
Abstract
Abstract
Purpose
The study aimed to develop a scoring system based on clinical and radiological findings to predict the risk of a sequential slipped capital femoral epiphysis (SCFE).
Methods
Paediatric patients with unilateral SCFE and at least two years of radiographic follow-up were screened for inclusion. Medical records were reviewed for multiple variables including age, gender, body mass index (BMI), stability of SCFE, and time to sequential presentation. Radiographic analysis included triradiate physeal status, Risser staging, superior epiphyseal extension ratio (EER), posterior epiphyseal angle (PEA), posterior sloping angle (PSA) and slip severity.
Results
In total, 163 patients (88 male, 54%, 75 female, 46%) met inclusion criteria. Of those, 65 (40%) with a mean age of 11.9 ± 1.3 years developed sequential SCFE at a mean of 9.8 ± 6.4 months after the initial slip. Eight independent variables were statistically different (p < 0.05) between unilateral and sequential groups. Following multivariate analysis, Risser stage and triradiate status were no longer significant and did not influence the strength of the final model (overall area under the curve (AUC) = 0.954) and were consequently excluded. We developed the PASS score using three radiographic parameters using chosen cut-off values that were close to their maximized value and weighted the point value assigned to each parameter based on the strength of predictor.
Conclusion
A PASS score of three or higher predicts a high probability of sequential SCFE with 95% confidence and may warrant prophylactic screw fixation. PASS score calculation can be used to predict a sequential SCFE and provide an objective method to determine the utility prophylactic screw fixation.
Level of Evidence
II
Keywords
Introduction
Slipped capital femoral epiphysis (SCFE) is a common hip disorder seen in adolescents. The exact cause of SCFE is currently unknown but biomechanical factors in the setting of obesity or endocrine disorders have been implicated. SCFE typically presents with unilateral involvement. The management strategy for the contralateral hip at the time of presentation is controversial. Some authors recommend routine prophylactic insitu pinning based on a 25% to 80% reported risk of sequential involvement.1–3 Others recommend close radiographic follow-up and observation since risks associated with prophylactic surgical treatment such as iatrogenic chondrolysis and avascular necrosis have been reported. 4
Many parameters have been proposed as predictive factors for contralateral, sequential SCFE including: skeletal maturity, 5 body mass index (BMI) 6 and magnetic resonance imaging (MRI) pre-slip parameters. 7 Femoral head/neck morphology, especially the posterior sloping of the epiphysis, has also been implicated.8–10 Previous studies have shown that the posterior sloping angle (PSA) of the physis on an axial radiograph is significantly higher in patients who progress to contralateral, sequential SCFE.11,12 Recent studies have shown that increasing capital femoral epiphyseal extension may confer physeal stability in the setting of SCFE, and that epiphyseal extension reflects an adaptive response to limit physeal stress and reduce the risk for progression to SCFE. 13 Therefore, patients with relatively less epiphyseal extension, and consequently decreased physeal stability, would be at an increased risk for the development of sequential SCFE. However, there is controversy regarding the appropriate thresholds of each parameter that would promote prophylactic fixation.
The purpose of this study was to determine the diagnostic value of a scoring system based on clinical and radiological findings for predicting sequential hip involvement in patients with unilateral SCFE and to develop an evidence-based clinical decision-making algorithm for the optimal management strategy of the contralateral hip.
Materials and methods
After institutional review board approval, a retrospective study was performed of all patients with unilateral SCFE treated at a single paediatric centre between 1st January 2000 and 31st December 2018. Patients who underwent contralateral prophylactic screw fixation, those with bilateral involvement at presentation, those with metabolic or endocrine disorders, or those without available preoperative images were excluded. Minimum follow-up requirement was complete at the time of contralateral SCFE, contralateral physeal closure or a follow-up of 24 months for patients with an open proximal femoral physis on their last radiograph. In total, 475 patients with a diagnosis of SCFE were identified between the years 2000 and 2018. Following exclusion criteria, 163 patients with unilateral SCFE were analysed: 65 patients (39.9%) developed contralateral, sequential SCFE and 98 (60.1%) remained unilateral (Fig. 1).
