
Abstract
Purpose
The treatment of displaced midshaft clavicle fractures in children remains controversial. The purpose of our study was to compare the outcome of displaced midshaft clavicle fractures in children who were managed operatively by flexible intramedullary nailing (FIN) with nonoperative treatment.
Methods
A prospective review of 31 children (mean age 10.5 years) with displaced midshaft clavicle fractures treated either by FIN or nonoperatively and with at least a six-month follow-up was undertaken. In all, 24 children underwent FIN and seven underwent nonoperative treatment. The patient outcomes included the Constant-Murley score, Customer Satisfaction Questionnaire (CSQ-8), numeric pain rating scale, time to union and time to return to activity. Surgical complications were recorded.
Results
The two groups were comparable with regards to age, gender and mechanism of injury. At six months of follow-up, the Constant-Murley (97.8 versus 94.7, p < 0.001) and CSQ-8 (29.1 versus 19.1, p < 0.001) scores were higher in the FIN group. Time to union and return to activity were significantly shorter in the FIN group (7.3 and 9.2 weeks versus 10.4 and 16.6 weeks respectively, p < 0.01). The only surgical complication was a FIN exchange for skin irritation due to nail prominence.
Conclusion
FIN is a minimally invasive procedure for children with displaced midshaft clavicle fractures associated with shorter time to union, quicker return to activity and higher Constant-Murley and CSQ-8 scores when compared with nonoperative treatment. However, the difference in Constant-Murley scores was not clinically significant. Furthermore, the advantages of FIN are at the expense of an increased complication rate of 12.5% (upper 95% confidence interval 33.3%).
Level of Evidence
Therapeutic, II
Introduction
The clavicle is the most frequently fractured bone in the shoulder region in children, accounting for 10% to 15% of all fractures1–5 with an incidence of 29 to 64 per 100 000 people.6,7 The midshaft of the clavicle undergoes a change in shape from concave to convex in the coronal plane and from round to flat in cross-section1,2 and as a result of this adjustment, 90% of fractures occur in the midshaft of the clavicle.7–9 McGraw et al 10 found that most of the clavicle growth occurs before the age of nine years in girls and 12 years in boys. Hence, there is limited ability for the clavicle to remodel if malunion occurs in patients aged between 12 to 18 years old.
Children with midshaft clavicle fractures are traditionally treated nonoperatively even in the presence of considerable displacement. Clinical studies have suggested that nonunion of midshaft clavicle fractures is uncommon in children and that malunion does not confer any clinical importance with the potential long-term ability for remodelling of the clavicle.5,11 However, there has been a recent increase in the trend for operative treatment of the paediatric patient with displaced midshaft clavicle fractures for several reasons. One reason is that there has been a paradigm shift in favour of operative treatment in adult displaced midshaft clavicle fractures following the publication of several randomized controlled trials (RCTs) suggesting better outcomes with operative treatment.4,12 Furthermore, the rates of malunion and nonunion following nonoperative treatment are higher and associated with shoulder weakness and residual pain.13–18 Despite this evidence from adult studies, the literature on the treatment of children with displaced midshaft clavicle fractures remains controversial. Studies that compare operative and nonoperative treatment are sparse. Moreover, there are only five retrospective studies that compare operative versus nonoperative treatment of children with displaced midshaft clavicle fractures with conflicting results.1,5,19–21
The possible operative treatments of children with displaced midshaft clavicle fractures include; Kirschner wire (K-wire) fixation, open reduction and internal fixation (ORIF) with plates and screws and flexible intramedullary nailing (FIN). Both K-wire fixation and ORIF have a greater incidence of complications and poor cosmetic outcomes.22–24 Even though little is known about the postoperative results of FIN in children, it is still considered a safe and effective method of treatment for older children22,25 and adults. 26 Kubiak and Slongo 27 reported indications for the use of FIN, which include neurovascular compromise, open fractures, severe shortening of the shoulder girdle and displaced fractures. Other indications for FIN include tenting of the skin over the clavicle1–3 and polytrauma. 22
The purpose of our study was to prospectively assess patient-oriented outcomes following operative treatment with FIN versus nonoperative treatment for children with displaced midshaft clavicle fractures. Our hypothesis was that children with displaced midshaft clavicle fractures who were treated operatively have better functional outcomes when compared with those managed with nonoperative treatment.
Patients and methods
After ethical approval was obtained from our Institutional Review Board, we conducted a prospective cohort study of children with displaced midshaft clavicle fractures who were treated at our institution between 2010 and 2015.
