bandage in the conservative treatment of clavicle fractures. Since the shoulder-arm sling is more suitable for treatment, it may be the primary preference.
Level of Evidence
Level III (retrospective comparative study)
Introduction
Clavicle fractures constitute approximately 10% to 15% of all paediatric fractures. 1 Although conservative methods are prominent therapeutic options, the tendency for surgical treatment increases in the adolescent age group. The optimal management of adolescent clavicle fracture is controversial. Nonunion of adolescent clavicle fracture is extremely rare, and treatment is usually focused on prevention of symptomatic malunion. Misunions in adolescent clavicle fractures may not lead to as large deficits as in adults, however, high-level evidence is needed to support this conclusion.2–8 Successful results with surgical treatment have been reported in children older than ten years with respect to better analgesia and an earlier range of movement in clavicle fractures. Recent studies have shown that surgery has the advantage of early union and early return to activity but is associated with higher rates of reoperation and complications than conservative methods. However, the need for surgical treatment is extremely low under the age of ten years.9–12
Although different opinions are suggested for the indications for surgical treatment, open fractures, neurovascular lesions and the occurrence of skin defects are considered the agreed surgical criteria.13,14 Complications such as malunion and union from non-surgical treatment are rare, but the risk increases with increasing age in adolescent patients.4,15
The two most commonly used methods in conservative treatment are arm sling and figure-of-eight bandage. 16 While some surgeons prefer shoulder-arm sling for conservative treatment, others prefer figure-of-eight bandages.17–19 However, studies have indicated that the wearing comfort of the shoulder-arm sling is higher than the figure-of-eight bandage.16,20 Although previous studies have compared surgical treatment with conservative treatment options, 20 to our knowledge, no study yet has compared the results of these two conservative treatment options in clavicle fractures in the paediatric age group.
Therefore, we compared the radiological and clinical results of the figure-of-eight bandages and the shoulder-arm sling that are used in the conservative treatment of paediatric clavicle fractures.
Materials and methods
This study was designed as a retrospective study. The data of 53 paediatric patients who were treated for clavicle fractures in our hospital between 2014 and 2019 were retrospectively analyzed from the hospital's medical archives. The ethics committee for our hospital approved the study (01.07.2021-E.47765).
The following inclusion criteria were applied: age less than ten years, patients should have been treated conservatively, followed by the application of shoulder-arm sling or figure-of-eight bandage. Patients with a follow-up period of < 12 months (n = 7), pathological fractures (n = 1), open fractures (n = 1) and fractures with neurovascular injuries (n = 1) were excluded from the study. Fractures were classified according to the Allman 21 and Robinson 22 classifications. Patients were divided based on whether they were treated with a shoulder-arm sling or figure-of-eight bandage. The treatment method was made according to the choice of the surgeon responsible for the emergency treatment. In the first week follow-up, it was observed that the selected treatment was applied and intensive recommendations were made for its reuse. All patients carefully adhered to the administration of the chosen treatment (shoulder-arm sling or figure-of-eight bandage). The sling or bandage used was removed at the outpatient clinic after three weeks of treatment. In total, 12 patients showing treatment non-compliance were excluded from the study.
Group A
Patients treated with figure-of-eight bandages were included in this group. No manoeuvres were made for reduction during wrapping the figure-of-eight bandage. These bandages were recommended to be used continuously for three weeks, even during bathing and sleeping.
One week later, the patients were invited to the outpatient clinic to check the use of bandages. The families were shown how to check the bandage and tighten it when necessary. At the first follow-up three weeks later, the bandage application was ended by evaluating the radiographic images (Fig. 1).
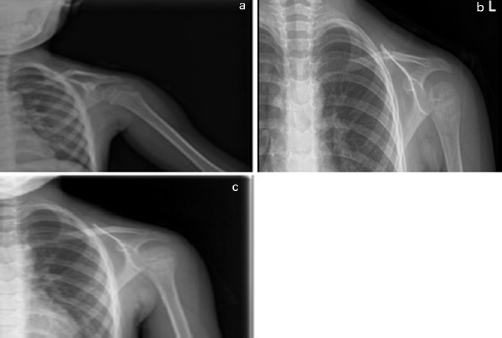
A seven-year-old boy with figure-of-eight bandages applied: a) day 1; b) day 21; c) week 24.
Group B
Patients who were followed up with a shoulder sling were included in this group. The upper extremity was immobilized in internal rotation by wearing a standard shoulder-arm sling starting from the damaged extremity elbow and going from the back to the opposite shoulder in all children. One week later, patients were invited to the outpatient clinic to check their use. After three weeks of continuous use, plain radiographic images were evaluated and the use of the sling was discontinued (Fig. 2).
