
Abstract
Purpose:
Clavicle injuries are among the most common pediatric injuries. This study aimed to identify the 50 most cited articles on pediatric and adolescent clavicle injuries, characterize their publication trends, and assess the correlation between citation metrics and study quality.
Methods:
A bibliometric analysis was performed using Web of Science and Scopus databases, identifying the 50 most cited articles on pediatric and adolescent clavicle injuries. Data extracted included citation counts, citation density, study design, level of evidence, and publication characteristics. Methodological quality was assessed using the modified Coleman Methodology Score (mCMS) and Methodological Index for Non-Randomized Studies (MINORS), where applicable. Correlations between citation metrics and quality scores were evaluated using Spearman correlation.
Results:
Among the 50 most cited articles published between 1984 and 2019, the majority (70%) were published in the last decade and in Journal of Pediatric Orthopaedics (38%). Most studies originated from the United States (74%). The mean citation count was 31.9 ± 19.7, with a citation density of 2.6 ± 1.4 citations/year. Level 4 evidence predominated (73%), with no level 1 studies identified. The average mCMS and MINORS scores were 40.1 and 13.1, respectively. No significant correlation was found between citation rank and methodological quality scores, although citation rank was significantly correlated with citation density (rs = −0.66, p < 0.001).
Conclusions:
The most cited studies on pediatric clavicle injuries are predominantly low-level evidence and retrospective in nature. Citation frequency was not associated with methodological quality, suggesting that article influence is often driven by historical context, novelty, or foundational relevance rather than study rigor.
Keywords
Introduction
Clavicle injuries are common in pediatrics, and clavicle fractures in particular account for approximately 10%–15% of all pediatric fractures. 1 Many fractures are treated nonoperatively due to the robust remodeling potential of pediatric patients. In adult populations, treatment paradigms have shifted over time, with a recent resurgence in operative fixation for displaced, comminuted, or shortened fractures. 1 Similarly, management trends in the pediatric population, particularly in adolescents, have shown an increased inclination toward operative intervention, although most can be successfully managed nonoperatively.2–6 Although adolescents retain greater remodeling potential than adults, their higher activity levels may make them more susceptible to functional limitations following suboptimal healing. 7 However, decisions regarding surgical treatment must be carefully weighed against the risks of anesthesia, hardware implantation in skeletally immature patients, and other operative complications such as infection. Therefore, there should be a joint decision-making model between physicians, parents or guardians, and patients, when appropriate, on whether to proceed with surgery.
Treatment decisions in orthopedics are shaped by a combination of historical practices and evolving literature. A critical appraisal of influential studies over time can illuminate changes in clinical practice and help identify gaps in knowledge, guiding future research toward optimizing patient outcomes. Furthermore, it is essential that current research addresses clinically meaningful questions to support evidence-based decision-making. Bibliometric analyses have been widely used across orthopedics to identify key contributions in various subspecialties.8,9
Such an analysis focused on pediatric clavicle injuries is particularly valuable, as it can reveal whether research trends align with current clinical guidelines and recommendations. While multiple articles may exist to contribute an eventual consensus, there is not necessarily a correlation between the number of available citations and high quality of evidence. 9
The purpose of this study was to identify and characterize the 50 most cited articles on pediatric and adolescent clavicle injuries, assess trends in publication and study characteristics, and evaluate the relationship between citation metrics and quality of evidence. We hypothesized that highly cited articles would demonstrate limited correlation with methodological quality and would reflect more historical or foundational significance rather than representing contemporary advancements or higher-level evidence. A significant challenge in delineating treatment paradigms for pediatric clavicle fractures is the inherent difficulty in conducting level I studies. Ethical concerns, logistical hurdles, and variability complicate randomized trials in pediatric populations. This study aims to highlight not only existing literature but also to map future avenues for rigorous research.
Materials and methods
The methods were adapted from previous recommendations and strategies for bibliometric analysis.8–10 An online search was performed utilizing two databases: (1) Web of Science (all databases) and (2) Scopus. These databases were selected for their ability to search independent terms and present the number of citations per article. The following search terms and Boolean operators were utilized to identify articles with titles relating to pediatric and adolescent clavicle fractures: ((adolescent) OR (pediatric) OR (skeletally immature)) AND ((clavicle) OR (clavicular) OR (clavicle fracture)). The search was performed using each database on 4 April 2024. All articles extracted from the search were included in initial screening. Articles were sorted from the most to the least number of citations on each database individually. Four authors (SMG, EO, SA, NKP) evaluated articles from each database for inclusion with the topic relating to pediatric and adolescent clavicle fractures. Articles were evaluated in sequence from most cited to least cited to generate the top 75 from each database individually. The number of citations from each database was averaged for each study, and the articles were resorted using the new means from most to least citations to generate the top 50 list.
In addition to the number of citations on each database, the following data were collected from each article: digital object identifier or PubMed identifier, title, author list, year of publication, journal name, country of origin, study type (i.e. case series, cohort study, case control, randomized controlled trial, biomechanical/cadaveric, imaging/diagnostic, technique/review), study category (diagnostic, prognostic, therapeutic), and level of evidence. Each article was assigned a decade of publication based on the publication year. The level of evidence was agreed upon by the authors; the level of evidence was not scored for biomechanical/cadaveric studies or technique/review studies. The methodological quality of studies was evaluated using the modified Coleman Methodology Score (mCMS) (scoring range, 0–100) and Methodological Index for Non-Randomized Studies (MINORS) (scoring range, 0–16 for noncomparative studies and 0–24 for comparative studies).11–13 mCMS was only applied to studies on clinical treatment, and MINORS was not applied to randomized trials. Biomechanical/cadaveric studies, imaging/diagnostic studies, and technique/reviews were not assessed for methodological quality. The number of citations per year (citation density) was calculated from the mean obtained divided by the number of years since publication.
Data were aggregated and presented utilizing descriptive statistics. The Spearman correlation coefficient (rs) was used to evaluate correlations between citation values (mean number citations, citation density) and level of evidence and methodological quality, in addition to between year of publication and level of evidence. The strength of correlation was denoted by the absolute value of rs: weak, <0.4; moderate, 0.4–0.7; and strong, >0.7. 14 Significance was set at p < 0.05 for two-tailed testing. Statistical analysis was performed on STATA v16.1 (Stata-Corp, College Station, TX).