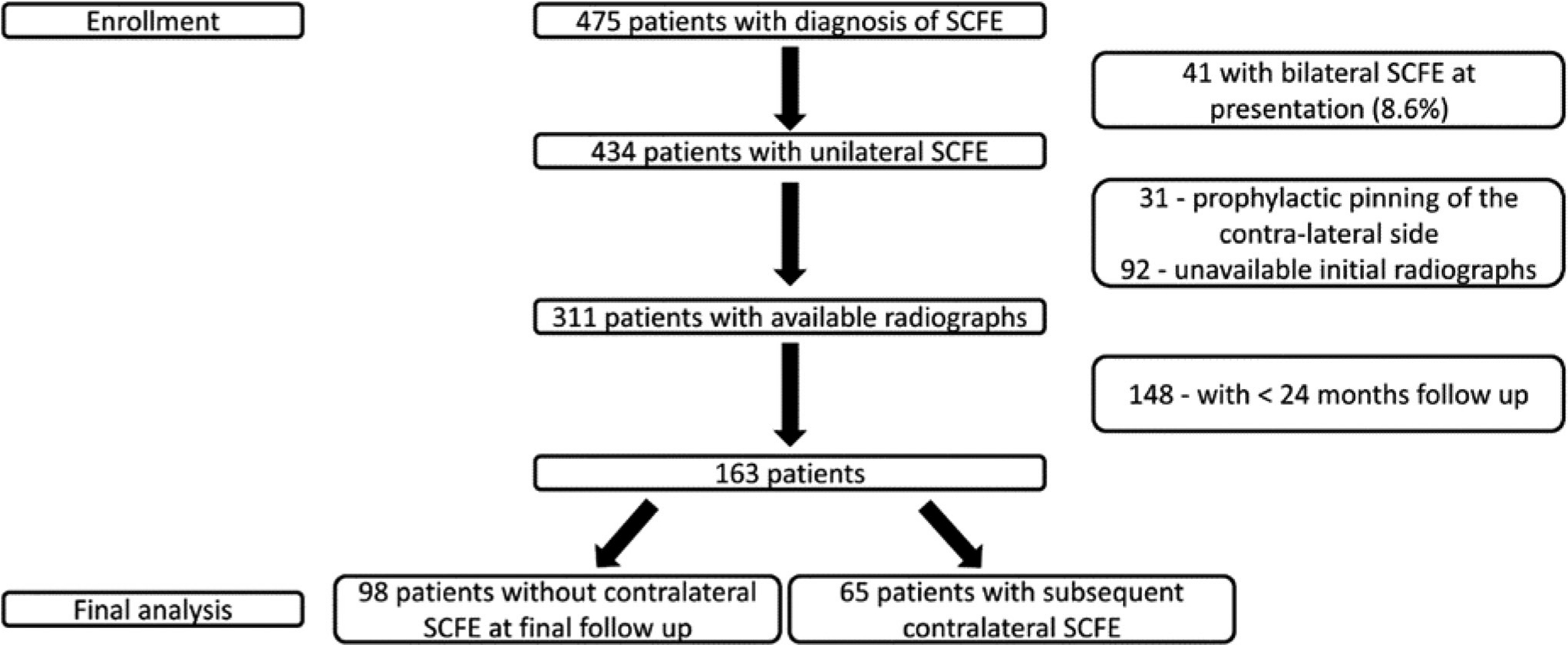
Study population.
Medical records were reviewed for gender, age at initial surgery, laterality, time to sequential presentation, SCFE clinical stability (as classified by Loder et al 14 ), height and weight. BMI percentile was calculated using the Centers for Disease Control and Prevention (CDC) website calculator 15 and categorized according to the guidelines of the CDC: 16 5th to 85th percentile considered normal or healthy weight, 85th to 95th percentile as overweight and 95th percentile or greater as obese.
Radiographic assessment was performed via the picture and archiving communication system (PACS) (GE Medical Systems, Barrington, Illinois) by a fellowship trained, paediatric orthopedic surgeon (BD) who was not clinically involved in patient care and blinded to the outcome of each hip. Measurements were repeated at approximately three months after the initial evaluation to test intra-rater reliability. Supine anteroposterior (AP) pelvic radiographs taken at initial presentation were available for all patients. Initial frog lateral pelvis radiographs – taken with the patient supine with both knees flexed at 45º, hips externally rotated and abducted 45º – were available for 149 (91%) of the 163 patients. The first postoperative frog lateral radiograph was used for the remaining 14 patients (9%).
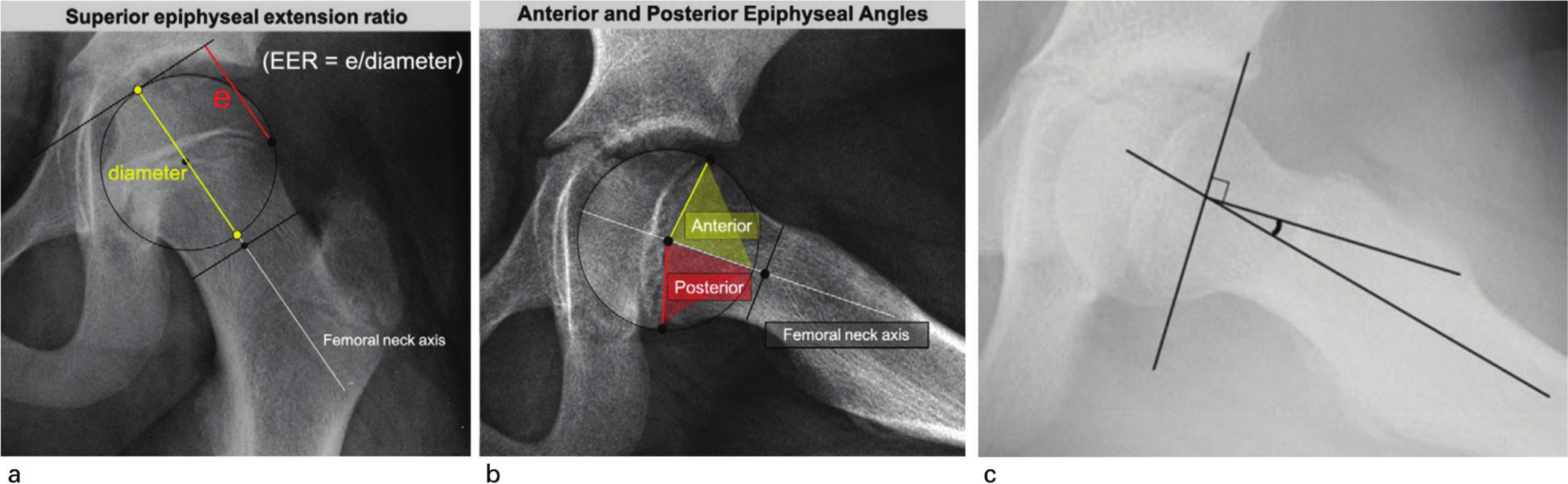
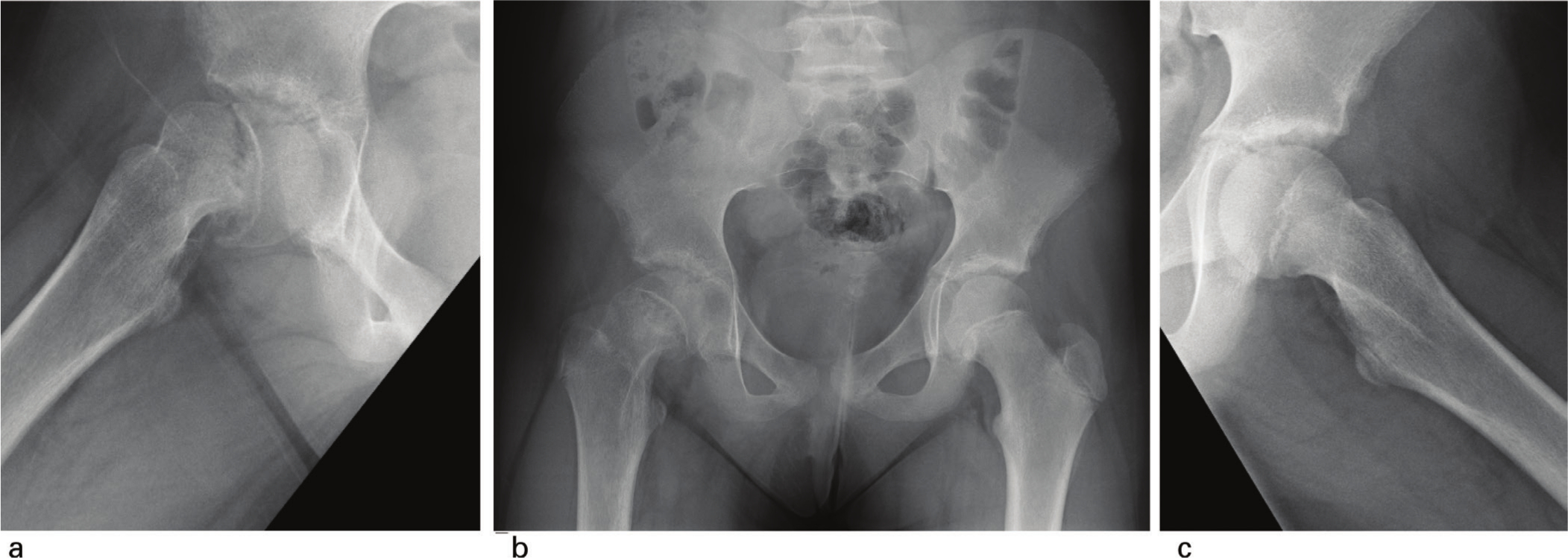
On the AP view, the triradiate cartilage status was labelled as open (grade I – more than 2mm width, grade II – less than 2mm width) or closed (grade III) as defined in the modified Oxford bone age score. 5 Risser stage was determined as described by Hacquebord and Leopold. 17 Superior epiphyseal extension ratio (EER) of the uninvolved hip at time of unilateral SCFE presentation (Fig. 2a) was calculated. On the frog lateral view, the posterior epiphyseal angle (PEA) (Fig. 2b) was measured for the uninvolved hip. The posterior sloping angle (Fig. 2c) was measured on the affected hip (initial PSA) and unaffected hip (PSA). Southwick angle of the involved hip was calculated by subtraction of the PSA on the unaffected hip from that on the affected hip.
Comparisons were made between the unilateral SCFE and the sequential SCFE groups. Categorical variables, triradiate status and Risser stage were converted to binary classifiers. Specifically, grade I and II triradiate were labelled ‘open’ and grade III ‘closed’. Risser stage was split into 0 and stages 1 to 4. Univariate analysis was performed using independent samples T test and Mann-Whitney U test for continuous variables. Chi-square test of proportions was used for categorical