
Abstract
Abstract
Purpose
The purpose of this study was to compare functional outcomes of adolescents with and without ankle syndesmotic injuries and identify predictors of functional outcome after operative ankle fractures.
Methods
A retrospective review was conducted on operative adolescent ankle fractures treated between 2009 and 2019 with a minimum of one-year follow-up (mean 4.35 years). Patients who underwent syndesmotic fixation (SF) (n = 48) were compared with operative ankle fractures without syndesmotic injury (n = 63). Functional outcomes were assessed using standardized questionnaires, specifically the Foot and Ankle Ability Measure (FAAM) and Single Assessment Numerical Evaluation.
Results
There were no differences in patient-reported outcomes, rates of return to sport or complications between groups with and without SF. The SF group had a longer tourniquet time (p = 0.04), duration of non-weight-bearing (p = 0.01), more Weber C fibula fractures (p < 0.001), fewer medial malleolus fractures (p = 0.03) and more frequently underwent implant removal (p < 0.0001). Male sex, lower body mass index (BMI) and longer duration of follow-up were significant predictors of a higher FAAM sports score using multivariable linear regression. SF was not a predictor of functional outcome.
Conclusion
This study demonstrated that patients that undergo surgical fixation of syndesmotic injuries have equivalent functional outcomes compared to operative ankle fractures without intraoperative evidence of syndesmotic injury. We also identified that male sex, lower BMI and longer duration of follow-up are predictors of a good functional outcome.
Level of Evidence
III
Introduction
Syndesmosis injuries are common, occurring in 1% to 18% of ankle sprains1–5 and 10% to 23% of ankle fractures in the adult population.6,7 The syndesmosis is repaired in 37% to 45% of operative Weber B fractures and 58% to 72% of operative Weber C fractures in adults.8–10 The incidence and natural history of this injury in paediatric and adolescent patients remains unclear, and few studies have examined functional outcomes.11,12 Kramer et al 13 reported a 1% prevalence of syndesmotic injury in all paediatric patients undergoing evaluation for ankle trauma, and Lurie et al 14 found that 36.7% of Weber B and 57.7% of Weber C unstable adolescent ankle fractures required syndesmotic fixation (SF). Accurate diagnosis without radiographic examination under anaesthesia can be difficult due to the low sensitivity and specificity of clinical examination and static radiographs, especially in skeletally immature patients.4,14–19
Injury to the syndesmosis in adults has been shown to be associated with worse functional outcomes, pain, stiffness and swelling.1,12,16,20 It is also associated with longer recovery times and time to return to sport.1,20–22 Appropriate syndesmotic reduction has been shown to have a significant impact on functional outcome in skeletally mature patients.4,6,23–25 While prior studies have compared the outcomes of ankle fractures with and without syndesmotic injury, the results were mixed, inclusion and exclusion criteria varied significantly between studies and very few studies included a significant number of adolescent patients.19,26–29
The purpose of this study was to identify adolescent patients that underwent operative fixation of either a Weber B or C ankle fracture and compare functional outcomes between those with and without a syndesmotic injury requiring SF.
Materials and methods
Study design
This was an institutional review board-approved retrospective study of patients with operative ankle fractures treated at a single institution between January 1, 2009 and December 31, 2019. Inclusion criteria were adolescent patients (defined as ages 10 to 19 years) 30 who underwent open reduction internal fixation of a Weber B or C fibula fracture, with minimum one-year follow-up. Excluded fracture types consisted of pilon fractures, Weber A fibula fractures and transitional fractures (Tillaux and triplane fractures). Skeletal maturity was defined as a closed physis on radiographs, whereas skeletal immaturity was defined as an open or partially open physis. Chart and radiographic reviews were conducted to determine demographic data (age, sex, weight, body mass index (BMI)), Weber classification, presence of a medial or posterior malleolus fracture, the status of the physis and sport or activity at time of injury. Tourniquet time, immobilization time and duration of non-weight-bearing were also recorded. At time of most recent follow-up, complete demographic, radiographic and operative data was available for all patients with the exception of BMI which was unavailable for five patients.