Inclusion and exclusion criteria
The inclusion criteria included paediatric patients aged from 8 to 18 years with displaced midshaft clavicle fracture who underwent operative treatment with FIN or nonoperative treatment. The family of the patient and the patient made the choice of treatment after a thorough discussion of both options. We excluded patients who did not adhere to follow-up visits, those with unavailable radiographs and cases of polytrauma.
Intervention
The nonoperative group was treated with a figure-of-eight brace for six to eight weeks. The operative group was treated with FIN. Children undergoing operative treatment had surgery on the same day of presentation or the next working day. The procedure was performed under fluoroscopic guidance. Patients were operated on in the supine position with a sand bag placed between the spine and medial border of the scapula, which elevated the shoulder and assisted to an extent in reducing the midshaft fracture of the clavicle. After administration of anaesthesia and intravenous prophylactic antibiotics, a small transverse incision was made 1 cm to 2 cm lateral to the sternoclavicular joint on the affected side. The subcutaneous fat and platysma were incised. The pectoral fascia was then divided in line with the skin incision followed by careful elevation of the underlying musculature from the clavicle. An aperture was made using a bone awl through the anterior clavicular cortex on the medial side creating an entry point. A 2-mm titanium flexible intramedullary nail was introduced through the entry point from the medial clavicular segment into the clavicular medullary canal until it reached the fracture site. The intramedullary nail in the proximal segment was utilized as a joystick with manipulation to achieve successful closed reduction. Thereafter, the curved distal end of the intramedullary nail was advanced across the fracture and introduced into the lateral clavicular segment to its final position. A flexible intramedullary nail of this size provided good stability of the fracture and easily negotiated the two curves of the clavicular canal. Subsequently, the medial end of the intramedullary nail was withdrawn approximately 1 cm and cut short, then the nail was bent, rotated and advanced to its final non-prominent position. The subcutaneous tissue and skin were closed and the shoulder was placed in a sling. We advised our patients to restrain from sporting activities on average for nine to ten weeks or until radiographic union of the fracture.
Outcome measures
Patient outcomes measures included functional status, patient satisfaction, self-reported pain, union time and return to activity time. Patients were assessed at two weeks, one month, two months and finally at six months. A physician not involved in the care of the patients assessed functional status. All other outcome measures were self-reported by the children.
Shoulder functional status was assessed using the Constant-Murley score which has been used previously in the paediatric literature as an outcome measure in clavicle fractures. 22 It consists of a 100-point scale with 0 indicating worst function and 100 indicating best function. The score is divided into four domains: 15 points for pain, 20 points for daily living activities, 25 points for strength and 40 points for range of movement. 28
Overall satisfaction was assessed using the Client Satisfaction Questionnaire (CSQ-8) which consists of eight questions, and responses to each question are rated from 1 to 4. 29 The maximum CSQ-8 score is 32, where higher scores reflect better satisfaction.
Self-reported pain was assessed using the numeric pain rating scale for children (0 to 10 points: 0 = no pain; 10 points = extreme pain), which was measured postoperatively for the operative group. 30
Radiographic imaging was performed at one- and two-month follow-up visits, using an anteroposterior and 45° cephalic tilt view to assess healing of the fracture and any associated complications such as displacement or angulation.11,31 Fracture union was defined as healing of at least three cortices in both views. Delayed union was considered when there was no bridging of the fracture at six months from the date of injury. Malunion was defined as disruption of the anatomical alignment of the shoulder girdle compared with the uninjured side. 5 Return to activity time was determined if healing was evident on radiographs and the clavicle was not tender.
Statistical analysis
Statistical data were analyzed using Stata/IC 15.1 statistical package (StataCorp LLC, College Station, Texas). Descriptive statistics were performed by the calculation of frequency, percentages, mean and sd. Sample characteristics were summarized using mean ± sd for numerical data and frequency and percentages for categorical data. For the comparison between discrete variables a chi-square or Fisher's exact test was used. For the comparison of continuous variables, non-parametric Mann-Whitney U test was used. A p-value < 0.05 was considered statistically significant.
Results
We identified 35 children with displaced midshaft clavicle fractures between 2010 and 2015 (Fig. 1), of which we recruited 31 children and four were excluded due to polytrauma and undergoing ORIF. Of the recruited cases, 24 children underwent operative treatment with FIN (Fig. 2), and seven were managed nonoperatively. The mean age of the children was 10.5 years (8 to 16) with 65% being male (n=20) and the left clavicle was fractured in 58% of patients (n=18). Sports injuries and road traffic accidents were the most common cause of fracture in the operative group, whereas, bicycle riding was the inciting event in the nonoperative group. The two groups were similar and details are provided in Table 1. All 31 children sustained a displaced midshaft clavicle fracture and five had angulation in addition to displacement. Displacement was defined as more than 45° axial deviation on radiographs; dislocation of shaft width or more; or shortening of at least 1.5 cm. 22 The mean clavicle displacement was 19.5 mm (16 to 25). Five of the 24 patients that underwent operative treatment with FIN required a mini-open reduction during nail insertion. All 31 children completed six months follow-up. All operative children underwent FIN removal 12 to 16 weeks after initial surgery.
