
Abstract
Abstract
Purpose
Early diagnosis and treatment of slipped capital femoral epiphysis (SCFE) is important to prevent slip progression and avoid complications. We sought to determine if MRI findings in patients with unilateral SCFE could indicate ‘pre-slip’ or predict future SCFE in the contralateral hip.
Methods
A prospective study evaluated patients with unilateral SCFE over a two-year period. MRI of the asymptomatic hip was performed within the perioperative period. Patients were followed with radiographs until a contralateral slip occurred or until physeal closure. Demographics, clinical stability, severity, posterior slope angle (PSA), modified Oxford Bone Score (mOBS) and patency of the triradiate cartilage were recorded and statistical analysis performed.
Results
In all, 33 of 54 patients with unilateral SCFE were enrolled into the study. In all, 29 (87.8%) had complete follow-up. Five of the enrolled patients (15.2%) developed a sequential slip requiring in situ pinning. Six of 33 (18.2%) patients had positive MRI findings: four of which proceeded to sequential SCFE and two which did not. One sequential slip had a negative MRI. PSA predicted 1/11 sequential slips (sensitivity 9.09%, specificity 81.4%, positive predictive value (PPV) 11.1%, negative predictive value (NPV) 77.8%) and mOBS predicted 5/11 sequential slips (sensitivity 45.5%, specificity 93%, PPV 62.5%, NPV 87%). An open triradiate cartilage was present in 8/11 patients with sequential slips (sensitivity 72.7%, specificity 81.4%, PPV 50%, NPV 92.1%).
Conclusion
MRI findings consistent with ‘pre-slip’ were present in 66.7% of patients who developed a sequential SCFE. Further study on the utility/sensitivity of MRI in predicting sequential SCFE is warranted.
Level of Evidence
II, diagnostic
Keywords
Introduction
Slipped capital femoral epiphysis (SCFE) is the most common adolescent hip disorder. 1 Overall incidence of SCFE is 10.8 cases per 100 000 children with the average age of onset around 12 years sd 1.8.2,3 The cause of SCFE is unknown, but likely multifactorial, with both biomechanical and biochemical factors implicated.4–6 Higher than normal body mass index (BMI) and endocrine disorders have routinely been correlated with SCFE. 7
Early diagnosis and treatment of SCFE is important to prevent slip progression and avoid complications. Delays in diagnosis have been shown to lead to greater morbidity, including severe deformity, chondrolysis and avascular necrosis.7–9 Long-term morbidity includes pain, stiffness, limitation of flexion and internal rotation, cam impingement and eventually osteoarthritis.2,10,11
Studies investigating the bilaterality of SCFE report a prevalence of bilateral SCFE between 18% and 80%.3,12–18 However, the majority of patients present with unilateral SCFE. According to Hägglund et al, 14 only 9% of patients present initially with bilateral SCFE, whereas Loder et al 7 demonstrated bilaterality as high as 50% at initial presentation. It appears that bilateral SCFE will eventually occur in 50% to 61% of patients, as determined by long-term studies.18,19 Most sequential SCFE presents within 12 to 24 months of the initial slip.19,20
Given the high prevalence of bilateral involvement, diagnosis of unilateral SCFE warrants evaluation of the contralateral hip to assess for a possible simultaneous slip or ‘pre-slip’. Pre-slip of the capital femoral epiphysis is defined as ‘hip pain without radiographic evidence of SCFE in a child who, left untreated, would progress to SCFE’. 8 Other authors describe the presence of metaphyseal and physeal changes without demonstrated slip on conventional radiographs. 21 There is no standard method for determining pre-slip. MRI has not traditionally played a role in the diagnosis and treatment of SCFE, although it has been utilized to evaluate and diagnose complications of SCFE, such as chondrolysis and osteonecrosis. 22
Furthermore, controversy exists regarding how to address the contralateral side at presentation of unilateral SCFE. Management of the unaffected side involves monitoring the patient's plain radiographs and intervening if there are any radiographic changes or if symptoms develop. Whereas some surgeons describe a benefit of prophylactic screw fixation of the contralateral uninvolved hip,5,23 others recommend an observational approach. 8 Significant disadvantages of prophylactic, contralateral fixation include pin penetration, osteonecrosis, chondrolysis, infection and anesthesia risks.24–26
If an MRI could identify those hips at risk for slip progression or development of SCFE, unnecessary prophylactic treatment would be avoided. In addition, those patients identified with pre-slip could be treated prior to slip progression. The aim of this study is to determine if MRI findings of the unaffected hip in patients presenting with unilateral SCFE are predictive of sequential SCFE. A secondary aim is to compare previously described methods of predicting contralateral slips such as chronologic age of patient at presentation, open triradiate cartilage, modified Oxford Bone Age Score (mOBS) and posterior slope angle (PSA) with our MRI results. We hypothesize that there are MRI findings that will diagnose contralateral pre-slip and help predict sequential, contralateral SCFE in patients who present with unilateral SCFE.