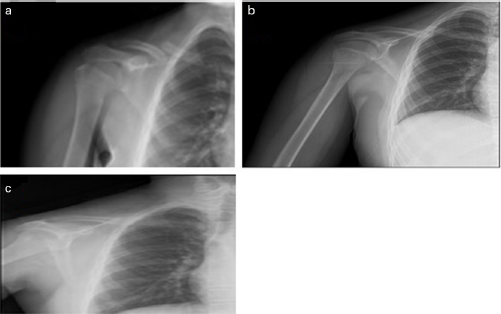
A nine-year-old boy followed up with a shoulder-arm sling: a) day 1; b) day 23; c) week 24.
Treatment and follow-up
The same non-steroidal anti-inflammatory syrup was given to all patients by calculating the doses according to patients’ weight. The drug treatment was discontinued after regular use for a week. Afterward, the same rehabilitation procedures were applied to both patient groups. The physical therapy protocol applied to the shoulder of the fractured side of the patients was completed when the joint range of movement of the contralateral shoulder was reached. Simple stretching and pendulum exercises that patients can perform at home for half an hour a day were suggested. The patients were followed up by the trauma resident.
Patients were compared clinically with respect to pain intensity and radiographic imaging at their third-week follow-up. The painless fracture line palpation and the appearance of callus tissue on direct radiography were evaluated as fracture healing. At the first-year follow-up, the muscle strength and range of movement of the patients were compared with the unoperated extremity. Radiographic images were not obtained at the end of the treatment to avoid unnecessary radiation exposure. Muscle strength examination was performed according to the Oxford/Medical Research Council Grading Scale 23 . The range of movement was evaluated using the Neutral Zero Method 24 .
Statistical analysis
SPSS 21.0 statistics programme (IBM Corporation, Armonk, New York) was used in our study. Normality of distribution was evaluated using the Kolmogorov-Smirnov and Shapiro-Wilk tests. Normally distributed data were evaluated using independent samples t-test and Mann-Whitney U test. Pearson's correlation test and Fisher's exact test were used for correlation analysis. A p-value < 0.05 was considered to indicate statistical significance.
Results
A total of 41 patients were included in the study. Group A comprised 20 children (12 boys and eight girls) treated with figure-of-eight bandage, and Group B (13 boys and eight girls) comprised 21 children treated with shoulder-arm sling (p = 0.901) (Table 1). The mean age of group A was 5.5 years (2 to 9), and the mean age of group B was five years (3 to 9) (p = 0.744) (Table 2).
Distribution of categorical variables of fractures according to groups
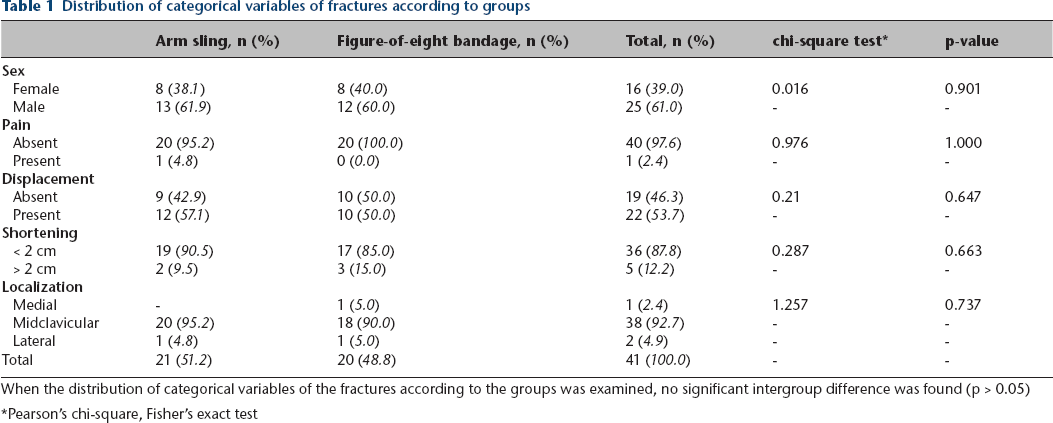
When the distribution of categorical variables of the fractures according to the groups was examined, no significant intergroup difference was found (p > 0.05)
Pearson's chi-square, Fisher's exact test
Continuous variables distribution of fractures by groups

When the distribution of continuous variables of the fractures according to the groups was examined, no significant intergroup difference was found (p > 0.05)
independent sample t-test, Mann-Whitney U test
According to the Robinson classification, ten fractures were displaced and ten fractures were non-displaced in group A, while 12 and nine fractures were displaced and non-displaced in group B, respectively (p = 0.647). In group A, the displacement of fracture was < 2 cm in 17 children, while it was > 2 cm in three children (Table 1). In group B, 19 and two children had < 2 cm and > 2 cm shortening of the clavicle, respectively.