variables. The continuous variables were individually analysed via Receiver Operator Characteristic (ROC) curves for the cut-off value where the area under the curve (AUC) was maximized. Unadjusted logistic regression models were constructed with sequential SCFE as the outcome variable and the variables of interest as single dichotomous predictors. The AUC (c statistic) was derived for each logistic regression model and sensitivity, specificity, positive predictive value (PPV),and negative predictive value (NPV) were calculated.
Adjusted multivariate logistic regression was performed to create the final model upon which the Probability Analysis of Sequential SCFE (PASS) Score algorithm is based. Regression coefficients, adjusted odds ratios, 95% confidence intervals and adjusted p-values were determined. An adjusted p-value of less than 0.100 was considered acceptable for the final model. An ROC curve of the final model was constructed to assess the diagnostic performance of the combination of multivariate predictors in predicting sequential contralateral SCFE. The probabilities of sequential SCFE for each combination of predictors in the final model were calculated. Intra-rater reliability was assessed using a two-way random, single measures, absolute agreement (ICC (2,1)) model. A weighted point value was then assigned based on the strength of each predictor. Statistical analysis was performed with SPSS Statistics 26 (IBM Corp., Armonk, New York) and SAS Enterprise Guide 8.1 (SAS Institute, Cary, North Carolina) software packages.
Results
Univariate analysis
In total, 163 patients (88 male, 54%) with unilateral SCFE met the inclusion criteria. Of those, 65 patients (40%) developed contralateral, sequential SCFE at a mean of 9.8 ± 6.4 (range 0.5 to 27.9) months after the initial SCFE. Mean age at initial slip was younger in the sequential group (11.9 ± 1.3, range 9.3 to15.1 years) compared to the unilateral group (12.5 ± 1.6, range 7.7 to 16.7 years) (p = 0.025). There appeared to be a significant association between lower BMI and developing sequential SCFE: mean BMI was lower in the sequential SCFE group compared to the unilateral group (26.2 and 28.0kg/m2, respectively, p = 0.034). This association may be attributable to the lower age at initial slip of the sequential group: no difference was found between groups when utilizing the CDC BMI-for-age percentiles when comparing means (p = 0.398) or the distribution of obese and overweight patients (p = 0.735); thus, BMI was excluded from further analysis. Neither initial side of involvement (p = 0.159) or classification of clinical stability (p = 0.377) were significantly different between the groups.