Outcome assessment
Functional outcome data was obtained by telephone at a minimum of one-year postoperatively using the Foot and Ankle Ability Measure (FAAM) questionnaire and Single Assessment Numerical Evaluation (SANE) questionnaire 31 , Williams. The FAAM questionnaire is composed of an Activities of Daily Living (ADL) subscale and a Sports subscale. The ADL section assesses difficulty with walking, climbing stairs and working, while the Sports section assesses difficulty with running, jumping, lateral movements and other sports-related activities. The SANE score consists of a single numerical score from 0 to 100 for the patient's subjective determination of their ankle function. The SANE score was administered for function during ADL and sports activities (denoted as SANE ADL and SANE Sports). Assessment of patients’ return to sport was assessed with a yes/no response to the question “have you been able to return to your normal physical activity or sport?” All patients had FAAM ADL and FAAM Sports scores available. SANE ADL and SANE Sports scores were available for 83.3% of patients (97.9% SF group, 72.7% no SF group). Return to sport and patient satisfaction scores were available for 50% of patients (43.8% SF group, 54.5% no SF group). Complication rates were also compared between the two groups.
Operative technique
All procedures were performed under general anaesthesia and with use of intraoperative fluoroscopic imaging. Because more than ten paediatric orthopaedic surgeons contributed cases to this series, variation existed with respect to the exact surgical approach and technique. In general, however, our institution has a fairly standardized approach which is summarized below. The fibula fracture was typically exposed with a lateral approach unless fixation of the posterior malleolus was necessary in which case a posterolateral approach was used. Most fibula fractures were treated with one or two lag screws and a neutralization plate. Certain long oblique fractures with no comminution were treated with two to three lag screws and no neutralization plate. SF was deemed necessary when force to the distal fibula caused either > 2 mm of lateral translation of the fibula with widening of the ankle mortise on the anteroposterior view or > 2 mm of posterior translation of the fibula relative to the tibia on a lateral view. The choice of syndesmotic screw or suture-button device, and the decision to remove syndesmotic implants, was made by the treating surgeon. Patients with medial malleolus fractures were treated with one or two 4-mm screws as necessary. Posterior malleolus fractures involving > 20% of the posterior articular surface were generally reduced and fixed with 4-mm screws. A layered closure was performed, re-approximating the periosteum over the implants.
Postoperatively, patients were placed in a short-leg non-weight-bearing cast or splint for two to six weeks and then transitioned to a controlled ankle motion (CAM) boot. For injuries not involving the syndesmosis, progressive weight-bearing was typically allowed at six weeks once there was evidence of radiographic healing on standardized anteroposterior and lateral radiographs. For patients with syndesmotic injuries, progressive weight-bearing was initiated at six to 12 weeks postoperatively. The exact timing of progressive weight-bearing was at the discretion of the treating surgeon. Physical therapy directed towards ankle strengthening, range of movement and proprioception was typically initiated at six weeks.
Statistical analysis
Basic descriptive statistics are reported. Continuous data was tested for normality with the Shapiro-Wilk test. All continuous data except for age and weight was not normally distributed due to the relatively small sample size and, therefore, the non-parametric Mann-Whitney test was used to compare means. Proportions of binary data was compared using Pearson's chi-squared test. A multivariable linear regression model was developed using backward stepwise regression, iteratively eliminating potential predictor variables with the highest p-value until the model contained only statistically significant predictors. Five patients who did not have BMI data available were excluded from the model to allow for analysis of this potentially clinically relevant variable. A post hoc power analysis was performed to determine whether we had adequate sample size to detect a ten-point difference in FAAM Sports score (approximately equal to the minimal clinically important difference (MCID) of the instrument as calculated by Martin et al). 32 Using the calculated sd of 14 points for the mean FAAM Sports score in our cohort, 42 patients per group would be required to have a power of 90% and an alpha of 5%. Thus, we concluded our study was adequately powered to compare FAAM Sports score between the two groups. Statistical analysis was conducted using the SciPy (version 1.2.3, open source, www.scipy.org) and StatsModels (version 0.6.1, open source, www.statsmodels.org) Python packages. Statistical significance was defined as p < 0.05.