Results
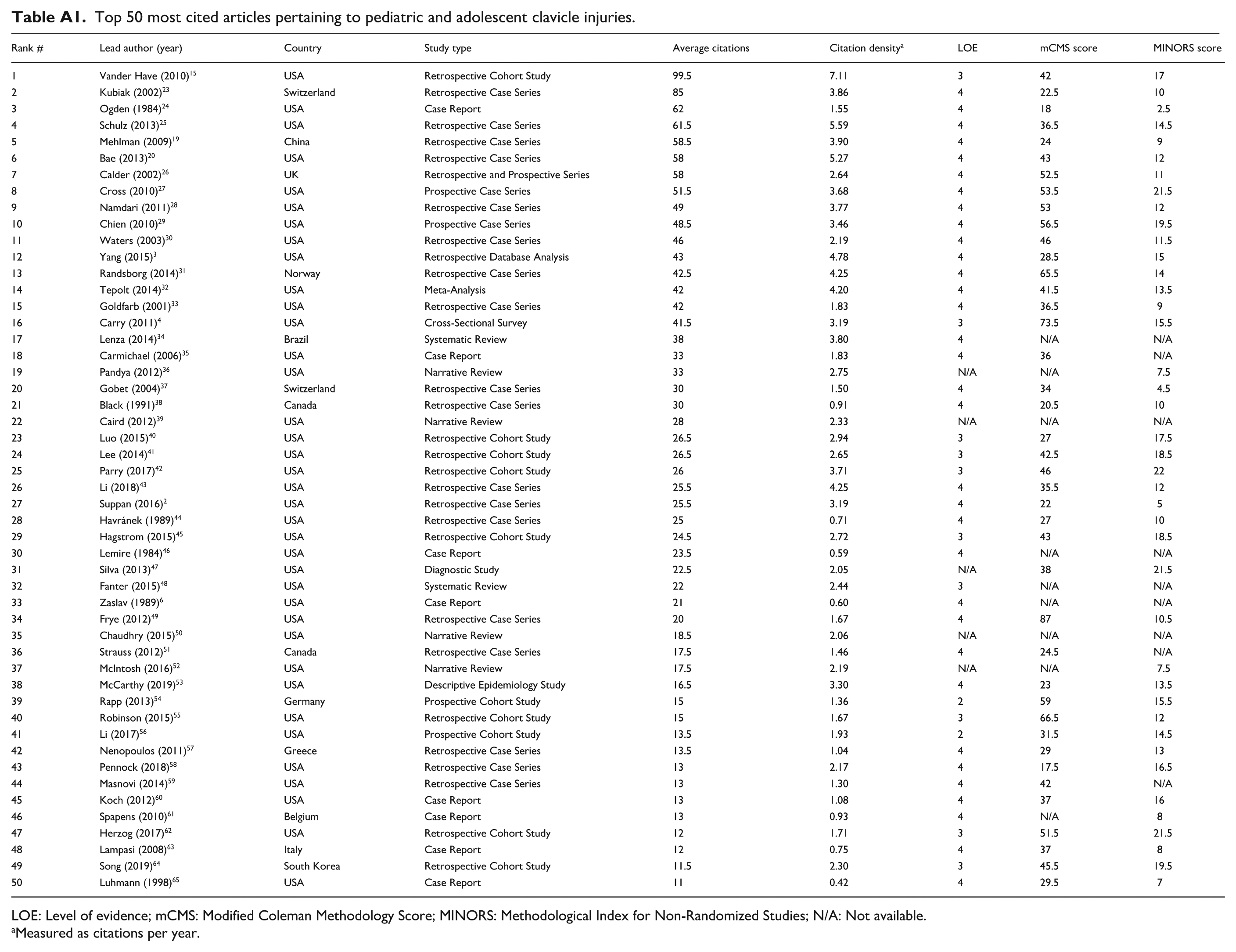
The top 50 most cited articles relating to pediatric and adolescent clavicle fractures were published between 1984 and 2019 (Appendix 1, Table A1). Most of the articles were published between 2010 and 2019 (70%) (Figure 1). Articles were published in 23 different journals with Journal of Pediatric Orthopaedics being the most common at 38% (Figure 2). The most common country of origin was the United States, representing 74% of the publications (Figure 3).
