
Abstract
Abstract
Purpose
Primary pyomyositis in immunocompetent children in non-tropical regions (countries with temperate climates) is very uncommon. It is rarely found in the intrapelvic muscles, and even more rarely in the obturator muscles. We try to draw attention to the potential occurrence in these conditions.
Methods
Five new cases of primary obturator-muscle pyomyositis in immunocompetent children aged between 6 and 11 years in a temperate climate are presented. They present with symptoms as follows: fever, pain (thigh, abdominal, inguinal, and/or hip pain), and limp. Three of them had no hip movement limitation. All of them had tenderness in the perineum zone.
Results
Laboratory tests may reveal high erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) counts, but depend on the length of diagnostic delay. The evolution time oscillated from 1 to 5 days. Fever and limp disappearance depends on the evolution time previous to the onset of the antibiotics administration. In 4 out of 5 patients, Staphylococcus aureus was present in the blood cultures. In all cases of obturator-muscle pyomyositis, diagnosis was confirmed using computed tomography (CT) scan (one) and/or magnetic resonance imaging (MRI) (four).
Conclusions
Obturator-muscle pyomyositis is aimed at emphasizing the diagnostic difficulties associated with the condition, due to its deep location and to the fact that the disease presents with multiple manifestations that may initially cause confusion, since they mimic other conditions occurring in the abdomen, hip (septic arthritis, osteomyelitis), spine, etc. The diagnosis is only confirmed using CT scan and/or MRI. In the five patients with antibiotics treatment, the condition resolves without sequelae, even at long-term follow-up.
Introduction
Pyomyositis is a primary infection of striated muscle. Muscle infections may be primary or secondary to neighboring or even remote infectious processes. Primary conditions are not uncommon in tropical regions, but are very rare in countries with temperate climates [1, 2]. The incidence of pyomyositis is on the increase worldwide among children and adults [3]. It is, therefore, essential to consider this uncommon infection when facing septic processes associated with sciatica or with inguinal, gluteal, or abdominal symptomatology. When it involves muscles around the hip, the condition must be differentiated from septic arthritis and transient synovitis, among other diseases, since reactive hip effusion normally develops. Lack of awareness of the condition frequently leads to delays in correct diagnosis.
The most common form of pyomyositis is secondary to other pathological processes (sacroiliitis, spondylodiscitis, etc.). Primary pyomyositis in immunocompetent children in non-tropical regions (i.e., countries with temperate climates) is very uncommon. It occurs more frequently in young adults with predisposing factors, which may be either patient-dependent (drug abuse, alcoholism, AIDS, and other conditions producing immunodepression) or muscle-dependent (excessive physical exercise, direct muscle trauma, parasite infections, viral myositis, etc.). It is rare in older people, in whom it is usually associated with diabetes [4]. Its most frequent anatomic locations are the quadriceps muscle (26.3 %) and the iliac psoas muscle (14 %) [5, 6].
Deep pelvic infections involving the psoas, the iliacus, the piriformis, and the obturators can be a significant cause of morbidity and mortality [7]. Due to its rarity, obturator pyomyositis is scantly mentioned in the orthopedic literature [7, 8]. It is rarely found in the intrapelvic muscles and even more rarely in the obturator internus and/or obturator externus muscles. They originate from the anterolateral and posterolateral wall of the pelvic cavity, surround the obturator foramen, ending in a tendinous band across the posterior capsule of the hip joint and attached to the medial surface of the greater trochanter. Simons et al. [9] reported the importance of understanding the distinction between the retroperitoneal and retrofascial potential spaces. The intrapelvic location of these muscles makes clinical diagnosis difficult. The diagnosis of rare and deep infections involving the peripelvic muscles requires a thorough clinical examination, together with a high rate of suspicion.
The main objective of this paper is to draw attention to the potential occurrence of primary pyomyositis of the obturator muscles, a serious and life-threatening condition, in immunocompetent children in countries with a mild climate. This is the largest presentation of obturator pyomyositis reported in immunocompetent children in temperate-climate countries. We also aim to heighten awareness by presenting our experience with five cases of this uncommon infection, all of which occurred over a short period of time.