Results
There were 111 surgically treated unstable ankle fractures included in the study. There were 48 patients in the SF group and 63 in the no SF group. Within the SF group, 21 patients had a suture-button construct, 26 patients had a syndesmotic screw and one patient had both a suture-button and syndesmotic screw. Representative case examples are shown in Figure 1 which demonstrates pre- and postoperative imaging for four patients with supination-external rotation (SER) and pronation-external rotation ankle fractures that did and did not require SF. Both a syndesmotic screw and suture-button construct are shown for SF. Table 1 shows the demographic and radiographic data of the two cohorts. Patient ages at the time of surgery ranged from 11 to 18 years. There were 66 male and 45 female patients. There were no statistically significant differences between the SF and no SF groups in terms of age (p = 0.28) or sex (p = 0.71). BMI was significantly higher in the SF (mean 29.1; SD 6.1; range 19.9 to 44) versus the no SF group (mean 26.2; SD 5.6; range 16.4 to 44.6) (p = 0.008).
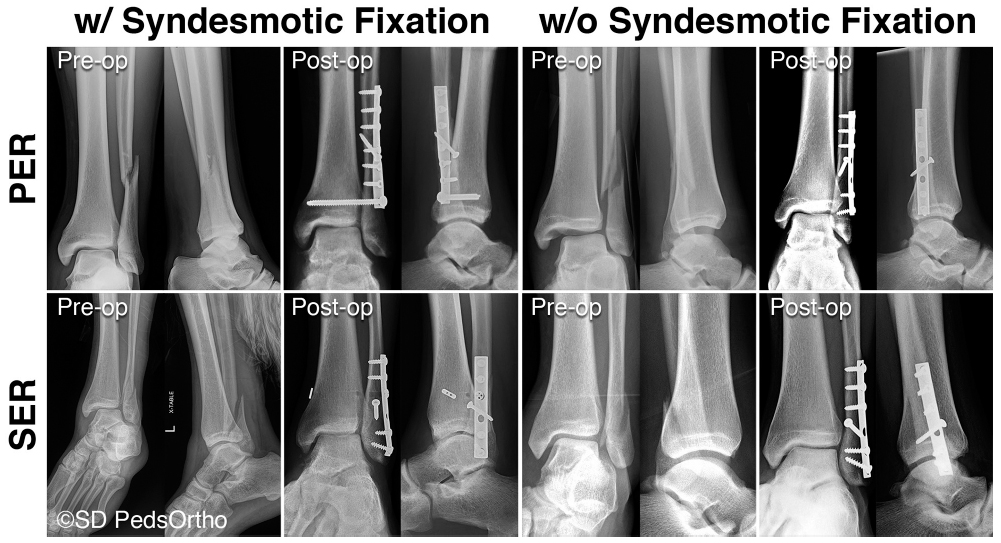
Four patients demonstrating the supination-external rotation (SER) and pronation-external rotation (PER) fracture patterns both with and without syndesmotic fixation in pre- and postoperative radiographs.
Demographics, radiographic and surgical data
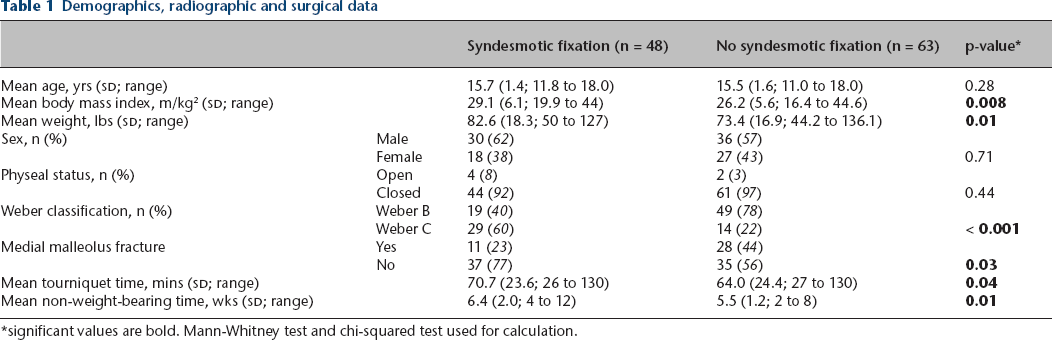
significant values are bold. Mann-Whitney test and chi-squared test used for calculation.