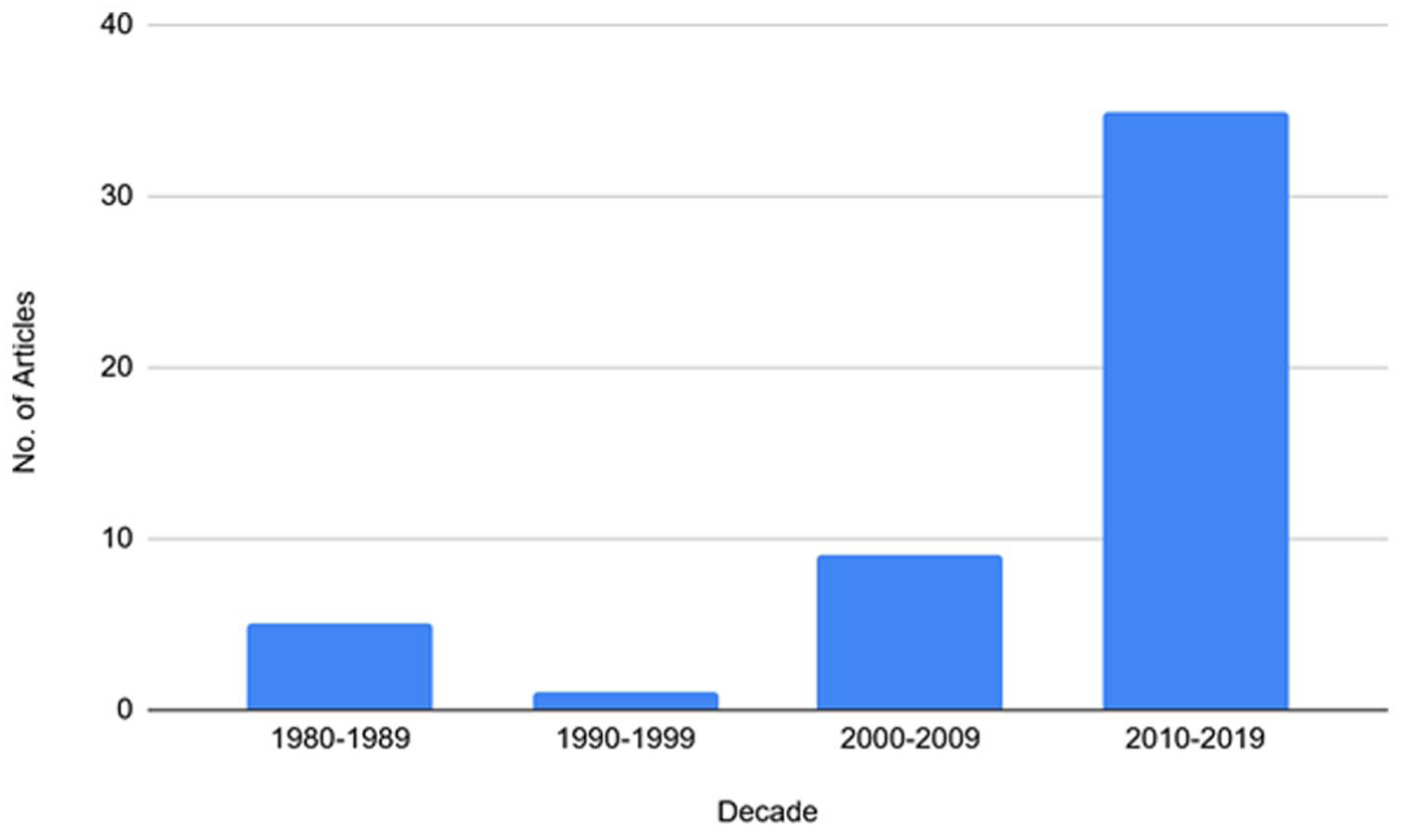
Number of 50 most cited articles relating to pediatric and adolescent clavicle injuries by decade of publication.
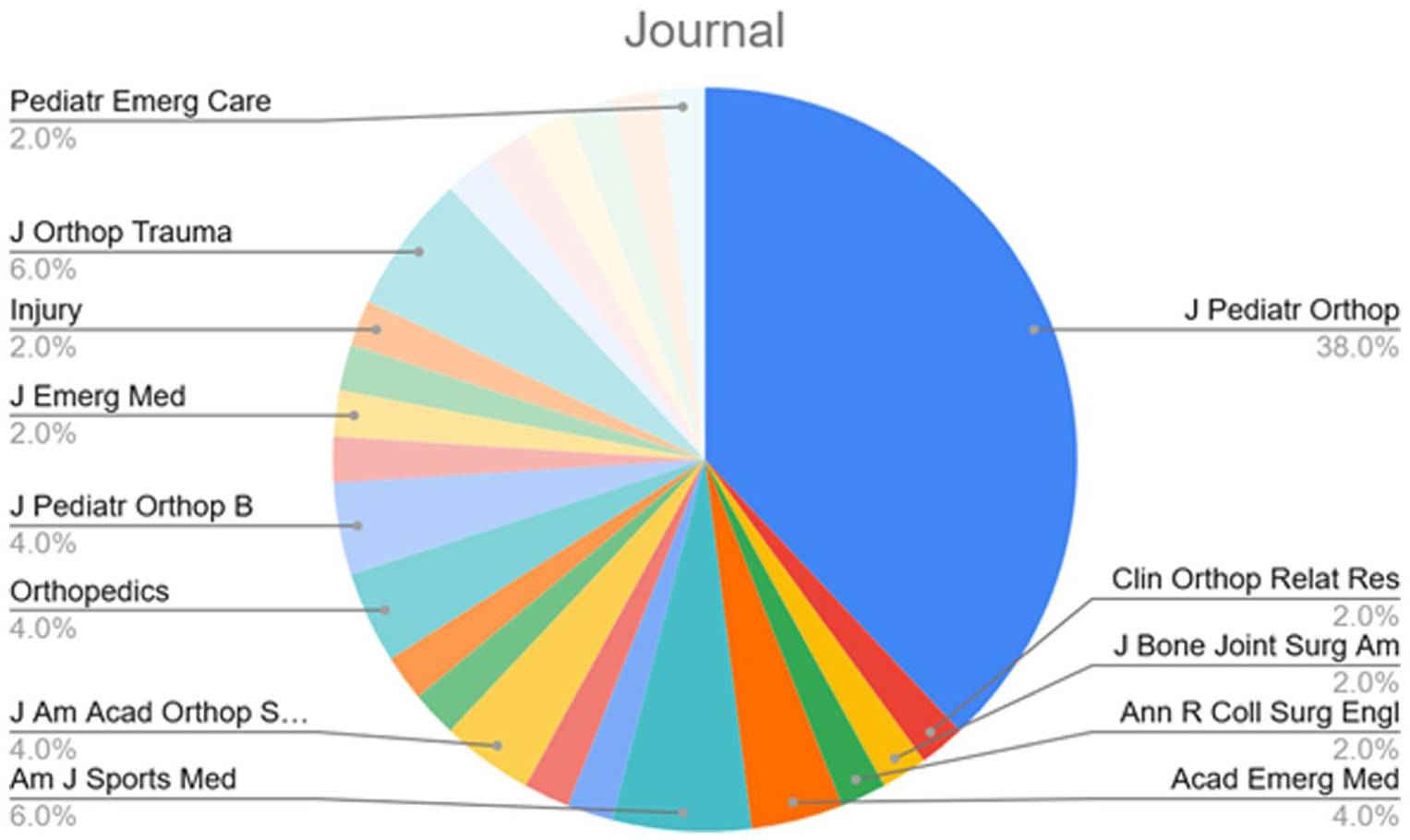
Percentage of 50 most cited articles relating to pediatric and adolescent clavicle injuries by the journal of publication.