According to the Allman classification, in group A, one fracture was in the medial region, 18 in the midclavicular region and one in the lateral region, respectively. In group B, 20 fractures were located in the midclavicular region and one in the lateral region (p = 0.737). The mean time until the first follow-up was 25.5 days (21 to 31) in group A and 24 days (20 to 30) in group B (p = 0.129) (Table 2).
Fracture healing was observed in all patients at the first control, and the use of shoulder-arm sling or figure-of-eight bandage was discontinued. No significant difference was found between the groups in the muscle strength examination performed at the first-year follow-up (p = 1.00).
The amount of limitation in shoulder range of movement was evaluated in the first year and no significant difference was found between the groups (p = 1.00).
Discussion
Clavicle fractures are common in the paediatric age group. 1 Although the frequency of complications increases with age, the tendency for surgical treatment also increases, especially in the adolescent age group. However, conservative treatment is still the preferred option in children.2–8,25
Although figure-of-eight bandages and shoulder-arm sling are used frequently in clavicle fractures among conservative treatments, few studies have compared the superiority of both methods. 26
Patients who were treated for clavicle fractures in the pre-adolescent period and followed up with a shoulder-arm sling or figure-of-eight bandage were included in our study. There was no significant difference between the two groups in terms of fracture union and clinical complications. This result might be due to an underpowered study. With these results, it was concluded that the shoulder-arm sling in the paediatric age group can be preferred primarily in terms of compliance with treatment and patient satisfaction.
Although clavicle fractures are quite common in the paediatric age group, there are not enough studies specifically conducted in this age group. In childhood, the periosteal sheath is thicker and the bone structure is softer and more flexible than in adults. In a study by Pavone et al, 27 clinical and radiological healing in clavicle fractures was shown to be associated with age, and it was emphasized that better results were obtained especially in those aged less than eight years. Similarly, children between the ages of two and nine years were evaluated in our study, and clinical and radiological improvement was observed in all patients at the first control. In a study involving 101 children in which paediatric clavicle fractures were evaluated, the results showed that conservative treatment was satisfactory, especially in children aged less than ten years of age, and that surgical treatment was a better option for older children depending on the level of displacement of the fracture. 28 Similarly, in Labronici et al's 29 study of ten children aged five to 11 years with a clavicle fracture, the only 11-year-old patient underwent surgical treatment, while others successfully recovered with conservative treatment. All patients examined in our study were aged younger than ten years and had clavicle fractures. Conservative treatment was applied to these patients regardless of the fracture type, extent of clavicle shortening and displacement. There were no complications such as nonunion or limitation of movement.
Our study supports the fact that conservative choices are the primary treatment option for children aged under ten years, regardless of the fracture type. In our study results, no significant difference was found between the two conservative treatments in terms of efficacy confirming the literature. In a 2011 study comparing shoulder-arm sling with figure-of-eight bandages, no difference was found between the two treatments in terms of development of clavicle shortening, pain, function, range of movement and strength. 30 Similarly, in other studies comparing shoulder-arm sling and figure-of-eight bandage treatment options, no significant difference was found between the two groups in terms of clinical and radiological improvement, however, the use of figure-of-eight bandage is more difficult for children and their families.16, 20, 31, 32
Calder et al 33 reported that there is no need for follow-up after the initial examination in childhood clavicle fractures, as complications are extremely rare in isolated and uncomplicated fractures. However, publications are reporting nonunion in children accompanied by conditions such as genital anomalies, vitamin D deficiency, neurofibromatosis and congenital pseudoarthrosis. 34
In our study, children with < 2 cm fracture displacement were included. Considering the union potential of the paediatric age group, nonunion or limitation in joint movements did not develop. None of the patients in our study had comorbidities, and no complications were observed, consistent with existing publications.
This study has some limitations. First is the retrospective design of the study and the small sample size. Evaluation of only a limited age group of children was considered as an advantage. After the treatment method was applied, the patients’ treatment compliance was carefully evaluated in the control examinations. All patients who were thought to not comply with treatment were excluded from the study. Therefore, it was not possible to interpret whether similar results will be obtained without using sling-arm or figure-of-eight bandages. Second, radiographs were not obtained when the treatment was terminated, although this was done to avoid unnecessary radiation exposure.
In conclusion, the conservative approach is the preferred treatment option of clavicle fractures in children before puberty. In our study, the radiological and clinical results of shoulder-sling and figure-of-eight bandage, which are the most preferred conservative treatment options, were evaluated, and no significant difference was found between the two groups. The shoulder-arm sling is easier to apply and manage in the paediatric age group and hence seems to be more advantageous than the figure-of-eight bandage in treatment selection.
Footnotes
CP: Design, Data analysis.
ACC: Data acquisition.
SK: Data analysis.
EC: Data acquisition and interpretation.