Methods
Institutional Review Board approval was obtained. Parents or legal guardians signed informed consent for the patient to participate in the study. Inclusion criteria were: patients presenting with unilateral SCFE, asymptomatic contralateral hip exam and normal contralateral radiographs. Exclusion criteria were: 1) contraindications to MRI; 2) previously treated hips; 3) malignant disease; 4) bilateral SCFE on plain radiographs; 5) known endocrine disorders.
Patient demographics including age, gender, race, weight, height, BMI, comorbidities and previous radiation therapy were recorded. Clinical stability as described by Loder et al 7 was documented.
All patients received preoperative anteroposterior and frog-leg lateral pelvis radiographs as well as a contralateral hip MRI within a week of presentation. No treatment decisions were made based on the MRI findings, as the surgeons were blinded to the MRI results. MRI studies were reviewed in a blinded fashion by two fellowship-trained, paediatric musculoskeletal radiologists (BA, SD) who were masked to clinical information regarding duration of symptoms and demographic data. Inter-rater reliability was assessed. The morphology and signal intensity of the physis and the presence or absence of synovitis, effusion and bone marrow edema and any additional relevant findings were documented. Patients were then followed until physeal closure or until progression to contralateral SCFE.
Radiographic data were recorded and measured, including laterality, open or closed triradiate cartilage and degree of slip according to Southwick. mOBS was calculated as described by Stasikelis et al 27 . Slips were classified by severity according to the method described by Boyer et al; 28 mild SCFE (class I) less than 30°, moderate (class II) between 30° to 50° and severe (class III) if greater than 50°. PSA was determined as described by Barrios et al 29 Follow-up radiographs were assessed for contralateral disease or the presence of complications such as avascular necrosis and/or chondrolysis.
MRI protocol
MRI was performed to identify specific features that could carry prognostic implications for treatment and management of the contralateral hip. Femoral neck buttressing, physeal and periosteal continuity or disruption, focal or diffuse physeal widening, synovitis, bone marrow edema, joint effusion and periarticular edema were assessed. The MR imaging protocol employed coronal T1-weighted images of both hips and acetabulum, axial T2 fat-saturated images and coronal fast spin-echo inversion-recovery (FSEIR) images. 30 Axial oblique proton density (PD) fat saturated, and radial oblique PD fat sat sequences through the physis provided at least one image that included both the proximal femoral physis and the greater trochanteric physis. A diffusion sequence was performed so as to better define regions of abnormal water diffusivity found to be sensitive for cellular injury. 31 Gadolinium contrast enhancement was not utilized.
Statistical analysis
Comparisons between screening methods and the dichotomous covariates were conducted via Fisher's exact test or Pearson's chi-squared test. The previously described radiographic predictors of contralateral slips were analyzed and compared with our results, using MRI as our first predictor method. Secondary analyses were also performed to evaluate three different screening methods using the entire study population (excluding the patients who had bilateral pinning). Sensitivity, specificity, negative and positive predicted values were calculated for all four screening methods. IBM SPSS Version 21.0 (Chicago, Illinois) was utilized for statistical analyses. Statistical significance was defined as p < 0.05.
Results
A total of 69 SCFE patients (84 hips) were treated at our institution from 2011 to 2013; the mean age was 12.5 years (8.6 to 18.4), with 29 females and 40 males, and a mean follow-up of 1.69 years (0.1 to 4.0). Mean PSA was 11.4° (2.6° to 22.3°) and mean mOBS was 22 (16 to 26). In all, 15 patients (21.7%) presented with bilateral disease. This resulted in 54 unilateral SCFE patients for possible enrollment. A total of 16 of these patients (29.6%) presented with an open triradiate cartilage, and 38 (70.4%) presented with it closed (Table 1).