Clinical cases
Four of the patients were admitted to hospital between 2004 and 2006 and one in 2009 (Tables 1 and 2). The patients were unrelated in terms of blood ties, place of residence, school they attended, physical activity, and social and economic status of the family. None of them had an underlying disease or a compromised immune system. None of them had prior history of trauma, abrasions, skin lesions, or bites. All of the patients live in Navarre (northern Spain), a temperate-climate region.
Clinical data of the five patients
Clinical data of the five patients
Case 1
An 11-year-old girl who was admitted to another hospital following 2 days of fever (39 °C) and pain in the abdomen and the right hip, weight-bearing inability, but normal rotation of the hip. Three days later, she was referred to us with persistent spikes of fever, pain in the right iliac fossa, and swelling in the medial region of the right hip. She was diagnosed with possible appendicitis or an intra-abdominal abscess. Ultrasound examination showed an accumulation of fluid in the obturator externus muscle, which was compatible with an abscess relating to coxofemoral joint effusion. Puncture of the hip joint produced 1 cc of serous articular liquid, which was cultured with negative results. Magnetic resonance imaging (MRI) was not available at the time and a computed tomography (CT) can was performed. The CT scan showed signs of inflammation of the obturator internus muscle (Fig. 1). The patient's fever remitted gradually, and disappeared completely 6 days after admission. The patient was treated with cloxacillin (1.5 g/6 h) and cefotaxime (1 g/8 h) for 10 days, and gentamicin (240 mg/24 h) for 7 days. Oral treatment with cloxacillin was continued until her C-reactive protein (CRP) value returned to normal. Seven and a half years later, the patient has suffered no relapses and is symptom-free, without sequelae.
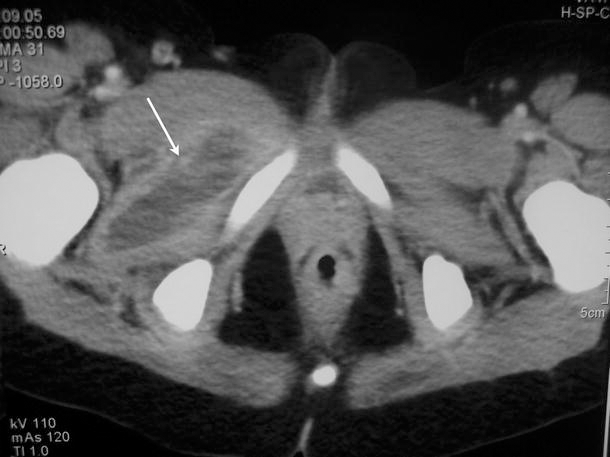
Axial CT scan with contrast confirms the absence of bone involvement, depicting the left obturator internus muscle collection (arrow)
Case 2
A girl aged 6 years and 2 months was referred by her pediatrician with a limp and spikes of fever of up to 39.5 °C for 5 days previously. For 2 days, she had been vomiting twice or three times a day, but no diarrhea was present. Physical examination revealed saburral tongue, pasty mucosae and dry lips, and caseum in the left tonsil. The patient exhibited a flexion and adduction attitude of the left hip, severe pain upon hip mobilization, and functional inability, which precluded weight-bearing. Hip rotation was possible, but only up to 50 %. Inflammation and fullness of the proximal third of the adductor region was observed, with mild pain upon palpation of the adductor magnus, and severe pain upon deep palpation of the pectineal region.