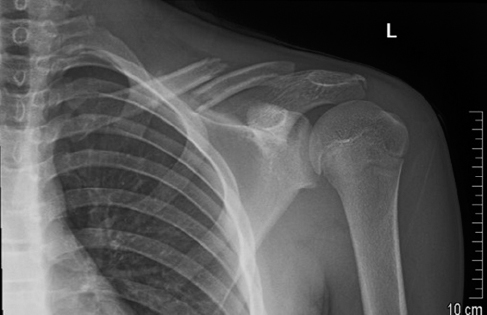
Radiograph of a 13-year-old male with a left displaced midshaft clavicle fracture.
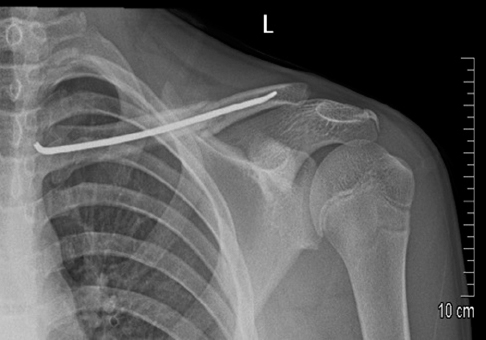
Postoperative radiograph of a left displaced midshaft clavicle fracture treated with fixed intramedullary nailing.
Patient demographics and characteristics
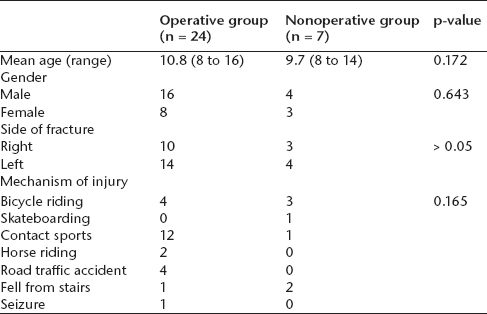
p < 0.05, statistical significance
Mean union time for the operative group was 7.3 weeks (6 to 8) which was significantly shorter than those who underwent nonoperative treatment with a mean union time of 10.4 weeks (9 to 12) (p < 0.001). Additionally, the operative group had an earlier return to activity time that was 9.2 weeks compared with the nonoperative group that had a mean return to activity time of 16.6 weeks (p < 0.001).
The nonoperative group reported a higher pain score with a mean score of 2.0 at two weeks, and a mean score of 0.5 at four weeks on the numeric pain rating scale for children. Whereas in the operative group the self-reported pain score was lower, with a mean score of 1.4 on the day of the surgery, 0.3 on the first day postoperatively and no pain at two weeks.
In the operative group, children achieved full arm mobilization one day following surgery and full activity was regained within seven days. Children who underwent surgery with FIN had better range of movement, shoulder power and function compared with the nonoperative group. The mean Constant-Murley score for the operative group was higher than the nonoperative group (97.8 versus 94.7, p < 0.001) at six months follow-up. Table 2 summarizes the main outcomes for both groups and Table 3 displays the Constant-Murley score comparisons between the groups.
Outcomes comparison between the operative and nonoperative groups
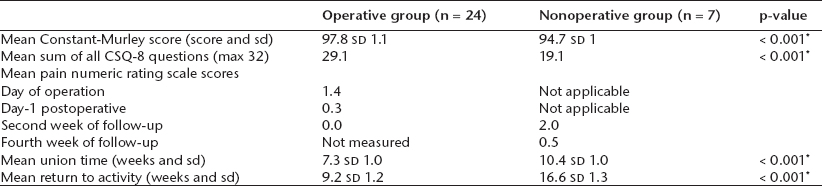
p < 0.05 statistical significance
Constant-Murley scores for both groups

p < 0.05 statistical significance
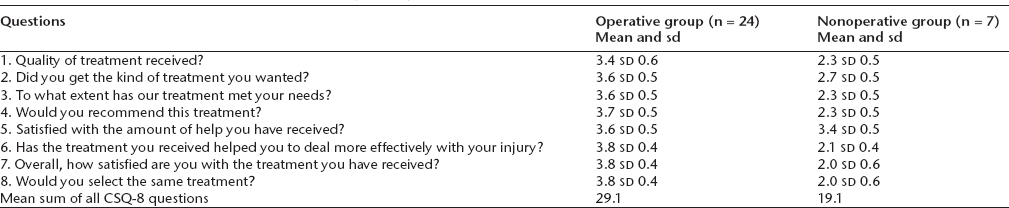
The mean overall satisfaction score for children who underwent operative treatment was significantly higher than the nonoperative group (29.1 versus 19.1, p < 0.001) at six months follow-up. Moreover, patients in the operative group were very satisfied with the surgical scar (CSQ-8; cosmetic question mean score = 3.9). Whereas, the nonoperative group reported sleep disturbance, paraesthesia and more discomfort from wearing the sling/brace. Table 4 summarizes the CSQ-8 scores for both groups.