Analysis of radiographic factors revealed that 72% of the sequential cohort had an open or closing (grade I or II) triradiate status compared to only 34% of the unilateral cohort (p < 0.001). Risser staging showed that 19% of the patients in the unilateral group had a Risser stage of one or higher, compared to only 3% of the patients in the sequential group (p = 0.002). The PSA of the affected hip was not a significant individual predictor of sequential SCFE (p = 0.200), however the PSA of the unaffected hip was higher in the sequential group (p < 0.001) (Table 1).
Univariate analysis
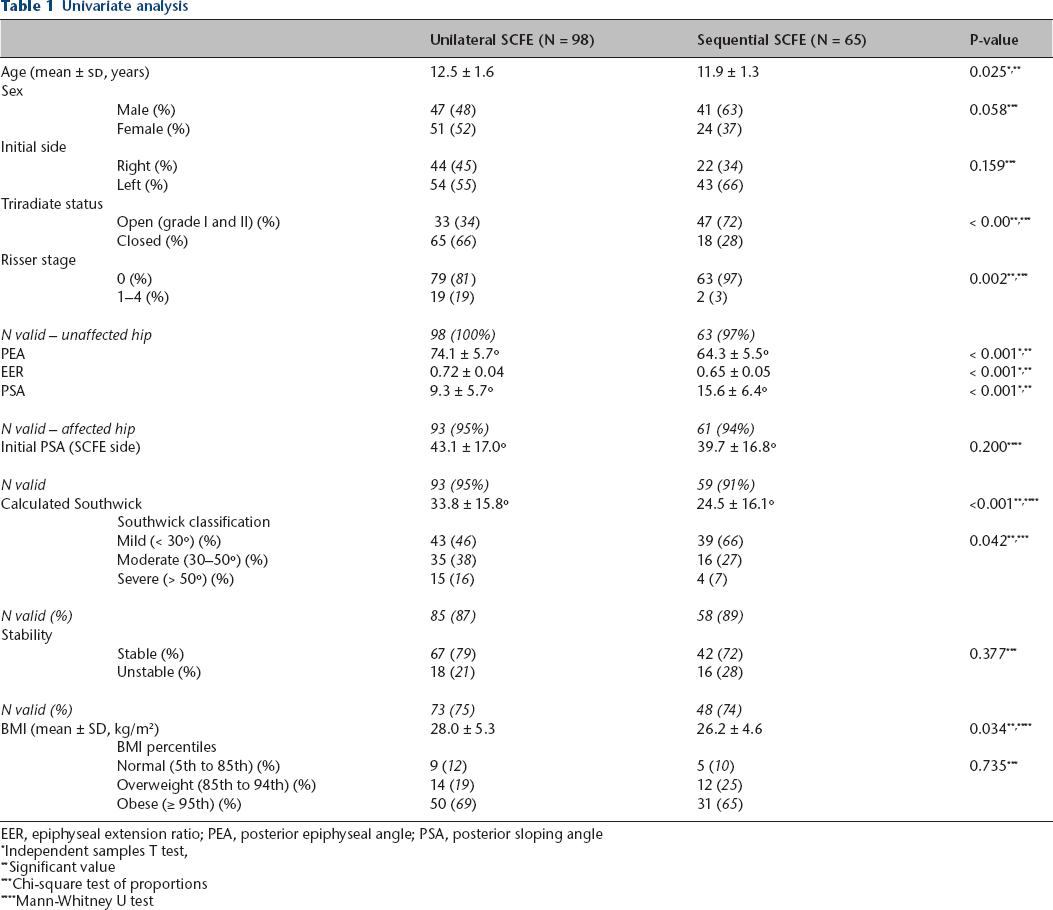
EER, epiphyseal extension ratio; PEA, posterior epiphyseal angle; PSA, posterior sloping angle
Independent samples T test,
Significant value
Chi-square test of proportions
Mann-Whitney U test
Seven independent variables were identified as significant individual predictors of sequential SCFE: age, triradiate status, Risser stage, calculated Southwick, PEA, EER and PSA. The unadjusted AUC provides the capability of each individual binary classifier to predict sequential SCFE. Sensitivity, specificity, PPV and NPV were also calculated (Table 2).