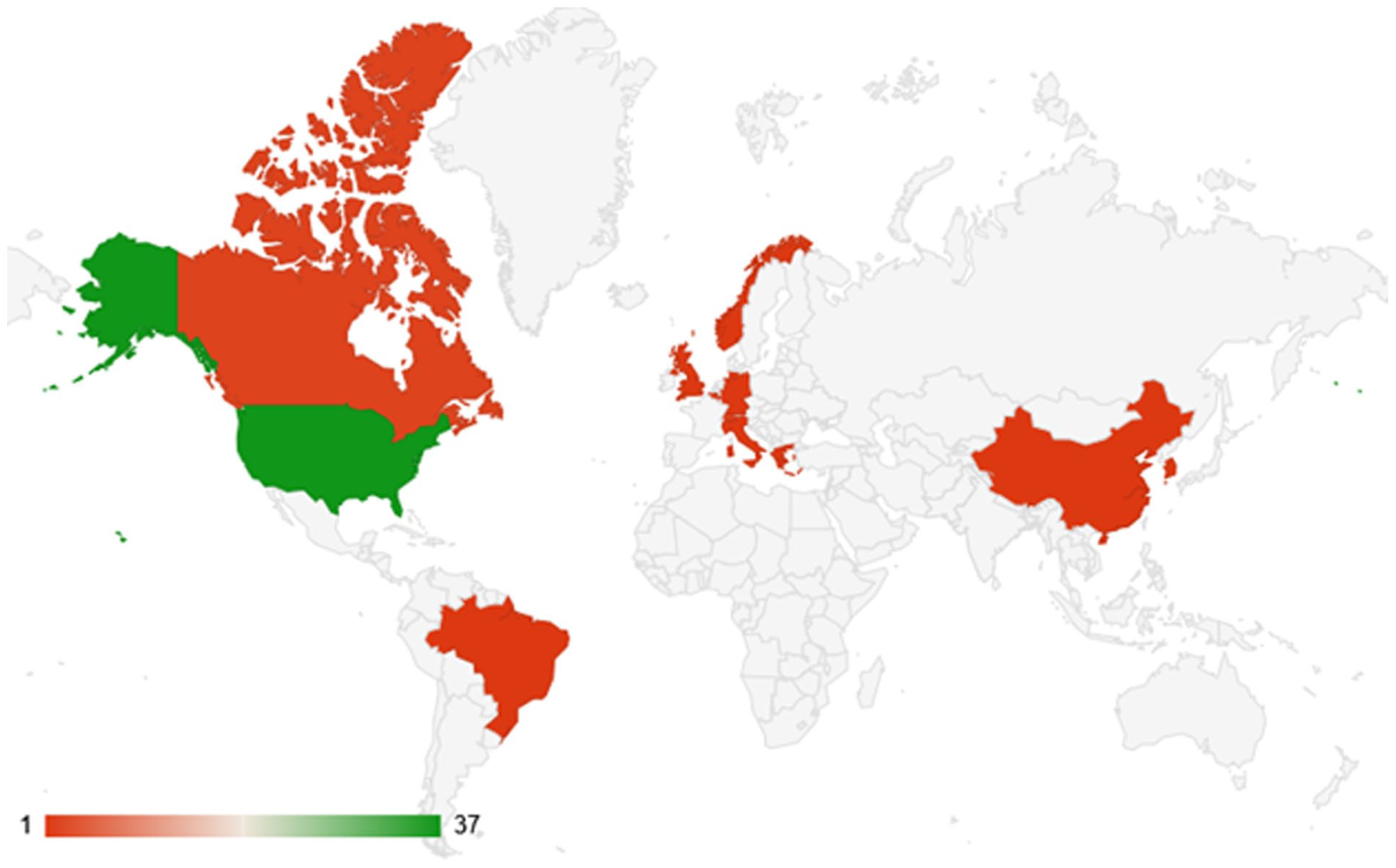
Map of countries of origin for the most cited articles pertaining to pediatric and adolescent clavicle injuries by journal of publication.
The mean ± SD number of citations was 31.9 ± 19.7 (range, 11–99.5) (Appendix 1, Table A1). The mean ± SD citation density was 2.6 ± 1.4 citations/year (range, 0.4–7.11 citations/year), with the same paper being the most cited for both mean number of citations and citation density. 15
Most articles evaluated for level of evidence were level 4 (n = 33/45, 73%; Figure 4). There were no level 1 studies. Out of these studies, the top three classifications were retrospective case series (36%), retrospective cohort studies (16%), and case reports (16%; Figure 5). A total of 41 studies were assessed for methodological quality in total (Appendix 1, Table A1).