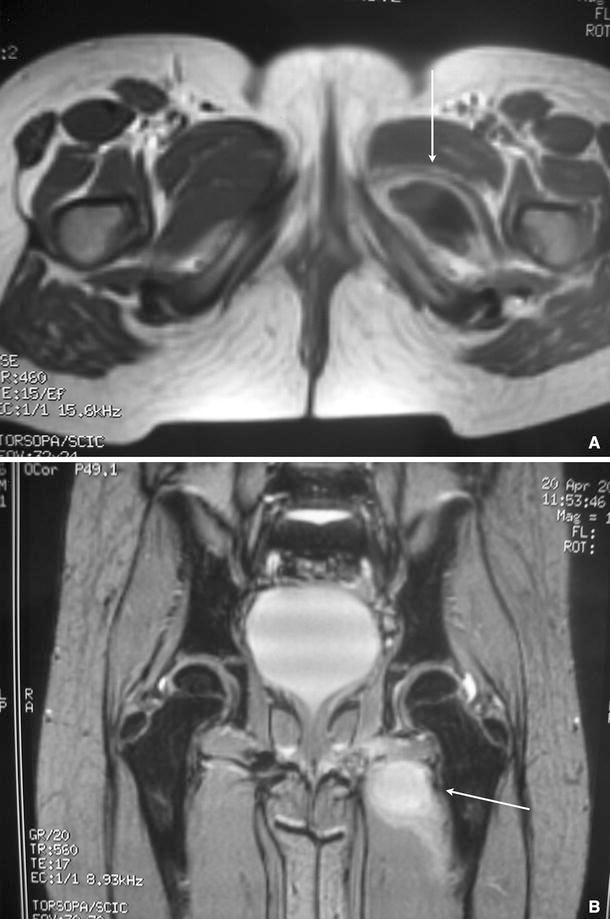
Tc-99 and Ga-67 bone scintigraphy revealed increased uptake in the region of the groin, extending to the pubic region and the superomedial area of the proximal region of the left thigh. MRI revealed an intramuscular abscess in the obturator muscles (Fig. 2). Intravenous treatment with cloxacillin (300 mg/6 h) and cefotaxime (1 g/6 h) was instated. Ten days after admission, the patient's inflammation and fullness remitted clearly. At 12 days, her flexion attitude of the hip had disappeared. At 16 days, she was discharged on oral cloxacillin treatment. Seven years later, the patient is symptom-free, without sequelae.
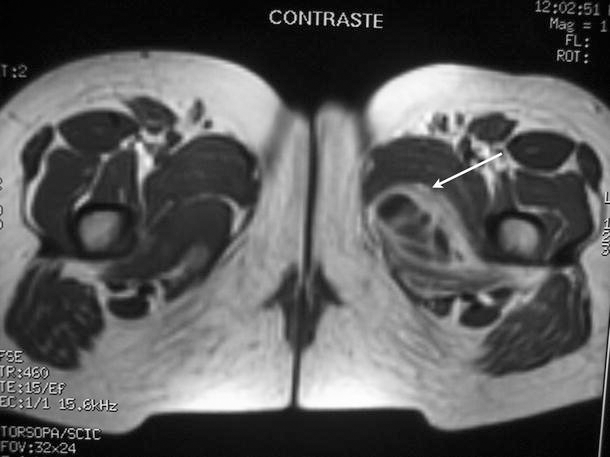
Axial fat-suppressed (STIR) T2-weighted MR images after intravenous contrast administration that shows high signal abnormality involving the right obturator internus muscle (arrow)
Case 3
A boy aged 10 years and 11 months who came to the A&E department with left inguinal pain and spikes of fever of up to 39.5 °C that had persisted for the previous 36 h. He was also suffering from a progressive limp caused by pain.
Physical examination showed prostration due to fever. The patient had mild pain upon mobilization of the hip in maximum rotation. Weight-bearing caused pain and limping. Hip rotation was possible, but only up to 80 %. There was slight inflammation of the ischiatic insertion of the left ischiotibial muscles, with intense pain upon retroischiatic palpation. The MRI showed an intramuscular abscess in the obturator internus and adductor magnus (Fig. 3a, b). The patient was treated with intravenous cloxacillin for 7 days, followed by 3 weeks of oral cloxacillin. Fever disappeared 4 days after admission, and pain remitted gradually over a period of 6 days. Six years later, the patient is symptom-free, without sequelae.