Expanded univariate and multivariate analysis (7 variable model AUC = 0.959)
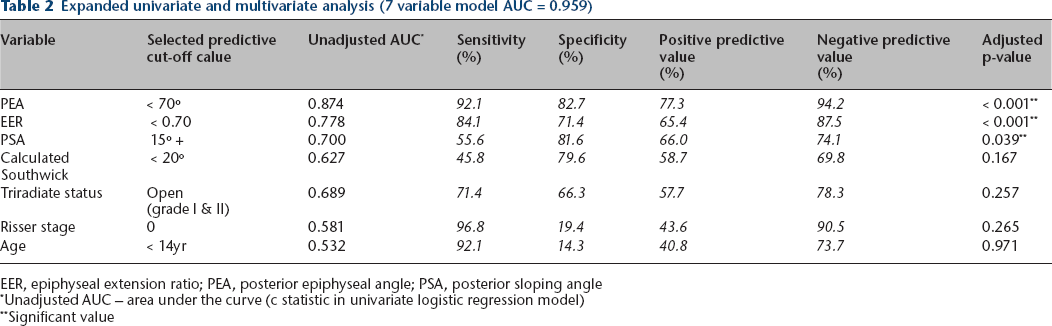
EER, epiphyseal extension ratio; PEA, posterior epiphyseal angle; PSA, posterior sloping angle
Unadjusted AUC – area under the curve (c statistic in univariate logistic regression model)
Significant value
Multivariate analysis
A seven variable adjusted multivariate logistic regression model was assessed via an ROC curve (AUC = 0.959) indicating excellent diagnostic performance. 18 Adjusted p-values revealed that calculated Southwick angle, triradiate status, Risser stage and age were no longer significant predictors of sequential SCFE (i.e. adjusted p > 0.100). Thus, they were excluded from the final model. A final model based on three radiographic measurements of the contralateral, uninvolved hip was assessed via regression coefficients, adjusted odds ratios, 95% confidence intervals and adjusted p-values (Table 3). The odds of a sequential SCFE were approximately 73.6 times greater when the PEA was less than 70º than when it was greater than 70º, with the lower and upper confidence limits of that estimation at 16.8 and 333.2, respectively (Table 3). A ROC curve of the final multivariate model revealed that removing the four other variables did not affect diagnostic performance significantly (ΔAUC = -0.005). An AUC of 0.954 suggests that the model will correctly predict the chance of sequential SCFE with over 95% accuracy (Fig. 3).
AP Pelvis
Final adjusted multivariate logistic regression model
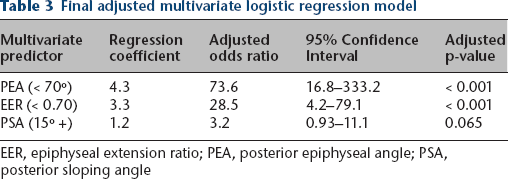
EER, epiphyseal extension ratio; PEA, posterior epiphyseal angle; PSA, posterior sloping angle
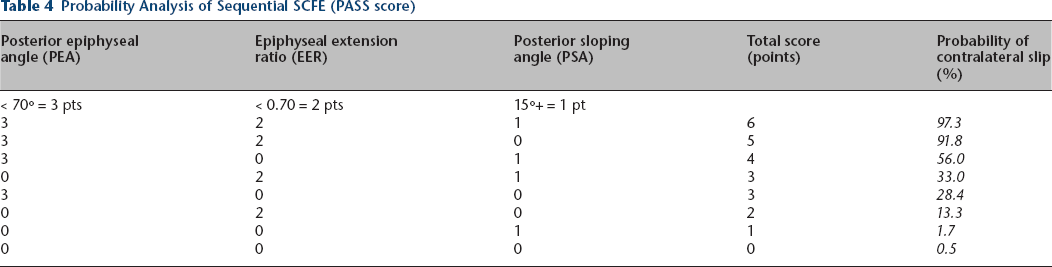
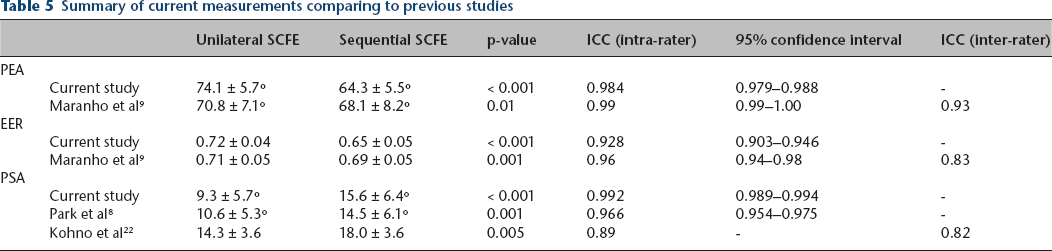
The predicted probability of sequential SCFE was determined on the basis of eight possible combinations (2 x 2 x 2) of the three radiographic predictors: PEA, PSA and EER. A weighted point value was assigned to each predictor based on diagnostic performance. PEA was the strongest predictor and assigned a point value of three. EER and PSA were weaker and assigned point values of two and one, respectively. A simplified clinical decision-making algorithm for the management of the contralateral hip, called the Probability Analysis of Sequential SCFE (PASS score), is shown in Table 4. Intra-rater reliability was excellent for all three radiographic measures (Table 5).
Probability Analysis of Sequential SCFE (PASS score)
Summary of current measurements comparing to previous studies
Discussion
The decision to perform prophylactic screw fixation on the contralateral hip in a patient who presents with a unilateral SCFE is controversial. Long-term studies have shown that even patients with mild deformity are at risk for subsequent labral tears and early arthrosis. However, the ability to predict sequential disease is critical since the surgeon must balance the iatrogenic risk associated with treating an otherwise normal hip against the perceived risk that the family will not reliably return for close radiographic monitoring of the uninvolved hip. Unfortunately, when conservative management is chosen, many families do not seek medical attention at the onset of pain in the contralateral limb despite warnings from the orthopedic providers. In some cases, even when proper precautions have been undertaken, sequential disease can occur without symptoms.
Previous studies have focused on the importance of age (chronologically and biologically) and on several radiographic parameters in an attempt to predict sequential SCFE. Riad et al 19 demonstrated that age at diagnosis is a risk factor for sequential SCFE. Authors recommend prophylactic in situ screw fixation in all girls younger than ten years of age and all boys younger than 12 years of age at presentation. Stasikelis et al 20 showed a linear distribution between the modified Oxford bone score and the risk of sequential SCFE. For male gender patients, the age at the time of the initial SCFE was predictive of a sequential slip.