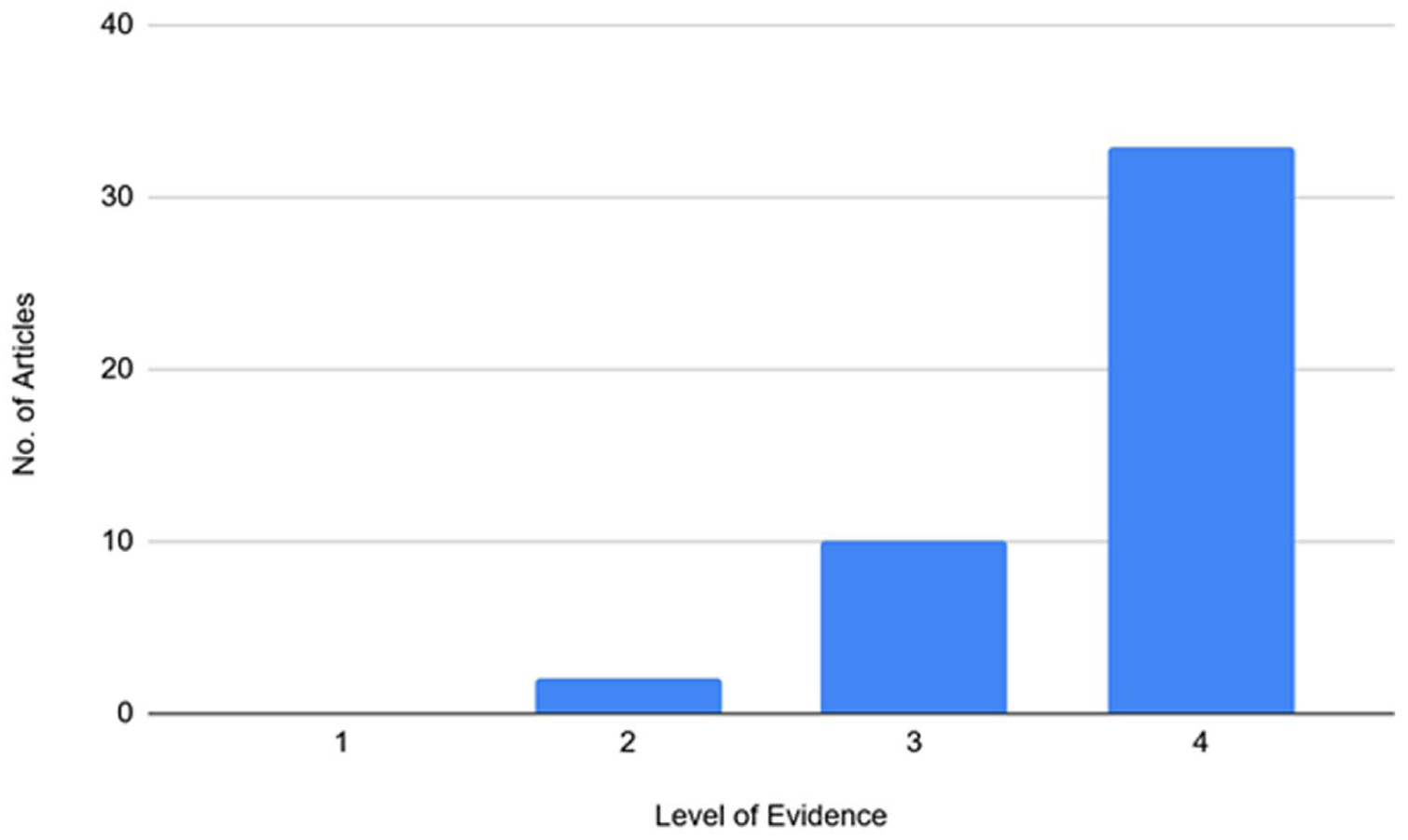
Number of 50 most cited articles relating to pediatric and adolescent clavicle injuries by assigned level of evidence.
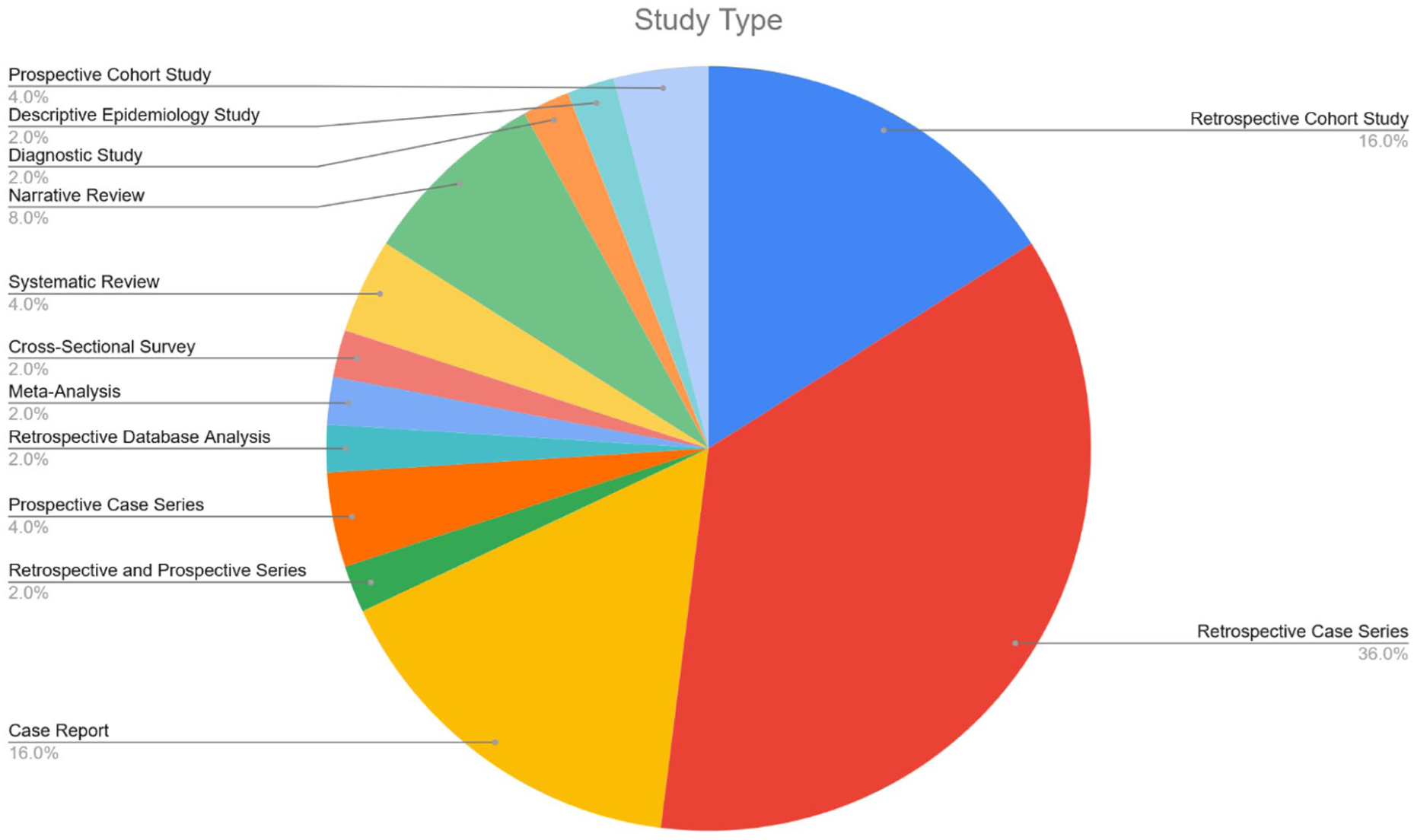
Percentage of 50 most cited articles relating to pediatric and adolescent clavicle injuries by study design type.