There were 68 Weber B and 43 Weber C fractures. Weber C fractures were significantly more common in the SF group than the no SF group (60.4% versus 22.2%; p < 0.001). Medial malleolus fractures were significantly less common in the SF group (p = 0.03). All patients went on to osseous union. As expected, the SF group had a significantly longer mean tourniquet time of 71 minutes compared with 64 minutes (p = 0.04) due to the additional reduction and fixation.
The activity at time of injury was determined for all patients, and the percentage of patients involved in this activity was compared between the SF versus no SF group as follows: football/collision sport (12.50% versus 12.70%), soccer (18.75% versus 6.35%), injury in rigid ankle immobilization (8.33% versus 12.70%), softball/baseball slide (4.17% versus 6.35%), ground-level fall (8.33% versus 20.63%), fall walking downhill (2.08% versus 4.76%), fall from height (12.50% versus 6.35%), skateboarding/scooter (27.08% versus 19.05%) and motor vehicle collision (6.25% versus 9.52%).
The SF group was more likely to undergo any implant removal than the no SF group (56.3% versus 15.9%; p < 0.0001). Of the 48 patients in the SF group, 27 patients underwent syndesmosis fixation hardware removal (24 had been treated with a syndesmotic screw, three with a suture-button). Mean time of syndesmotic screw removal was 3.68 months (SD 1.51; range 1.50 to 8.40) Mean time to suture-button removal was 9.20 months and coincided with the removal of the fibula implants in all cases. The two groups did not differ significantly in regard to need for second surgery other than implant removal.
There was no significant difference in complication rates between the groups (p = 0.91). In the SF group, one patient treated initially with a 3.5-mm tricortical syndesmotic screw underwent revision open reduction internal fixation of the syndesmosis with a suture-button due to inadequate reduction of the syndesmosis and persistent medial clear space widening. Furthermore, the SF group had two superficial surgical site infections, one stitch abscess and one case of postoperative fourth toe numbness. In the no SF group, there were three stitch abscesses and one wound dehiscence requiring irrigation, debridement and closure. One patient also underwent operative scar revision.
The SF group had longer non-weight-bearing restrictions (mean 6.4 weeks; SD 2.0; range 4 to 12) than the no SF group (mean 5.5 weeks; SD 1.2; 2 to 8) (p=0.01). There was no significant difference in return to sport rates between the two groups with rates of return to sport of 89.6% and 92.4% in the SF and no SF groups respectively (p = 0.44).
Comparison of functional outcomes
All patients had functional outcomes collected with the FAAM score at a minimum of one-year after surgery with mean follow-up in SF group of 46.9 months (SD 25.2; range 12 to 106) and in no SF group of 54.5 months (SD 26.6; range 12 to 99). There was no difference in functional outcomes between the SF and no SF groups: mean FAAM ADL score 96.8% (64.3% to 100%) versus 97.5% (72.6% to 100%) (p = 0.32); mean FAAM Sports score 91.6% (21.4% to 100%) versus 92.8% (53.6% to 100%) (p = 0.19). There was also no statistically significant difference between the SF and no SF groups on the SANE ADL or SANE Sports scores: mean SANE ADL 92.1% (40% to 100%) versus 95.5% (75% to 100%) (p = 0.07); mean SANE Sports 85.3% (20% to 100%) versus 88.5% (50% to 100%) (p = 0.16). Satisfaction scores were identical between the groups with both averaging 9.67 out of 10 (p = 0.47). The outcome data is presented in Table 2. The patients were also stratified by Weber grade and analyzed independently to evaluate for differences in outcomes in SF and no SF groups based on fracture pattern (see Table 3), which did not demonstrate any difference.