Patient demographics
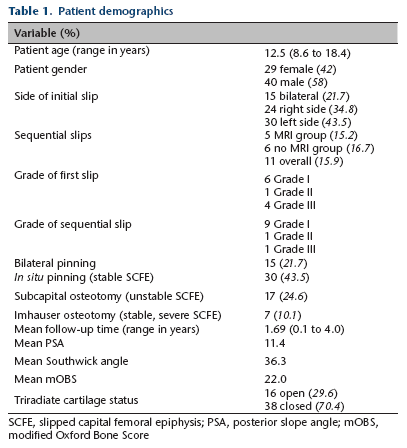
SCFE, slipped capital femoral epiphysis; PSA, posterior slope angle; mOBS, modified Oxford Bone Score
In all, 33 patients (61%) enrolled in the study. Excluded patients (n = 19) did not enroll for a variety of reasons: claustrophobia (two), custody issues (nine), weather (two), motion artifact (one), missed appointment (three), consent issues (two) or declined participation. In 29 of the 33 enrolled patients (87.8%) in the MRI group had complete clinical and radiographic follow-up.
In all, 11 patients (15.9%) developed a sequential SCFE, including six patients who did not undergo MRI evaluation. Five of the 33 enrolled patients (15.2%) developed a sequential slip requiring in situ pinning at an average of 10.4 months (five to 25) after initial presentation. Six patients (18.2%) had positive MRI findings: four sequential slips had positive MRI findings at the index procedure; two hips with positive MRI findings did not slip. One sequential slip had a negative MRI (sensitivity 80%, specificity 92.9%, positive predictive value (PPV) 66.7%, negative predictive value (NPV) 96.3%). There was 100% interrater reliability between the two musculoskeletal radiologists in the evaluation of pre-slip MRI findings, which findings included presence of focal or diffuse physeal widening and abnormal signal, and bone marrow edema adjacent to the proximal femoral physis.
The PSA predicted 1/11 sequential slips (sensitivity 9.09%, specificity 81.4%, PPV 11.1%, NPV 77.8%) and the mOBS predicted 5/11 sequential slips (sensitivity 45.5%, specificity 93%, PPV 62.5%, NPV 87%). An open triradiate cartilage was present in 8/11 patients with sequential slips (sensitivity 72.7%, specificity 81.4%, PPV 50%, NPV 92.1%). Combining an open triradiate cartilage with abnormal MRI results provided the most predictive information (sensitivity 80%, specificity 100%, PPV 100%, NPV 96.6%) (Table 2).
Screening test parameters

PPV, positive predictive value; NPV, negative predictive value; PSA, posterior slope angle; mOBS, modified Oxford Bone Score; TRC, triradiate cartilage
Chronological age (i.e. girls younger than ten years, and boys younger than 12 years) predicted 2/11 sequential slips (sensitivity 18.2%, specificity 88.4%, PPV 28.6%, NPV 80.9%). The mean age of patients presenting with unilateral SCFE who did not develop into bilateral involvement was 11.7 years (9.7 to 14.2) for girls, and 13.1 years (8.6 to 18.4) for boys. The mean age for patients who presented with unilateral SCFE and later developed a contralateral slip was 10.7 years (9.3 to 11.5) for girls, and 12.8 years (11.5 to 14.8) for boys. Grades of initial SCFE (grade I (n = 6), grade II (n = 1), grade III (n = 4)) showed no statistical difference (p > 0.05) between grades of sequential SCFE (grade I (n = 9), grade II (n = 1), grade III (n = 1)). In all, 82% of sequential SCFE were mild in severity.
Discussion
Although MRI has not traditionally played a role in the diagnosis and treatment of SCFE, it has been found to demonstrate pathological changes such as focal or diffuse widening of the physis, best delineated on coronal or axial T1-weighted images. 32 Tins et al 30 found bone marrow edema and joint effusion on MRI in all 15 of their study patients diagnosed with SCFE by plain radiograph. Pre-slip displays similar morphology as SCFE, including distortion of the physis on T1 and bone marrow edema in the adjacent metaphysis on T2.22,30,33 Lalaji et al 33 described two cases of proven pre-slip which progressed to SCFE prior to pinning. In both cases, MRI demonstrated distortion of the physis and/or peri-physeal bone marrow edema before the development of radiographically detectable SCFE. Futami et al 22 documented pre-slip in the contralateral hip of four out of ten patients being treated for unilateral SCFE. Umans and colleagues 32 found focal or diffuse widening of the physis (on coronal or axial T1-weighted images) in 100% of SCFE and pre-slip patients. They concluded that there is a continuum of imaging characteristics of SCFE on MRI, with the earliest imaging finding being a focal widening of the physis with or without synovitis. This feature preceded slippage of the femoral head and was only apparent on MRI. They determined that this would be the earliest confirmation in a clinically suspected pre-slip, as no radiographically detectable physeal changes could be found.