Case 4
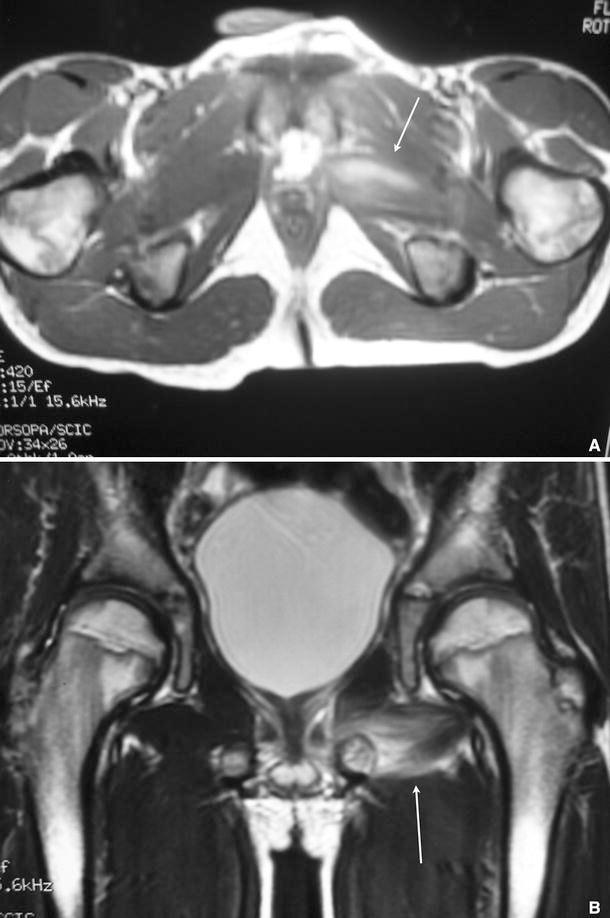
A boy aged 7 years and 8 months who came to the A&E department with left-thigh pain, a limp, and a fever of up to 38.9 °C for the previous 24 h. He was suffering from upper-airway infection. Upon admission, the patient had pain in the left iliac fossa. Mobility of both hips was normal. Thigh palpation and kneading were negative. Thirty-six hours after admission, the patient reported diffuse pain in the adductor insertions. There was slight swelling of the left pelvic floor (next to the ischium), with intense, selective pain at that level. The MRI revealed an intramuscular abscess in the obturator internus muscle (Fig. 4a, b). The patient was treated with intravenous cloxacillin for 10 days, followed by 3 weeks of oral cloxacillin. Fever remitted 3 days after admission, and local tenderness disappeared after 72 h. The patient's limp resolved completely after 9 days. The CRP value returned to a normal level in 8 days. Five years and nine months later, the patient remained symptom-free, and exhibited no sequelae.
Case 5
A boy aged 11 years and 10 months who came to the A&E department with right-thigh pain, severe limp that enabled upright position, and a fever of up to 38.7 °C for the previous 24 h. There was no history of infection. There was slight swelling of the right pelvic floor (next to the ischium), with intense, selective pain at that level. MRI revealed an intramuscular abscess in the obturator internus muscle and adductor magnus reaction (Fig. 5). Tc-99 and Ga-67 bone scintigraphy revealed increase uptake in the region of the ischium and soft tissue in the proximal region of the right thigh. The patient was treated with intravenous cefotaxime and cloxacillin for 10 days, followed by 3 weeks of oral cloxacillin. Fever and local tenderness remitted 2 days after admission. The patient's limp resolved completely after 8 days. The CRP value returned to a normal value in 7 days. Three years later, the patient remained symptom-free, and exhibited no sequelae.

Coronal T1-weighted TSE MR imaging after intravenous contrast administration showing abscess in the left obturator internus muscle and left adductor muscles edema (arrow)
Results
The five cases were patients between 6 and 11 years of age (no infants or adolescents) (Tables 1 and 2). The mean body temperature upon admission was 39.12 °C (38.7–39.5 °C). Fever ≥39 °C was presented after the second day. The five patients were referred to us with a misdiagnosis of intra-abdominal abscess in one patient, gastrointestinal symptoms in one, and septic arthritis of the hip in three cases.
The symptoms were: limp in all five cases, pain in the proximal part of the leg in all five cases (thigh pain in two cases, hip pain in two, and groin pain in one), and abdominal pain in one patient (associated with hip pain). At clinical examination, flexed position of the leg was only present in two cases and slight limitation of the hip rotations in two cases. Therefore, hip impairment at examination is scarce, unlike with psoas pyomyositis, osteomyelitis, and/or septic arthritis of the hip.
The evolution time (from the onset of the symptoms to the onset of antibiotic treatment) ranged from 1 to 5 days.