The mean ± SD mCMS was 40.1 ± 15.6 (range, 17.5–87). The mean ± SD MINORS score was 13.1 ± 5.0 (range, 2.5–22). There was a statistically significant correlation between citation rank and citation density (rs = −0.66; p = 0.00) (Figure 6 and Table 1). There was not a significant correlation between either mCMS or MINORS score and citation rank (Table 1).
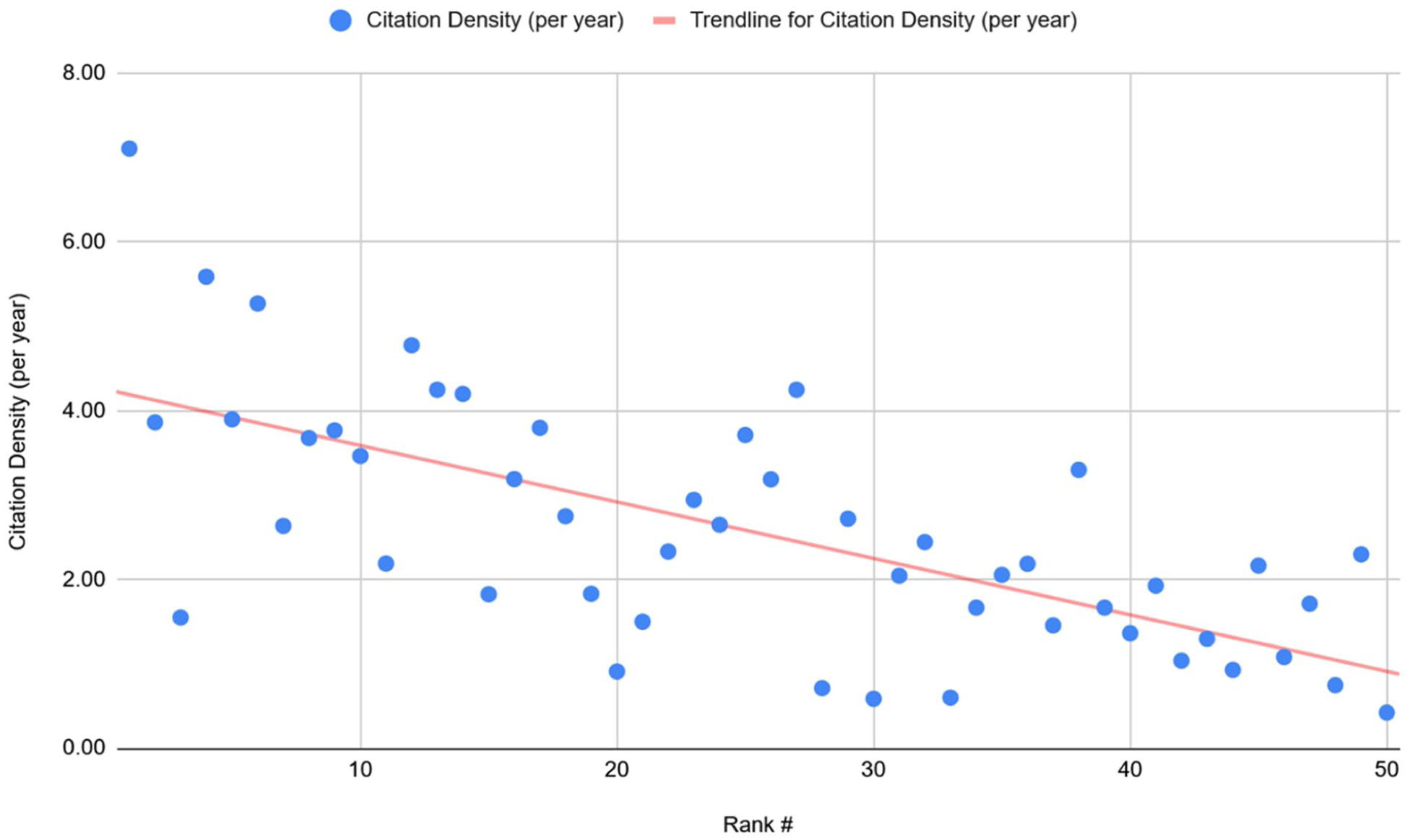
Correlation between citation density (per year) and rank of publication by mean number of citations.
Spearman correlations between citation density and level of evidence and methodological quality assessments.
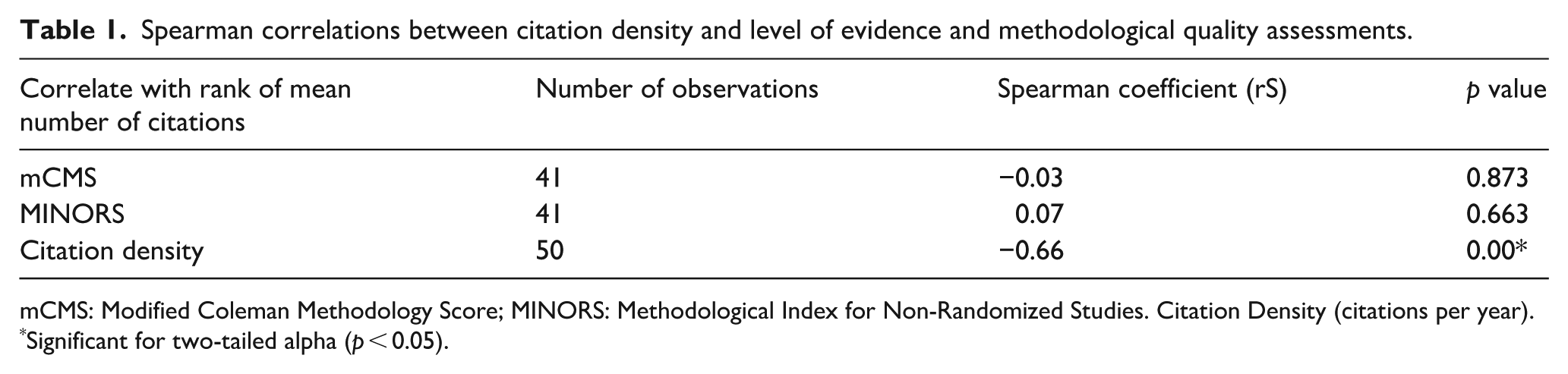
mCMS: Modified Coleman Methodology Score; MINORS: Methodological Index for Non-Randomized Studies. Citation Density (citations per year).