Several studies have demonstrated the significance of the posterior sloping angle (PSA) of the unaffected hip in predicting sequential SCFE.8,10,12,21,22 Park et al 8 stated that PSA is predictive of sequential SCFE in patients presenting with unilateral SCFE. They recommend considering prophylactic screw fixation in females with PSA greater than13º upon presentation. Bellemore et al, 23 in a biomechanical study, presented data that supported the threshold of 15º PSA as an objective measure for prophylactic fixation of the contralateral hip.
Maranho et al 9 recently found superior epiphyseal extension ratio (EER) to be an independent factor associated with the likelihood of a sequential SCFE: for each 0.01 increase in the superior epiphyseal extension ratio, the odds of a sequential slip decreased by 6%. Our data showed similar results with predictability of the EER, however slightly less predictive of sequential slip when compared to the PEA.
The average degree of initial SCFE severity was significantly higher in patients with unilateral SCFE compared with patients who subsequently developed a sequential SCFE. These findings correlate with previous data from Loder et al 2 who reported patients with unilateral SCFE had higher degree deformity at presentation than those with sequential disease (34º versus 21º). Our data produced similar results with an average Southwick angle of 25° versus 34° for sequential and unilateral groups. Comparative data are summarized in Table 5. However, because the PSA of the unaffected hip was higher in the sequential group, the calculated Southwick angle (PSA affected – PSA unaffected) may have been falsely decreased.
Aversano et al 6 elucidated an association between BMI-for-age and risk for bilateral SCFE both at initial presentation and throughout the remaining growth period. They did not find a significant association between BMI-for-age and sequential slip after initial presentation. Nasreddine et al 24 found that patients whose BMI was decreased after initial slip were less likely to progress to bilateral SCFE.
In our study, mean BMI was lower in the sequential SCFE group compared to the unilateral group – 26.16 and 27.98 kg/m2, respectively (p = 0.05). Using the BMI-for-age percentile, shown to be more effective in evaluating obesity in the paediatric population, no difference was found in the distribution of patients between the unilateral and sequential groups. We suggest that there is not enough evidence to support BMI as one of the predictors for sequential disease.
A previous study sought to utilize MRI to evaluate contralateral SCFE upon presentation. 7 This study enrolled 33 patients from 2011 to 2013. In this study, six of 33 patients had positive MRI findings suggestive of a pre-slip. Of the six patients, four proceeded to sequential slip and two did not. Since 2013, subsequent results have shown that several patients in the ‘normal MRI’ cohort developed sequential SCFE. These patients are thought to represent true sequential disease rather than bilateral disease upon presentation. These outcomes were a driving force in the development of a more inclusive scoring system to predict patients at risk for sequential SCFE.
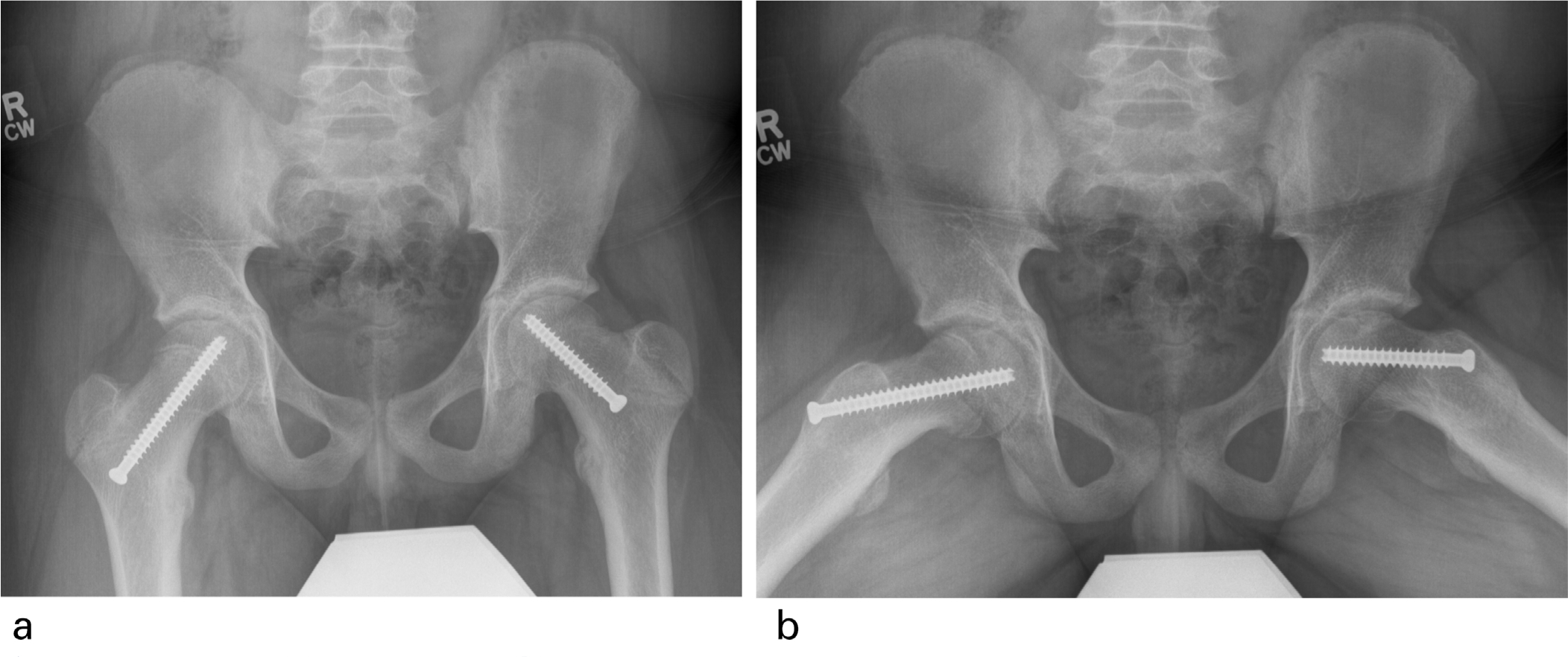
In addition, some may argue that higher initial PSA measurements in the asymptomatic ‘normal’ hip could suggest subclinical, bilateral disease at presentation. However, normal MRI findings at presentation would suggest otherwise. Lack of significant statistical power prevents this study from such conclusion and further study is needed. Due to these factors, MRI is no longer used routinely in our institution to guide treatment of the contralateral hip and was not utilized in our statistical analysis (Figs. 4–6).