Leukocyte counts were only elevated in case 2, corresponding to the longer diagnostic delay (5 days). For delayed diagnosis >1.5 days, the CRP ranged from 4.4 to 10.7 mg/L and erythrocyte sedimentation rate (ESR) ranged from 9 to 12 mm/h. For delayed diagnosis between 3 and 5 days, the CRP ranged from 16.8 to 19.9 mg/L and the ESR ranged from 74 to 111 mm/h. There is a significant decline in the clinical status (fever >39 °C, hip reaction) and laboratory results after 24 h.
CT scan and MRI were diagnostic. After finishing the process, CT scan in case 1 and MRI in the other four cases were performed at 3 months of follow-up, checking the resolution of the abscess.
In our cases, fever and limp resolution depends on the time to commencement of antibiotic treatment. Both symptoms disappeared earlier when the diagnostic delay was ≤1.5 days. We studied the possible relationship between the disappearance of the fever and limp with the delay in diagnosis by Pearson's correlation index. For diagnostic delay (>1.5 days) and days with fever, we found a positive correlation of 0.971 (p = 0.006): the longer the delay in diagnosis, the longer it takes the fever to resolve. For diagnostic delay and days with limp, we found also a positive correlation of 0.864 (p = 0.059): longer diagnostic delay means more days limping.
No complication from the treatment was found in any of the cases. There have been no recurrences or sequelae.
Discussion
In the literature, we only found 30 cases of obturator-muscle pyomyositis [4, 7, 10–20], most of them single case reports. The population ranged from children to elderly patients [4], with a male:female ratio of 3:2. Twenty-two cases were described in children [10, 11, 13, 15–19]. Pyomyositis, in general, is more frequent in young adults, but obturator-muscle pyomyositis is predominant in children. Only five cases of pyomyositis of the obturator muscles have been reported in the UK.
Infection of the obturator muscles is exceptionally rare but could be more common than usually believed, as we diagnosed five cases in a relatively small reference population (600,000 inhabitants), four of them between 2004 and 2006. Given the fact that the disease is difficult to diagnose, especially in its initial stages, and considering that in our five cases the condition resolved after rest and antibiotic therapy, it may be speculated that other cases are aborted in their early stages by empirical treatment with antibiotics administered for other suspected infections (septic arthritis, osteomyelitis, cellulitis).
The etiology of pyomyositis has not been clearly determined, but it is believed that it may be a complication of transient bacteremia, which would explain the fact that 30–60 % of cases are multifocal [21]. Its rarity stems from the high level of resistance of striated muscle to episodes of bacteremia [22]. The most frequent causal agent is Staphylococcus aureus (90 % of cases in the tropics and 70 % in non-tropical countries), followed by Streptococcus pyogenes. In cases described in the obturator muscles, most infections were caused by S. aureus. This was true in four out of the five cases we report. Since the disease focuses on the long muscles of the pelvic waist and lower limbs, it is commonly mistaken for other febrile conditions that occur frequently in the region. The average described duration of symptoms is 4.4 days (1–21 days) [12] and diagnostic delay is, therefore, uncommon (3 and 5 days in our cases 1 and 2, respectively).
Physical examination is usually not clear. Patients normally exhibit a triad consisting of fever, pain in the hip, thigh, or abdomen, and limping, which cause functional impotence that precludes weight-bearing on the involved limb (similar to those of septic arthritis of the hip and osteomyelitis). Symptoms are confusing in the first 2–3 days. External manifestations will greatly depend on whether the muscle involved is intra- or extrapelvic. Extrapelvic pyomyositis usually involves the eventual development of external phlogotic signs such as inflammation, warmth, and local tenderness, which reduce the average time to diagnosis [23]. This does not normally occur in intrapelvic cases. The intrapelvic location of the obturator muscles has a blurring effect on symptoms, which largely depend on which neighboring structures are involved, thus, requiring a high index of diagnostic suspicion. The surrounding tissues are frequently indurated and woody to palpation (cases 1 and 3 exhibited inflammatory signs in the adductor muscles). Thigh pain (cases 4 and 5) is a rare symptom that has been described in cases of infection of the obturator internus [11, 16], but also of the psoas and the adductor muscles [6].
Well-localized pain upon palpation around the right ischial tuberosity develops after several days. In our experience, this is one of the most suspicious signs of obturator infection. Induration, fullness, or warmth has not been noted in this region in any cases, including those reported by Birkbeck and Watson [7]. External rotation of the hip is usually more painful than internal rotation, with pain being present in extreme flexion of the hip [15]. Increased discomfort, with resistance to abduction/external rotation (Pace's sign), is common [7].