Significant for two-tailed alpha (p < 0.05).
Discussion
The present study identified the top 50 articles relating to pediatric clavicle injuries. The majority of the most cited articles on this topic are of a lower level of evidence, with no included studies that were level 1 evidence. The topics within the top 50 articles on pediatric clavicle injuries ranged from the diagnosis of fractures in the emergency department, comparison of nonoperative and operative treatments, physeal injuries, and sternoclavicular dislocations.
Of the studies for which methodological quality was assessed, there were no significant correlations between methodology scores and number of citations. Therefore, the methodological quality of a study may not appropriately capture a study’s literature influence, at least that measured by citations. The effect of a study may derive from its contribution to foundational understanding or development of new concepts from which further higher-level research may arise. Longer term follow-up studies are more likely to be retrospective in nature and therefore have a lower level of evidence that may not capture the benefit of elucidating long-term outcomes. In the present study of the top 50 articles, 72% were retrospective studies, demonstrating this phenomenon.
In another bibliometric analysis of all pediatric fractures, clavicle fractures were found to be among the top keywords related to publications of pediatric fracture data from 2020 to 2022. 16 Interestingly, the top cited article in our study was previously found to be the 16th and 49th most cited article on clavicle fractures in a bibliometric analysis of all clavicle fracture studies (including adults) in two prior studies, respectively.15,17,18 Two other studies in the top six in our analysis were also included one of these studies.17,19,20 This highlights the discrepancy in literature volume between adult and pediatric clavicle fracture studies.
A substantial portion of the articles identified in our analysis (n = 35) focused on operative management of pediatric clavicle fractures or comparisons between operative and nonoperative approaches. Recent studies from the Prospective Multicenter FACTS Study Group have demonstrated limited indications for surgical fixation of pediatric clavicle fractures.21,22 These studies have shown the significant remodeling potential of pediatric clavicle fractures and no significant differences in outcomes with nonoperatively treated fractures compared with those treated surgically. As such, future research is likely to concentrate on further refining the indications for operative management. Additionally, there is an increasing need for studies that address post-injury rehabilitation protocols and provide evidence-based guidelines for safe return to sport, which is particularly relevant for the active adolescent population.
There were also a high number of articles focusing on rare or unique cases. Firstly, case reports represented 16% of the top-cited articles. However, case reports tend to be focused on rare pathology and while they are educational and can be useful in specific cases, they may have less significance than higher level studies in changing practice. Furthermore, many studies emphasized physeal injuries and sternoclavicular injuries, likely a much higher proportion than the relative proportion of these injuries seen in clinical practice. This trend demonstrates the effect of novelty on citations.
This study has inherent limitations related to its methodology. The selection of the top 50 most cited articles was arbitrary, and many impactful studies may fall outside this cutoff. Citation-based analyses inherently favor older publications, as they have had more time to accumulate citations. Accordingly, recent studies, such as the most recent from 2019, may not yet reflect their potential influence. Some highly cited older studies may be cited more for historical context than for current clinical relevance. Conversely, foundational studies may be cited less over time as their insights become widely accepted and no longer referenced direct, a phenomenon that can obscure their ongoing importance. Additionally, citation counts are dynamic and may change significantly over time. Evaluating citation density within a shorter window, such as the first 5 years post-publication, might better capture a study’s early and immediate impact.
Conclusion
The most cited studies in pediatric clavicle injury literature are largely low-level evidence and retrospective in nature. There is limited correlation between citation impact and methodological quality. Future research may benefit from prioritizing higher level prospective studies to improve evidence-based practices.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521251411146 – Supplemental material for Influential articles on pediatric clavicle injuries: A bibliometric analysis
Supplemental material, sj-pdf-1-cho-10.1177_18632521251411146 for Influential articles on pediatric clavicle injuries: A bibliometric analysis by Steven M Garcia, Erin Orozco, Abhay Kopardekar, Sachin Allahabadi and Nirav Pandya in Journal of Children's Orthopaedics
Footnotes
Appendix 1
Top 50 most cited articles pertaining to pediatric and adolescent clavicle injuries.