Functional outcomes and complications
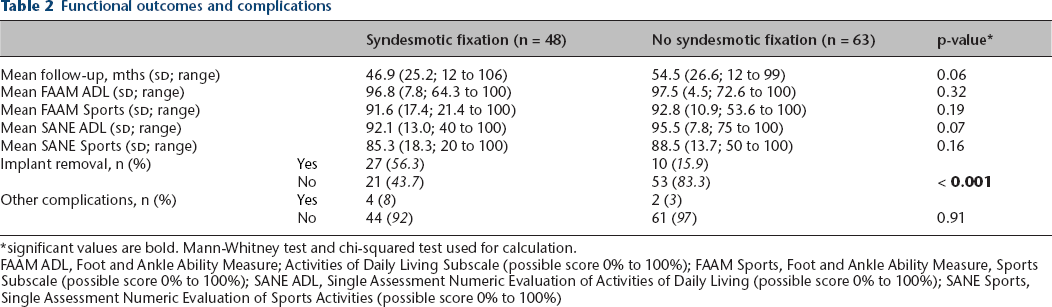
significant values are bold. Mann-Whitney test and chi-squared test used for calculation.
FAAM ADL, Foot and Ankle Ability Measure; Activities of Daily Living Subscale (possible score 0% to 100%); FAAM Sports, Foot and Ankle Ability Measure, Sports Subscale (possible score 0% to 100%); SANE ADL, Single Assessment Numeric Evaluation of Activities of Daily Living (possible score 0% to 100%); SANE Sports, Single Assessment Numeric Evaluation of Sports Activities (possible score 0% to 100%)
Functional outcomes based on Weber B and Weber C classification
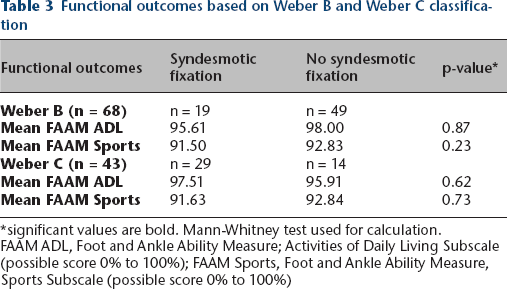
significant values are bold. Mann-Whitney test used for calculation.
FAAM ADL, Foot and Ankle Ability Measure; Activities of Daily Living Subscale (possible score 0% to 100%); FAAM Sports, Foot and Ankle Ability Measure, Sports Subscale (possible score 0% to 100%)
Patient outcomes were also compared based on sex. There was no difference in the incidence of SF between male and female patients (p = 0.71). Male patients had a significantly older mean age of 16.05 years (SD 1.22; range 12.29 to 18.0) versus 14.89 years (SD 1.76; range 10.94 to 18.04) in females (p = 0.0001) and significantly lower BMI of 26.57 (SD 5.51; range 17.0 to 44.6) versus 28.84 (SD 6.32; range 16.4 to 41.8) (p = 0.02). Male patients on average weighed more than female patients with a mean weight of 78.28 kg (SD 17.18; range 52.0 to 136.1) versus 76.08 kg (SD 19.09; range 44.2 to 113.4), although this difference was not significant (p = 0.25). Female patients had significantly lower patient-reported outcomes scores: mean female FAAM ADL score 95.5% (64.3% to 100%) versus 98.3% (66.7% to 100%) (p = 0.0004) in male patients; FAAM Sports score 87.4% (21.4% to 100%) versus 95.6% (45.8% to 100%) (p = 0.001); SANE ADL 89.7% (40% to 100%) versus 96.1% (75% to 100%) (p = 0.006); SANE Sports 80.6% (20% to 100%) versus 90.5% (50% to 100%) (p = 0.009). There was no significant difference between male and female patients in terms of satisfaction (p = 0.17), tourniquet time (p = 0.40), follow-up time (p = 0.33) or immobilization time (p = 0.37). There was a small difference in non-weight-bearing time, with female patients averaging less (mean 5.58 weeks; SD 1.47; range 4 to 12) versus males (mean 6.03 weeks; SD 1.73; range 2 to 12) which approached significance (p = 0.057).
A multivariable linear regression model was developed with FAAM Sports score as the dependent variable. The variables in the model were selected from nine possible predictors using backward stepwise regression. After all variables that were not significant predictors of outcome were eliminated, the model had three variables: sex, BMI and months of follow-up. While SF was not a significant predictor, this was manually added back to the model to help answer the central clinical question of this study. The adjusted r-squared of the model was 0.17. Male sex, lower BMI and longer duration of follow-up were positive predictors of functional outcome. Male sex conferred a 6.8% higher FAAM Sports score (p = 0.018). A one-point increase of BMI conferred a 0.8% lower FAAM Sports score (p = 0.001). A one-month increase in follow-up time conferred a 0.1% higher FAAM Sports score (p = 0.036). SF was not a predictor of functional outcome (p = 0.545).