An antalgic attitude may be present in hip flexion, but hip rotation is totally or partially preserved (mainly in the first 1–2 days). This depends on whether the hip joint is adjacent to the pelvic muscles involved (psoas, adductors, obturators) and reactive hip effusion is present (as in case 1). Limping, functional impairment, some degree of pain upon hip mobilization, and fever are normally present in all cases. Abdominal pain or infection may also occur (cases 1 and 4 at the time of admission), as well as femoral nerve involvement (especially when the psoas muscle is affected). Pain in the lumbar area, the flanks, the right iliac fossa, and the groin can be present. Neurological compromise [24] and the simultaneous occurrence of pyomyositis and septic arthritis of the hip are exceptional [25].
Laboratory tests may reveal high ESR and CRP counts, but alterations of these parameters always depend on the length of diagnostic delay. In our series, these values had suffered clear alterations in cases 1, 2, and 4, but were only slightly altered in case 3. These parameters are no different to any other abscesses in other localizations. We agree with Ovadia et al. [13] that CRP is the most sensitive and clinically helpful parameter in monitoring the course of the disease and its response to treatment. Leukocytosis is not always present at the onset of the disease (cases 1, 3, 4, and 5), but always develops 12–24 h later. It is important to remember that blood cultures are frequently negative [26–29] and S. aureus must, therefore, be regarded empirically as the causal germ. Note that, in 4 of our 5 reported cases, S. aureus was present in the blood cultures.
Plain radiography has the value of ruling out other conditions (osteomyelitis, bone sarcomas, etc.). Ultrasound is the cheapest, most easily available and innocuous tool for ensuring high diagnostic efficiency [30–32], although it has been criticized for missing small lesions [29] and not picking up incipient phlegmonous lesions. It is not normally of use in locating abscesses in the obturator muscles. Ultrasound has a high level of sensitivity but less specificity than CT scan or MRI. Ultrasound and CT scan can be used as ancillary tools in the image-guided percutaneous drainage of purulent material [33]. MRI is the imaging method of choice in the pelvis, since it does not emit ionizing radiation, allows visualization on several planes, and reveals diffuse inflammation in early stages of the disease [22, 34], and it also enables the evaluation of other processes, such as hip joint effusion suggestive of septic arthritis [35, 36]. MRI is preferable because it allows the evaluation of multiple processes, such as joint effusion suggestive of septic arthritis. MRI shows hyperintensity on T2-weighted images and diffuse borders. MRI with contrast is useful to define the extent of abscess involvement, showing a hyperemic ring around the periphery and increased dye uptake around an attenuated necrotic central portion. Edema and inflammatory adductor reaction can be present, being a misleading sign. In all cases of obturator-muscle pyomyositis reported in the literature, diagnosis was confirmed, as in our cases, using CT scan and/or MRI. The MRI scan was misleading in only one of the reported cases [12]. In recent years, pyomyositis is being diagnosed more frequently, probably due to an increase in the number of immunodepressed patients (though that is not the case in this sample) and especially as a result of a greater availability of diagnostic tests, such as CT scan, bone scintigraphy, and, above all, MRI [37]. This can also explain the cluster of our four cases, diagnosed over a short period of time (2004–2006).
Differential diagnosis should rule out abdominal processes (septic conditions, Crohn's disease, obturator hernia), sacroiliitis, osteomyelitis, etc., and especially septic arthritis of the hip, given the devastating consequences that may be associated with a delayed diagnosis of the latter. Nearly 60 % of reported cases of obturator-muscle pyomyositis are initially diagnosed as septic arthritis of the hip [12]. Reactive hip effusion is often present, and requires puncture and aspiration under general anesthesia. When septic arthritis or osteomyelitis have been ruled out using Tc-99 and Ga-67 bone scintigraphy, or Indium-111-labeled leukocyte scans, other uncommon conditions must also be ruled out, because pyomyositis can mimic a malignant tumor in the presence of skeletal pain, tenderness and swelling with or without fever [7, 8], thrombophlebitis, or muscle rupture [7]. Viani et al. [11] reported that 3 out of 7 patients with obturator-internus muscle abscess also had ischial osteomyelitis.