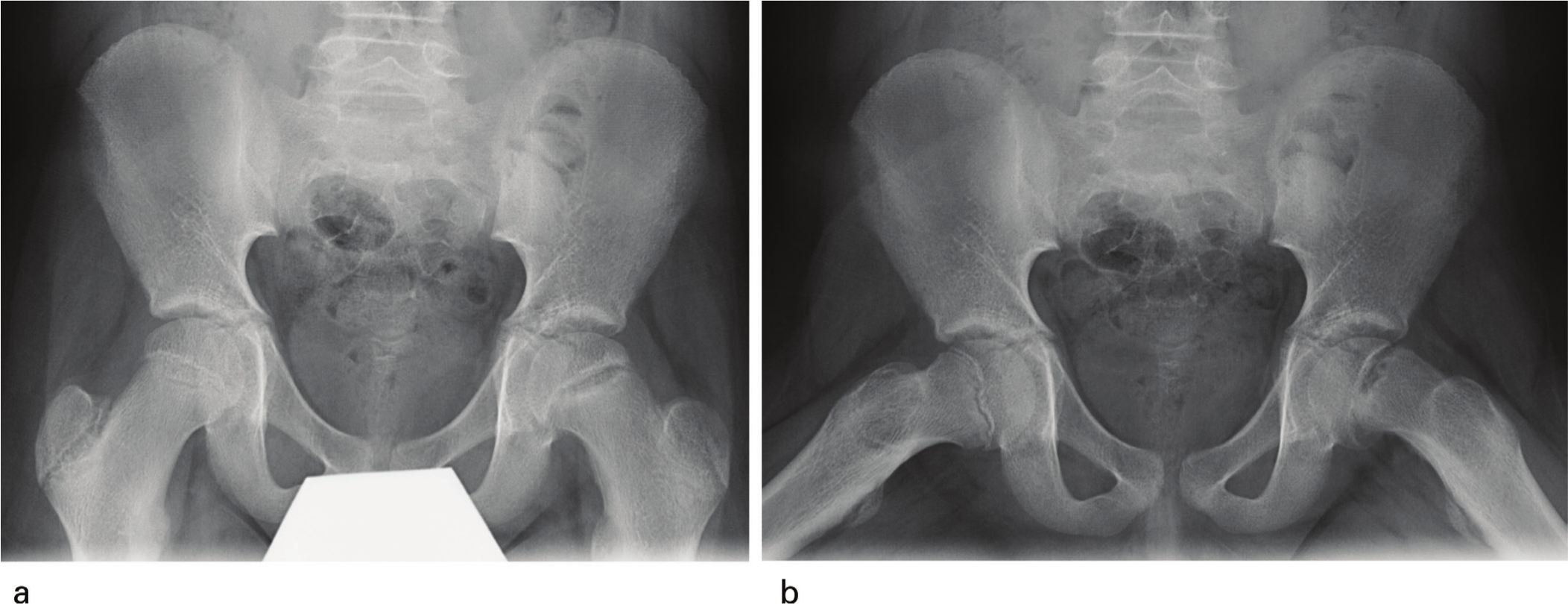
Anteroposterior
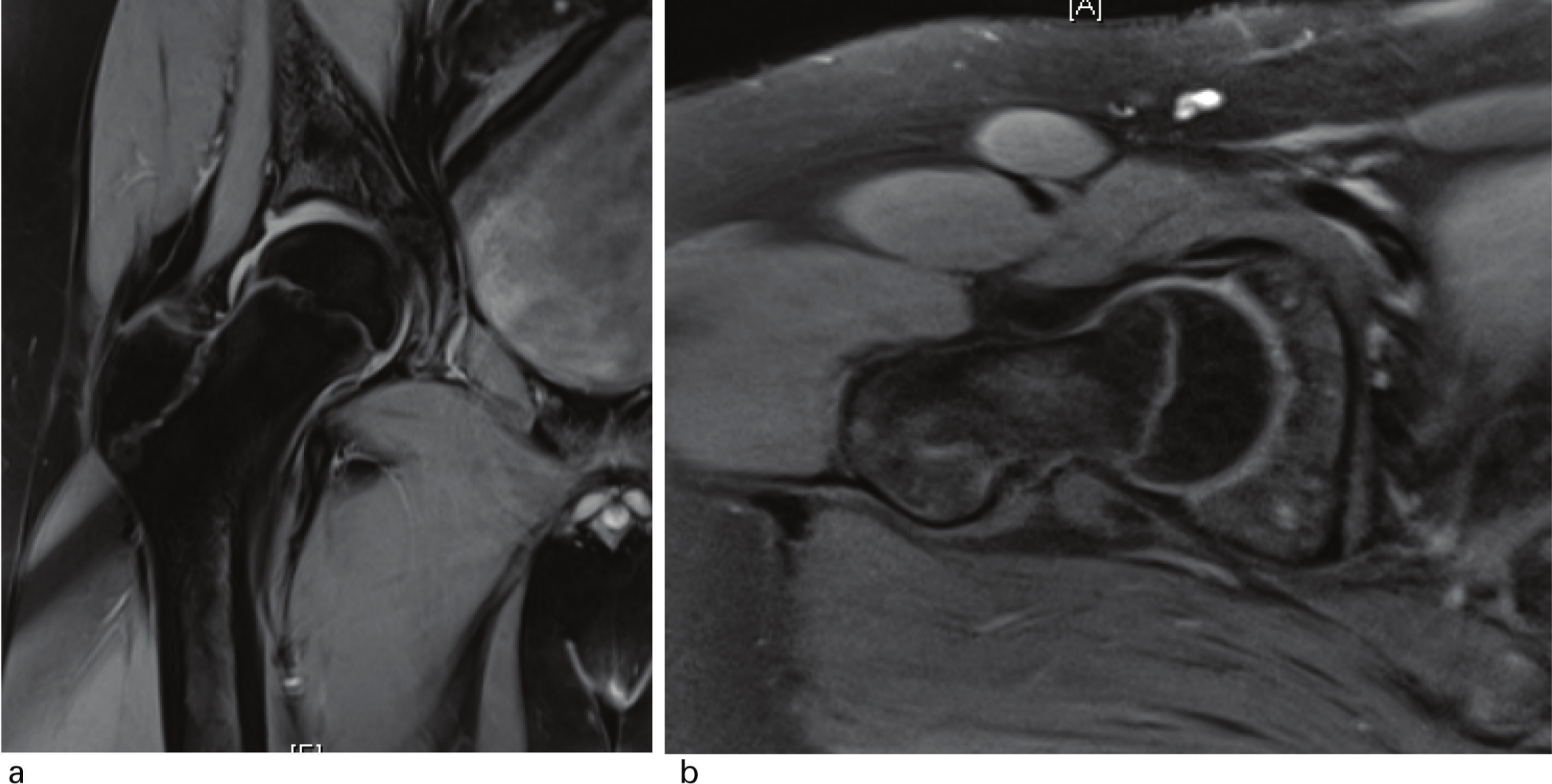
MRI images of contralateral right hip seen in Figure 4 at time of left hip presentation suggest no evidence of pre-slip on radial and axial oblique fat suppression sequences.
Anteroposterior
There are several limitations to this study. Due to its retrospective characteristics, the initial number of patients with SCFE decreased considerably – patients were excluded due to absent imaging studies and lack of adequate follow-up. BMI data were available for 75/98 (77%) from the unilateral group and 48/65 (74%) from the sequential group. Clinical stability was documented for 85/98 (87%) from the unilateral group and 58/65 (89%) from the sequential group. In addition, 31 (7.1%) of unilateral SCFE patients were treated with prophylactic pinning at the discretion of the treating surgeon(s) and therefore were removed from analysis. All such factors could potentially reduce the apparent impact of the common indications for prophylactic treatment including age and BMI. Nonetheless, this study comprises one the largest reported cohort of patients with sequential SCFE. A single reviewer of radiographic measurements may inherently lead to measurement inaccuracy and bias. However, this study and previous studies have shown strong intra-observer reliability for the measurements of PSA, PEA and EER (Table 5). Such studies have also shown strong inter-observer reliability. Furthermore, difficulty with radiographic reference points in obese patients requires both a significant time commitment and learning curve, and is aided by the radiographic system PACS, which is not universal at this time.
Although patients with open capital femoral physes were followed for a minimum of 24 months after the onset of unilateral SCFE, it is possible that patients in whom a sequential SCFE occurred after this period were not captured. In our patient cohort, the mean time to the sequential SCFE was 9.7 months, with 95% of cases of subsequent SCFE occurring in the first 24 months after initial SCFE. These data are compatible with the literature in which approximately 90% of cases of sequential SCFE have been reported to occur in the first few months after the diagnosis of initial SCFE. 2