We found that there are findings on MRI which warn of pre-slip, including focal and/or diffuse widening of the physis, greater signal intensity of the proximal femoral physis compared with the physis of the greater trochanter and bone marrow edema. The comparison of the T2 signal intensity of the trochanteric physis with that of the proximal femur has not previously been described as a finding to detect pre-slip. We did find that the MRI sequences could be further optimized with the addition of the radial oblique sequence which best evaluated both physes. A sequence that specifically addresses this anatomy with a unique axial oblique angle may help detect very subtle changes consistent with early sequential disease. Furthermore, the best diffusion sequence to simultaneously analyze these two structures would be the coronal as opposed to the axial plane, though this sequence is often low in resolution unless carefully prescribed. Our institution has changed our MRI protocol to reflect these findings (Fig. 1).
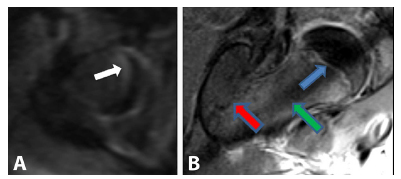
Axial diffusion weighted images. Physis is clearly increased in signal (
Four of the six patients with contralateral SCFE had positive MRI findings (Figs 2 and 3). The sensitivity was high at 80%, specificity 92.9%, positive predictive value 66.7% and negative predictive value 96.3%. MRI was a good predictor for future slip, outperforming the previous methods. Two patients with positive MRI findings, however, showed no evidence of sequential disease at follow-up. These patients may represent mild contralateral disease that did not progress to clinical or plain radiographic deformity and that stabilized without treatment.
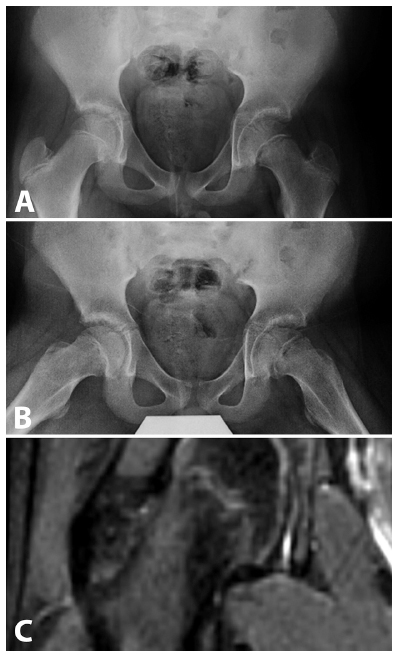
Preoperative anteroposterior/lateral radiographs (
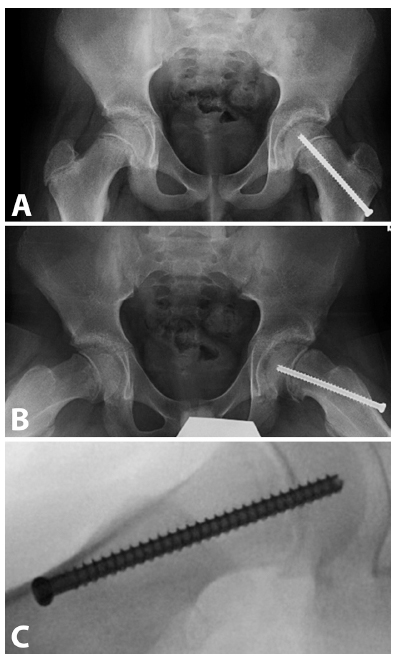
Approximately four months postoperative; patient presents with pain; x-ray changes (
It is well known that delayed diagnosis of SCFE can lead to short- and long-term consequences. Although some surgeons recommend prophylactic in situ fixation of the contralateral hip on initial presentation, only 12% of practising surgeons perform the prophylactic surgery despite supportive research in the high-risk patient. 34 The ability to determine high-risk patients for contralateral slip is lacking. Though there have been various epidemiologic characteristics, scoring systems and radiographic parameters to help guide treatment, none have been universally adopted. Reasons include lack of accepted epidemiologic risk factors, the complexity of the scoring system and contradicting recommendations from the radiographic parameters proposed. The most widely accepted predictor is the chronological age of the SCFE patient at presentation. The correlation between chronologic age and risk of subsequent slip was described by Loder and colleagues. 7 Riad and colleagues 18 advocated that all girls younger than ten years and boys younger than 12 years who present with a unilateral SCFE undergo prophylactic screw fixation. Though it is generally accepted that a strong correlation exists between younger patients and increased risk of a contralateral slip, an exact chronologic age is of limited value due to the great differences in maturation. When this age cutoff was applied to our study; one out of five girls and one out of six boys would have been properly identified (sensitivity 18.2%, specificity 88.4%, PPV 28.6%, NPV 80.9%).