Customer Satisfaction Questionnaire (CSQ-8) for both groups
Among the operative group, three out of 24 patients (12.5%) had complications. Two operative cases sustained re-fractures following further trauma from falling while horse riding. This can serve as a learning point to delay the return to activity in order to prevent re-fractures. The re-fractures were associated with nail bending and were treated by re-insertion of a new FIN. One child in the operative group underwent revision surgery for skin irritation due to nail prominence. There were no complications such as infection, malunion/nonunion, neurovascular compromise, scar hypertrophy or keloid formation. All the displaced midshaft clavicle fractures in both groups united within the six-month follow-up. None of the children in the nonoperative group required operative treatment for malunion.
Discussion
Clavicle fractures are one of the most common fractures in children, with each patient requiring a specific treatment tailored to the patient needs and extent of injury. Displaced midshaft clavicle fractures account for the majority of clavicle fractures, and nonoperative treatment remains the benchmark. This predilection to nonoperative management is mainly due to earlier studies reporting the rarity of nonunion in adults, lack of symptoms of malunion of clavicle fractures and the potential complications of operative treatment.32–34 However, recent evidence has demonstrated rather unfavourable outcomes in adult displaced midshaft clavicle fractures that were managed nonoperatively. A multicentre RCT conducted by the Canadian Orthopaedic Trauma Society 4 on 132 adult patients (mean age 33.5 years) with displaced midshaft fractures showed significantly improved Constant-Murley shoulder scores and disabilities of arm, shoulder and hand (DASH) scores reflecting better functional outcomes in the operative versus nonoperative group. Furthermore, the operative group had lower rates of malunion and nonunion as opposed to those who underwent nonoperative treatment. Another recent multicentre RCT on 200 patients (age range 16 to 60 years) with displaced midshaft clavicle fractures reported similar findings with lesser rates of nonunion and better functional outcomes in patients who underwent ORIF compared with nonoperative treatment. 12 Hence, there has been a paradigm shift in the treatment of adult displaced midshaft clavicle fractures in favour of operative treatment. A recent meta-analysis of adult midshaft clavicle fractures showed that nonunions were more frequent in displaced fractures that underwent nonoperative treatment rather than operative fixation, with nonunion rates of 15.1% and 2.2% respectively. 18 This alarming rate of nonunion after nonoperative treatment of adult clavicle fractures might have influenced the management of children with displaced midshaft clavicle fractures despite the fact that nonunion of clavicle fractures in children is rare. Such influence is evident in a recent survey of surgeons of the Pediatric Orthopaedic Society of North America, which reported that nearly 50% of surgeons were in favour of operative treatment for displaced midshaft clavicle fractures in older children. 35
Five retrospective cohort studies exist in the literature that compare operative with nonoperative treatment of children with displaced midshaft clavicle fractures.1,5,19–21 The first study was conducted in 2010 by Vander Have et al 5 on 42 patients with a mean age of 15.4 years. They found that the mean time to radiographic fracture union was shorter for those who underwent plate fixation treatment compared with nonoperative treatment. Operative treatment was successful with no major complications, and patients regained full range of movement and fracture union at a mean of 88 days. Furthermore, return to activity time was 12 weeks in the operative group compared with 16 weeks in the nonoperative group. Hagstrom et al 1 reviewed 78 patients and reported no significant difference between both groups in terms of return to activity, fracture healing and DASH scores, although approximately 40% and 60% of patients who underwent nonoperative and operative treatment were lost to follow-up, respectively. These findings were recently supported in a study of 16 patients by Parry et al, 19 who conducted a single time follow-up visit. They found that there was no significant difference between the operative and nonoperative treatment with regards to range of movement, strength and fatigue testing, Constant-Murley and QuickDASH scores. However, they had a small sample size of 16 patients and a follow-up period ranging from ten to 41 months. In another recent study of 20 adolescents with midshaft clavicle fractures, Herzog et al 20 reported no statistically significant difference between the operative and nonoperative treatments when comparing DASH and the American Shoulder and Elbow Surgeons standardized shoulder questionnaires, despite their conclusion that nonoperative treatment was associated with worse functional outcome when comparing the injured shoulder to its uninjured counterpart in each patient. Despite the favourable outcomes of operative treatment from the aforementioned studies, Luo et al 21 found in a retrospective study of 153 paediatric midshaft clavicle fractures that operative treatment was associated with a 21.7% complication rate compared with 0.8% with nonoperative treatment. Hence, the debate continues with those studies favouring nonoperative treatment. Additionally, a case series of 36 patients with midshaft clavicle fractures showed an 86% complication rate with plate fixation. 36 Furthermore, in another case series of 16 children by Bae et al, 32 malunion of the midshaft clavicle following nonoperative treatment posed no clinically significant loss of strength or range of movement compared with the uninjured clavicle.