Park et al suggested the difference in expected value between prophylactic pinning and observation was small. 8 Kocher et al performed a systematic review to determine outcome probabilities and to construct an expected-value decision analysis on the utility of prophylactic pinning of the contralateral hip after unilateral SCFE. Their results suggested that in the absence of endrocrinopathy, renal disease or unreliable follow-up, a probability of sequential disease exceeding 27% favours prophylactic pinning. The authors advocated a shared decision-making model between physician and patient. Given these data, clinical or radiographic methods of quantitatively assessing the risk of contralateral SCFE would be helpful to the clinician in deciding whether to observe or prophylactically pin the contralateral hip. A PASS score of three or higher suggests a 28% or higher probability of sequential SCFE, above the published threshold for prophylactic pinning. 25
Conclusion
There are several independent variables associated with sequential SCFE including triradiate status, Risser staging, initial SCFE severity, PSA, EER and PEA. Utilizing the radiographic measurements of the PSA, EER and PEA creates a clinically significant probability model for risk of the contralateral hip. A PASS score of three or greater predicts a high probability (28% +) of sequential SCFE and therefore may favour prophylactic screw fixation.
Footnotes
The other authors declare no conflict of interest.
SS: Substantial contributions to the conception and design of the work, Acquisition, analysis and interpretation of the data, Drafting of the work, Critical revisions to the manuscript.
JS: Substantial contributions to the conception and design of the work, Acquisition, analysis and interpretation of the data, Drafting of the work.
JY: Substantial contributions to the conception and design of the work, Acquisition, analysis and interpretation of the data, Drafting of the work.
WPS: Substantial contributions to the conception and design of the work, Acquisition, analysis and interpretation of the data, Drafting of the work; critical revisions to the manuscript.
CAI: Substantial contributions to the conception and design of the work, Acquisition, analysis and interpretation of the data, Drafting of the work, Critical revisions to the manuscript.
KEK: Substantial contributions to the conception and design of the work, Acquisition, analysis and interpretation of the data, Drafting of the work, Critical revisions to the manuscript.