| Rank # | Lead author (year) | Country | Study type | Average citations | Citation density a | LOE | mCMS score | MINORS score |
|---|---|---|---|---|---|---|---|---|
| 1 | Vander Have (2010) 15 | USA | Retrospective Cohort Study | 99.5 | 7.11 | 3 | 42 | 17 |
| 2 | Kubiak (2002) 23 | Switzerland | Retrospective Case Series | 85 | 3.86 | 4 | 22.5 | 10 |
| 3 | Ogden (1984) 24 | USA | Case Report | 62 | 1.55 | 4 | 18 | 2.5 |
| 4 | Schulz (2013) 25 | USA | Retrospective Case Series | 61.5 | 5.59 | 4 | 36.5 | 14.5 |
| 5 | Mehlman (2009) 19 | China | Retrospective Case Series | 58.5 | 3.90 | 4 | 24 | 9 |
| 6 | Bae (2013) 20 | USA | Retrospective Case Series | 58 | 5.27 | 4 | 43 | 12 |
| 7 | Calder (2002) 26 | UK | Retrospective and Prospective Series | 58 | 2.64 | 4 | 52.5 | 11 |
| 8 | Cross (2010) 27 | USA | Prospective Case Series | 51.5 | 3.68 | 4 | 53.5 | 21.5 |
| 9 | Namdari (2011) 28 | USA | Retrospective Case Series | 49 | 3.77 | 4 | 53 | 12 |
| 10 | Chien (2010) 29 | USA | Prospective Case Series | 48.5 | 3.46 | 4 | 56.5 | 19.5 |
| 11 | Waters (2003) 30 | USA | Retrospective Case Series | 46 | 2.19 | 4 | 46 | 11.5 |
| 12 | Yang (2015) 3 | USA | Retrospective Database Analysis | 43 | 4.78 | 4 | 28.5 | 15 |
| 13 | Randsborg (2014) 31 | Norway | Retrospective Case Series | 42.5 | 4.25 | 4 | 65.5 | 14 |
| 14 | Tepolt (2014) 32 | USA | Meta-Analysis | 42 | 4.20 | 4 | 41.5 | 13.5 |
| 15 | Goldfarb (2001) 33 | USA | Retrospective Case Series | 42 | 1.83 | 4 | 36.5 | 9 |
| 16 | Carry (2011) 4 | USA | Cross-Sectional Survey | 41.5 | 3.19 | 3 | 73.5 | 15.5 |
| 17 | Lenza (2014) 34 | Brazil | Systematic Review | 38 | 3.80 | 4 | N/A | N/A |
| 18 | Carmichael (2006) 35 | USA | Case Report | 33 | 1.83 | 4 | 36 | N/A |
| 19 | Pandya (2012) 36 | USA | Narrative Review | 33 | 2.75 | N/A | N/A | 7.5 |
| 20 | Gobet (2004) 37 | Switzerland | Retrospective Case Series | 30 | 1.50 | 4 | 34 | 4.5 |
| 21 | Black (1991) 38 | Canada | Retrospective Case Series | 30 | 0.91 | 4 | 20.5 | 10 |
| 22 | Caird (2012) 39 | USA | Narrative Review | 28 | 2.33 | N/A | N/A | N/A |
| 23 | Luo (2015) 40 | USA | Retrospective Cohort Study | 26.5 | 2.94 | 3 | 27 | 17.5 |
| 24 | Lee (2014) 41 | USA | Retrospective Cohort Study | 26.5 | 2.65 | 3 | 42.5 | 18.5 |
| 25 | Parry (2017) 42 | USA | Retrospective Cohort Study | 26 | 3.71 | 3 | 46 | 22 |
| 26 | Li (2018) 43 | USA | Retrospective Case Series | 25.5 | 4.25 | 4 | 35.5 | 12 |
| 27 | Suppan (2016) 2 | USA | Retrospective Case Series | 25.5 | 3.19 | 4 | 22 | 5 |
| 28 | Havránek (1989) 44 | USA | Retrospective Case Series | 25 | 0.71 | 4 | 27 | 10 |
| 29 | Hagstrom (2015) 45 | USA | Retrospective Cohort Study | 24.5 | 2.72 | 3 | 43 | 18.5 |
| 30 | Lemire (1984) 46 | USA | Case Report | 23.5 | 0.59 | 4 | N/A | N/A |
| 31 | Silva (2013) 47 | USA | Diagnostic Study | 22.5 | 2.05 | N/A | 38 | 21.5 |
| 32 | Fanter (2015) 48 | USA | Systematic Review | 22 | 2.44 | 3 | N/A | N/A |
| 33 | Zaslav (1989) 6 | USA | Case Report | 21 | 0.60 | 4 | N/A | N/A |
| 34 | Frye (2012) 49 | USA | Retrospective Case Series | 20 | 1.67 | 4 | 87 | 10.5 |
| 35 | Chaudhry (2015) 50 | USA | Narrative Review | 18.5 | 2.06 | N/A | N/A | N/A |
| 36 | Strauss (2012) 51 | Canada | Retrospective Case Series | 17.5 | 1.46 | 4 | 24.5 | N/A |
| 37 | McIntosh (2016) 52 | USA | Narrative Review | 17.5 | 2.19 | N/A | N/A | 7.5 |
| 38 | McCarthy (2019) 53 | USA | Descriptive Epidemiology Study | 16.5 | 3.30 | 4 | 23 | 13.5 |
| 39 | Rapp (2013) 54 | Germany | Prospective Cohort Study | 15 | 1.36 | 2 | 59 | 15.5 |
| 40 | Robinson (2015) 55 | USA | Retrospective Cohort Study | 15 | 1.67 | 3 | 66.5 | 12 |
| 41 | Li (2017) 56 | USA | Prospective Cohort Study | 13.5 | 1.93 | 2 | 31.5 | 14.5 |
| 42 | Nenopoulos (2011) 57 | Greece | Retrospective Case Series | 13.5 | 1.04 | 4 | 29 | 13 |
| 43 | Pennock (2018) 58 | USA | Retrospective Case Series | 13 | 2.17 | 4 | 17.5 | 16.5 |
| 44 | Masnovi (2014) 59 | USA | Retrospective Case Series | 13 | 1.30 | 4 | 42 | N/A |
| 45 | Koch (2012) 60 | USA | Case Report | 13 | 1.08 | 4 | 37 | 16 |
| 46 | Spapens (2010) 61 | Belgium | Case Report | 13 | 0.93 | 4 | N/A | 8 |
| 47 | Herzog (2017) 62 | USA | Retrospective Cohort Study | 12 | 1.71 | 3 | 51.5 | 21.5 |
| 48 | Lampasi (2008) 63 | Italy | Case Report | 12 | 0.75 | 4 | 37 | 8 |
| 49 | Song (2019) 64 | South Korea | Retrospective Cohort Study | 11.5 | 2.30 | 3 | 45.5 | 19.5 |
| 50 | Luhmann (1998) 65 | USA | Case Report | 11 | 0.42 | 4 | 29.5 | 7 |
LOE: Level of evidence; mCMS: Modified Coleman Methodology Score; MINORS: Methodological Index for Non-Randomized Studies; N/A: Not available.
Measured as citations per year.
Author contributions
Steven M Garcia—Conceptualization, data collection, formal analysis, manuscript writing and editing, methodology, visualization
Erin Orozco—Data collection, formal analysis, manuscript writing and editing, visualization.
Abhay Kopardekar—Data collection and manuscript editing
Sachin Allahabadi—Conceptualization, formal analysis, manuscript writing and editing, methodology, visualization
Nirav Pandya—Conceptualization, manuscript writing and editing, methodology, supervision
Note: All authors have read and agreed to the published version of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical considerations
Ethics board approval was not required for this bibliometric analysis study.
Data availability statement
The data that support the findings of this study are available from the corresponding author on request.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.