Pyomyositis is not easy to trace in the different groups of muscles around the pelvis. Obturator-, adductor-, or psoas-muscle involvement is confusing, in that its clinical signs and symptoms are similar: spikes of fever, pain in the groin or the hip, and a flexion attitude of the hip [2, 30], usually without differences in laboratory results. A confusing array of clues is present in obturator-muscle pyomyositis, and correct diagnosis can be difficult unless pyomyositis has been included in the differential diagnosis. Given the proximity between the obturator muscles and the sciatic nerve, irritation of the sciatic nerve can be one of the causes leading to such symptoms [7], while proximity to the hip capsule may cause symptoms consistent with a septic hip. Meanwhile, obturator pyomyositis is not easy to diagnose due to the lack of external signs, except for cases with simultaneous adductor reaction (Figs. 3b, 4b, and 5). One of our patients was referred to us misdiagnosed for suspected intra-abdominal abscess and/or septic arthritis, three for suspected septic arthritis (or ischial osteomyelitis), and one because of fever and thigh pain with gastrointestinal infection, revealing the diversity of potential clinical manifestations. In short, septic arthritis of the hip usually presents hip flexion with severe limitation of rotation. Psoas involvement produces an irreducible and/or painful flexion attitude, with increasing pain when attempting to extend the hip but slight limitation of hip rotations. Extrapelvic psoas involvement produces anterior groin lump [2]. Conditions affecting the adductors and external obturator exhibit external inflammation, a slighter and partially reducible flexion attitude, pain upon palpation in the adductor zone, pain upon rectal examination, and even inflammation of the genitals. Obturator pyomyositis shows neither flexion nor limitation of hip rotation. Therefore, obturator pyomyositis can be difficult to diagnose clinically due to the lack of specific signs, although all of our patients had tenderness in the perineum zone.
Therapy must commence with bed rest and intravenous antibiotics (cloxacillin, erythromycin, gentamicin, or third-generation cephalosporin) [38, 39]. We usually administer a combined intravenous therapy, generally cloxacillin (12.5–25 mg/kg/6 h) and cefotaxime (100–150 mg/kg/6–8 h) until blood culture gives the antibiogram. Antibiotic therapy is discontinued when physical signs and symptoms disappear and the blood test and CRP count return to normal values. In the event that antibiotic treatment is not totally effective, ultrasound or CT scan-guided percutaneous drainage [31] should be considered. If this proves inadequate, open drainage should be performed [13, 24]. Antibiotic therapy alone is usually enough, as it was in our five reported cases. The success of conservative treatment in our patients was probably due to the short period of time from symptom onset to the start of antibiotic treatment (1–5 days), preventing the pyomyositis from becoming a rim abscess. Fever and limp disappeared earlier when the diagnostic delay was ≤1.5 days. This seems to apply more frequently in children [40] than in adults [23]. Fourteen out of 30 previously reported cases of obturator-muscle pyomyositis were treated by percutaneous aspiration or surgical open drainage, but antibiotics alone succeeded in 16 cases (14 of them were children). In pyomyositis with abscess formation, percutaneous drainage is more likely to be needed, but is not always necessary [2]. In phlegmon stages of the disease, antibiotics are usually enough. Note that, although rim-enhancing abscesses in other locations are sometimes persistent or resistant to antibiotics alone, this is not the case in obturator locations.
With appropriate treatment, the condition normally resolves without sequelae [1], even at long-term revision [2], as in our cases. If not treated appropriately, however, it can relapse [38] or progress to acute compartmental syndrome and osteonecrosis [13], solid-organ impairment, and even septic shock and death [38].
This description of five new cases of obturator-muscle pyomyositis aims to emphasize the diagnostic difficulties associated with the condition, due to its deep location, multiple initially confusing manifestations, and the fact that its symptoms are similar to those of other more common infections (abdomen) and osteoarticular processes (septic arthritis of the hip, osteomyelitis, and spine). The possibility of this location must be considered in order to establish a diagnosis of obturator pyomyositis. Prompt diagnosis could lead to a good prognosis, complete resolution of the pyomyositis, and absence of complications.