There were six patients in the study that were skeletally immature, defined as open physes on ankle imaging. Of those six patients, four were in the SF group and two were in the no SF group (p = 0.44). Due to the small sample size, no statistical comparisons between the skeletally immature SF and no SF patients were made. However, when comparing the skeletally immature with the mature patients, the immature patients trended towards better functional outcome scores (mean FAAM ADL 99.4% (SD 0.92; range 97.6% to 100%) versus 97.1% (SD 6.24; range 64.3 to 100); mean FAAM sports 100% (SD 0; range 100% to 100%) versus 91.9% (SD 14.21; range 21.4% to 100%); mean SANE ADL 96.7% (SD 3.73; range 90% to 100%) versus 93.6% (SD 11.07; range 40% to 100%); mean SANE sports 92.5% (SD 4.79; range 85% to 100%) versus 86.5% (SD 16.56; range 20% to 100%). The four skeletally immature patients requiring SF in our study consisted of two patients with isolated fibula fractures and two patients with trimalleolar fractures. All fibula fractures in the patients were classified as Weber B. Mean age was 14.28 years (SD 1.48; range 12.29 to 16.37 years). Activities causing the injuries were two instances of another person falling on the patient (one on trampoline and one playing football) and two were skateboarding injuries. The two skeletally immature patients that did not require SF were both bimalleolar fractures with Weber B fibula fractures and concomitant medial malleolus fractures. One was caused by jumping on a trampoline and another from falling off a motorized dirtbike.
Discussion
The purpose of the current study was to compare outcomes between operative ankle fractures that did and did not require fixation of the syndesmosis. We found that patients requiring SF had longer tourniquet times, length of weight-bearing restrictions and rates of implant removal but had equivalent functional outcomes, rates of return to sport and overall satisfaction. In order to identify potential variables that independently impact functional outcome, we developed a multivariable linear regression, which found male sex, lower BMI and longer follow-up time to be independent positive predictors of FAAM Sports score, and also found that SF did not predict outcome.
FAAM Sports score was chosen as the dependent variable because it was available for all patients and had a greater variation in score between patients, unlike FAAM ADL score which was excellent in nearly all patients. After backward stepwise elimination was performed, male sex, lower BMI and months of follow-up were positive independent predictors of FAAM Sports score. The remainder of the potential predictor variables (follow-up time, medial malleolus fracture, skeletal maturity, complications, immobilization time, Weber grade and BMI) were excluded from the model. Male sex conferred a 6.8% higher FAAM Sports score (p = 0.018). A one-point increase of BMI conferred a 0.8% lower FAAM Sports score (p = 0.001). A one-month increase in follow-up time conferred a 0.1% higher FAAM Sports score (p = 0.036). This is consistent with Still and Atwood 29 who found that in 41 operative ankle fractures, male sex significantly increased likelihood of scoring higher on the subjective outcome scale, however, in that study, the female cohort was statistically significantly older than the male cohort. The sex difference in functional outcomes of our study may also be explained by a difference in biological mechanisms of pain and psychosocial factors, which have been previously described.33,34 With BMI ranging from 16 to 44 and follow-up ranging from 12 months to 106 months in our cohort, the small regression coefficients could still signify a clinically relevant difference. With the linear modelling used, we are not able to determine at what level higher BMI has the greatest effect on outcome, or for how long patients continue to improve after one-year follow-up. Future studies with larger cohorts and/or the use of polynomial regression, or measuring outcomes at multiple time points in the same patients could provide additional information.