In a RCT on displaced midshaft clavicle fracture in adults, Smekal et al 26 reported that FIN resulted in higher union rates and better functional outcomes compared with nonoperative treatment. Similarly, Kubiak and Slongo 27 recommended FIN in children with midshaft clavicle fractures. Furthermore, Rapp et al 22 prospectively studied 24 patients aged between ten and 15 years with displaced midshaft clavicle fractures. All 24 patients underwent FIN, and had satisfactory outcomes such as full mobilization from the first day postoperatively; full functional activity after seven days; return to sport activity after 30 days; and very low self-reported pain. However, five complications occurred such as nail breakage, deformation and imminent skin perforation. These complications were preventable by trimming the nail and restricting sport activities for a period of four to eight weeks. Furthermore, Namdari et al 23 reviewed 14 patients (mean age 12.9 years) with displaced midshaft clavicle fractures who all underwent ORIF. All patients had excellent outcomes reflected by a mean QuickDASH score of 7 (0 to 100; no disability-maximum disability) and a mean of 11 questions answered ‘yes’ to the simple shoulder test. However, there was no control nonoperative group.
Our study results have shown that clavicle fractures benefit from operative treatment with FIN as opposed to nonoperative treatment with regards to early fracture healing and return to activity. The Constant-Murley score was statistically significant in favour of FIN, however, this was not clinically significant as the minimal clinical important difference is at least 10 points. 37 An advantage of operative treatment with FIN is the minimal approach and insertion of the intramedullary nail, which is confirmed in our study as evident by a mean CSQ-8 cosmetic score of 3.9. An additional benefit of FIN is that self-reported postoperative pain was lower than nonoperative treatment in our study.
Although two of our patients in the operative group required revision surgery due to nail bending after falling while horse riding, no malunion or nonunion occurred in the operative group, which was similarly reported in the study by Rapp et al. 22 However, a complication developed in one patient in the operative group who required revision surgery due to skin irritation from nail prominence. This could have been avoided by cutting the nail to a maximum length of 5 mm protruding from the bone to avoid skin penetration as previously reported by Rapp et al. 22 Other disadvantages to FIN are the need for another procedure to remove the intramedullary nail and postoperative nail migration that may occur due to shortening of the clavicle. In our study, there were no cases of intramedullary nail migration and all FINs were removed with another procedure. Given we had a complication rate of 12.5% in the operative group (three out of 24 patients), it is important to acknowledge that this study had a small sample size (n = 31). Hence, the calculated upper limit of the 95% confidence interval for the complication rate following FIN was 33.3%. 38
We recognize that this study is not without limitations. It had a small total sample size (n = 31) with uneven distribution in both groups which is underpowered after performing a power calculation. The patients were not randomized to operative and nonoperative treatments, and this could introduce selection bias that most likely depended on patient age and fracture configuration. Furthermore, measurements of some of the outcomes were vulnerable to observer bias because of the non-blinded nature of the study design.
FIN is a minimally invasive procedure for children with displaced midshaft clavicle fractures that was accompanied with shorter time to union, quicker return to activity and higher Constant-Murley and CSQ-8 scores when compared with nonoperative treatment. However, the difference in Constant-Murley scores was not clinically significant. Furthermore, the advantages offered by FIN are at the expense of an increased complication rate of 12.5% (95% upper confidence interval 33.3%). The standard treatment of paediatric displaced midshaft fractures remains a matter of ongoing debate unless absolute indications of operative are present. Future RCTs are required to support the effectiveness of operative treatment compared with nonoperative treatment for children with displaced midshaft clavicle fractures.
Footnotes
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
Ethical approval: All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.