A recent study by Popejoy et al 35 suggested that the mOBS was the best predictor. These investigators followed 260 patients treated for unilateral SCFE, of whom 64 went on to sequential disease. In all, 48 out of 50 patients who had a mOBS between 16 and 18 developed a contralateral slip. We did not find this assessment to be as predictive in our study, predicting only two of the six sequential slips (sensitivity 33.3%, specificity 92.9%, PPV 50%, NPV 86.7%). Furthermore, this scoring system is not widely utilized because of its complexity and wide interpretation variation among orthopaedic surgeons.
In 2015, Nicholson et al 36 suggested that a calcaneal apophysis staging system could be used as an adjunct to the mOBS. They reviewed 279 pelvis radiographs with age matched foot radiographs. 37 They correlated the various stages of calcaneus apophysis ossification with the numerical values of the mOBS. It was suggested that calcaneal apophysis maturation could be used to predict contralateral slips. They created a staging system and concluded that children with calcaneal stages 0 to 2 correlated with mOBS scores of 16 to 18 approximately 94% of the time, making it straightforward to utilize. We did not employ this method as a comparison, as it was not yet published at the time of our study.
Individual radiographic parameters have also been proposed to help predict contralateral slips, such as increased femoral coverage, 38 acetabular retroversion, decreased pelvic incidence 39 and the PSA.34,40 Barrios et al 29 recommended prophylactic pinning in patients with a PSA greater than 12°. Park et al 34 suggested that PSA is more predictive in girls and recommended prophylactic pinning in girls with PSA more than 13°. Although the PSA may be easier to apply in a clinical setting, findings have not been consistent with this method. In our study population, using a PSA more than 12°, only one out of five contralateral slips were predicted (sensitivity 9.09%, specificity 81.4%, PPV 11.1%, NPV 77.8%).
Open triradiate cartilage has been shown to be a reliable risk factor for a contralateral slip. 41 In our study, having an open triradiate cartilage was predictive of contralateral slip, with all patients with contralateral failure demonstrating open triradiates at the initial presentation. However, if an open triradiate cartilage was utilized solely as an indication to prophylactically pin the contralateral extremity, an additional six hips would have been exposed to the risk of surgery without ever progressing to sequential disease. Presence of an open triradiate cartilage combined with MRI findings provided the best predictor of subsequent slip (sensitivity 80%, specificity 100%, PPV 100%, NPV 96.6%).
Limitations of this study include the small number of patients who were enrolled and high number of patients who were excluded. However, patient profiles and slip characteristics were very similar in both groups, lessening the possibility of bias. Another limitation was that patients were not routinely screened with laboratory tests for hypothyroidism or hypogonadism. There is an increased cost to obtain an MRI, but these costs would likely be offset by preventing readmissions and need for future, unanticipated surgery. Reasons for those patients who declined enrollment are difficult to overcome: need for sedation, lack of MRI availability and decreased mobility of those patients with unstable SCFE make it difficult to perform preoperative MRIs on all patients. Strengths of the study include the prospective, blinded design of the study and development of an MRI protocol for the evaluation of pre-slip.
In conclusion, MRI findings consistent with ‘pre-slip’ pathology were present in 67% of patients who went on to a sequential slip. These findings suggest that a sequential SCFE may actually represent bilateral disease upon presentation, and an unidentified pre-slip state in the contralateral hip. The ability of MRI to evaluate a concurrent, contralateral pre-slip with high sensitivity and specificity prior to treatment of a unilateral slip would prevent unnecessary prophylactic pinning and indicate surgery for those hips destined to fail. MRI is a valuable adjunct to help guide treatment of contralateral hips in patients presenting with unilateral SCFE and when combined with an open triradiate cartilage, outperforms previously described predictive methods. We recommend a preoperative MRI of the contralateral hip for patients presenting with unilateral, stable SCFE.