Our finding that operative ankle fractures with and without SF had equivalent functional outcomes differs from some studies in the adult population.19,26–29 Egol et al 27 conducted a large study on 347 patients with unstable ankle fractures, finding that those with SF had significantly worse functional outcome and pain scores at minimum one-year follow-up. Still and Atwood 29 also found that fractures requiring SF had worse functional outcomes. The literature is mixed, however, and other studies have not demonstrated a difference in functional outcome. Veen and Zuurmond 26 compared ankle fractures requiring SF with those that did not at six-year follow-up. They found a trend towards higher functional outcome scores and lower incidence of joint degeneration in their SF versus no SF groups (86.7% versus 55.5%) although their sample size was small and not statistically significant. Kortekangas et al 28 found no difference in radiological or clinical outcomes at four to six years in SER IV (Weber B) fractures that did and did not require SF. While the effect of syndesmotic injury on functional outcome in the adult population remains unclear, data on adolescent syndesmotic injuries is even more limited. Lamer et al 19 reviewed 128 paediatric ankle fractures but only identified 11 patients that underwent SF and found similar functional outcomes at approximately one-year follow-up. Our study had a much higher proportion of skeletally mature adolescents that required SF and, therefore, we were able to perform an adequately powered comparison between adolescent ankle fractures treated with and without SF. While there was a trend towards a lower mean SANE ADL score in the SF group (92.1% versus 95.5%; p = 0.07), this potential difference is significantly lower than the MCID of the outcome tool and unlikely to be clinically significant.35,36
Previous studies have shown a strong correlation between syndesmotic injury and Weber C fracture patterns. Egol et al 27 found that 79% of the Weber C fractures in their study required syndesmotic stabilization compared with 18% of Weber B fractures. Veen and Zuurmond 26 found that 88.5% of the patients requiring SF group were Weber C, compared with 51.5% in the no fixation group. Kramer et al 13 found that 76% of their patients with syndesmosis injury and concomitant fracture had a Weber C fracture pattern. Our study further supports these findings, with 60.4% of our SF group having a Weber C fracture compared with only 22.2% in the no SF group. In addition, our study found that mean BMI was significantly higher in the SF group compared with the no SF group. It is possible that a higher BMI could cause relatively higher forces during injury and thus be associated with higher rates of syndesmotic injury.
It is known that the ankles of paediatric patients behave very differently than adults during injury. The ligaments are stronger than the physeal plate, which often leads to fractures over purely ligamentous injury.19,37 Furthermore, an open distal tibial physis is believed to result in Salter Harris type I or II injuries but as the physis closes, ligamentous injuries and transitional fractures become more common.11,38 Kramer et al 13 supported this theory of the protective nature of an open physis against purely ligamentous injury requiring surgical fixation. Their study found syndesmotic injury requiring fixation to be associated with a closed distal physis and concomitant fibular fracture. Lamer et al's 19 findings are also consistent with this, observing that there were no syndesmotic surgical repairs in their skeletally immature or transitional groups. They suggested that these injuries are either nearly non-existent in these young skeletally immature patients or that they cannot be diagnosed accurately with current techniques. In our study, however, we identified four patients (3.5%) with open physes who had a syndesmotic injury identified by routine intraoperative testing of the syndesmosis. We, therefore, conclude that while syndesmotic injury is indeed rare in skeletally immature patients, clinicians should remain suspicious in rotational ankle fracture and perform thorough intraoperative testing of the syndesmosis.
There are a number of limitations in this study. First, it is a retrospective study and the quality of the data is likely lower than that found in a prospective cohort. Additionally, functional outcome was assessed by patient-reported outcome scores. Future studies including objective data on strength and range of movement could provide valuable information. Another potential limitation to the study's external validity is that the intraoperative diagnosis of syndesmotic injury at other facilities may be different than the method used at our centre. While our average follow-up of 4.35 years is likely to capture the immediate effects of the injury on ankle function, it may be too short to detect the long-term effects of altered tibiofibular joint mechanics and post-traumatic arthritis. Lastly, the number of skeletally immature patients with syndesmotic injuries was small and thus it is difficult to draw strong conclusions about these patients.
In conclusion, adolescent patients requiring surgical fixation of the syndesmosis are likely to have equivalent outcomes and rates of return to sport at short- to medium-term follow-up compared with those without syndesmotic injuries. Male sex, lower BMI and longer follow-up time (within our follow-up range of one to eight years) are independent positive predictors of functional outcome, whereas SF is not a predictor of functional outcome.
Footnotes
BML: Study design, Data acquisition, Data analysis, Interpretation of data.
VVU: Interpretation of data.
ATP: Study design, Interpretation of data.