
Abstract
Abstract
In patients with immature skeletons, ligamentous injuries rarely accompany ankle fractures. In this article, we report about deltoid ligament tears and syndesmotic disruptions accompanying triplane ankle fractures in two children, and make recommendations as to the evaluation and treatment of children with such injuries.
Introduction
The original description of triplane ankle fractures has been attributed to Bartyl [1]. In 1957, Johnson and Fahl [2] reported a series of 27 physeal ankle injuries that included 10 such injuries. However, Marmor is credited as being the first to recognize the pathological anatomy of triplane ankle fractures; he reported that they were three-part fractures [3]. Subsequently, in 1978, Cooperman et al. [4] published an article stating that, based on tomographic evaluations, most triplane fractures actually consisted of two parts. Since that time, there have been several studies that have further characterized the bony anatomy of these injuries, including Karrholm's description of four-part triplane fractures, Denton and Fischer's description of two-part medial triplane fractures, Peiro's description of three-part medial triplane fractures, and Von Laer's description of intra malleolar triplane fractures [5–8]. The purpose of this report was to document two patients who had deltoid ligament tears and syndesmotic disruptions associated with triplane ankle fractures.
Case 1
A 12-year-old female presented to her local emergency room for evaluation of an injury to her right ankle, which she sustained when she slipped while running. On examination, she had marked swelling of the involved ankle. In addition to anterior, lateral, and posterior tenderness, she had discomfort about the medial malleolus. She had intact pulses and was neurologically intact. Radiographs revealed a three-part triplane fracture, a fibular fracture, and lateral displacement of the talus relative to the medial malleolus (Fig. 1). She was placed in a well-padded splint, and the extremity was elevated for the next 10 days to allow her swelling to subside. She was then taken to the operating room. The posterior Salter Harris-II fragment of her fracture was openly reduced and fixed with a screw placed from the anterior lateral aspect of the distal tibia into the metaphyseal portion of the Salter Harris-II fragment. The Tillaux fragment was then reduced and fixed with a screw inserted from the medial side of the distal tibia into the Tillaux fragment. An antero–posterior (AP) fluoroscopic view of the ankle made with an external rotation stress applied through the foot to the ankle after the two screws had been placed was deemed to reveal mild widening of the ankle mortise (Fig. 2). A syndesmotic screw was therefore inserted to further stabilize the ankle mortise and syndesmosis (Fig. 3). Additional fixation of the fibular fracture was not deemed to be necessary.

Antero–posterior (AP) and lateral ankle radiographs demonstrating a three-part triplane fracture with widening of the space between the medial malleolus and talus and widening of the syndesmosis

Antero–posterior (AP) radiograph after open reduction and internal fixation of the triplane fracture showing mild residual widening of the ankle mortise

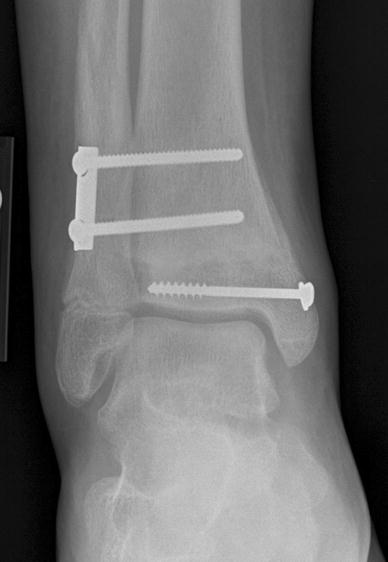
Antero–posterior (AP) radiograph after the addition of a syndesmotic screw showing restoration of the ankle mortise
Case 2
A 12-year-old boy fell from a scooter, injuring his left ankle. Examination revealed moderate swelling of his ankle. In addition to anterior lateral tenderness, the patient was found to have tenderness about the medial malleolus. X-rays revealed a two-part triplane ankle fracture associated with a fibular fracture. The patient was taken to the operating room. Fluoroscopic examination of the ankle revealed widening of the ankle mortise and syndesmosis with external rotational stress testing (Fig. 4). The fixation of the syndesmosis achieved by fixation of the triplane fracture was supplemented with two syndesmotic screws (Fig. 5).

Lateral and antero–posterior (AP) stress ankle radiographs demonstrating a two-part triplane fracture with widening of the space between the medial malleolus and the talus and widening of the syndesmosis
Antero–posterior (AP) radiograph after open reduction and internal fixation of triplane fracture and placement of two syndesmotic screws
Discussion
It is generally agreed that triplane ankle fractures are the result of an external rotation force applied to the ankle through a supinated foot [5]. While the bony anatomy of triplane ankle fractures has received considerable attention, review of the English literature reveals that little attention has been paid to the possible existence of significant ligamentous injury associated with these fractures.
Kleiger and Mankin [9] postulated that the anterior tibiofibular ligament was responsible for avulsing the anterior lateral distal tibia in juvenile Tillaux fractures and that a similar mechanism accounted for the anterior lateral fragment in three-part triplane fractures. They did not comment on whether ligamentous disruption might accompany these fractures. Peiro, however, did mention the possibility that the deltoid ligament could be torn in association with triplane ankle fractures, although did not present any documented case of such a tear [7].
In 1996, Healy et al. [10] reported on a patient who had a triplane ankle fracture associated with a proximal third fibula fracture. The authors speculated that in such Maisonneuve equivalent injury, deltoid ligament rupture and syndesmotic disruption could occur. However, neither was documented preoperatively in their case report. Stress testing of the syndesmosis after fixation of the triplane fracture revealed no instability and therefore a syndesmotic screw was not inserted. The authors concluded that since in such injuries the anterior–inferior tibiofibular ligament is intact and attached to the Tillaux fragment, bony fixation of the tillaux fragment can be expected to reconstitute the syndesmosis.
The two patients presented here are, to my knowledge, the first with documented deltoid ligament ruptures and syndesmotic disruptions associated with triplane ankle fractures to be presented in the English literature. Both injuries had associated fibular fractures, probably indicating that they were the result of higher levels of energy than triplane ankle fractures without associated fibular fractures. In both cases, reduction and internal fixation of the Tillaux fragment significantly improved the stability of the syndesmosis. In case 1, repeat stress testing after fixation of the Tillaux fragment was deemed to demonstrate mild residual instability of the syndesmosis. Based on the degree of instability demonstrated by the patient's preoperative radiographs, disruption of the posterior tibiofibular ligament and complete disruption of the interosseus ligament below the level of the fibular fracture were deemed to exist. Therefore, a syndesmotic screw was inserted.
After considering these two cases, it is recommended that physicians look for tenderness about the medial malleolus in patients with triplane fractures. It is further recommended that stress evaluation of the integrity of the syndesmosis and the ankle mortise be performed in such patients. When widening of the mortise is demonstrated before fixation, it is important to document that fixation of the triplane fracture restores the ankle mortise and stabilizes the syndesmosis. If it does not, or if the operating surgeon wishes to supplement the fixation of the syndesmosis afforded by single screw fixation of the Tillaux fragment, fixation of any associated fibular fracture and/or stabilization of the syndesmosis may be appropriate.