
Abstract
Purpose:
To identify a specific factor that can support the decision for prophylactic fixation in unilateral slipped capital femoral epiphysis.
Methods:
This retrospective cohort study included a total national population of 379 children diagnosed with slipped capital femoral epiphysis from 2007 to 2013. Regression analysis used information on slip severity, clinical classification of the index hip, age, sex, age-adjusted body mass index, the difference in epiphyseal–diaphyseal angle, and comorbidity to identify any risk factor for the subsequent development of a slip in the contralateral hip. Four observers evaluated the triradiate cartilage following the modified Oxford bone score grade. The occurrence of later development of a contralateral slip in different stage of physeal closure was used to analyze the sensitivity and specificity for this method.
Results:
This study’s only predictor for a subsequent contralateral slip was chronological age. At age 13 years or older, 1/15 in girls and 3/65 in boys suffered from a slip in the contralateral hip. Thus, when using age <13 years as a test for deciding when to do prophylactic fixation, the sensitivity would be 88% and specificity 51% for preventing contralateral slip. However, the correlation between the four different observers was too low to be considered useful when assessing the triradiate cartilage for skeletal maturity.
Conclusion:
We would advocate a prophylactic fixation for children <13 years diagnosed with a unilateral slipped capital femoral epiphysis as an easy-to-use algorithm.
Level of evidence:
level II.
Introduction
Slipped capital femoral epiphysis (SCFE) is often unilateral at presentation. Furthermore, there is also a subsequent contralateral slip in many affected children. 1 The incidence of subsequent involvement in the contralateral hip has been reported to be as high as 60%. 2 Whether prophylactic fixation of the contralateral hip in unilateral SCFE should be performed is controversial.3–5 Prophylactic fixation aims to avoid a possible subsequent slip in the contralateral hip. The arguments against prophylactic fixation underscore the risks for potential complications in the non-affected hip, for example, a peri-implant femur fracture, chondrolysis, deep infection, or focal avascular necrosis (AVN).6,7 There have been attempts to evaluate whether predictive factors yield a higher risk of a subsequent contralateral slip.8,9 Proponents argue that a prophylactic fixation of the contralateral hip can always be justified in the presence of an underlying renal disorder, endocrinopathy, metabolic disease, or a very young child.3,4
This study aimed to identify a subgroup of children with a unilateral SCFE where prophylactic fixation is justifiable, based on age-related and classification criteria. We hypothesized that specific factors predict when prophylactic fixation of the contralateral hip could be recommended for children with a unilateral SCFE. We also hypothesized that the triradiate cartilage classification by the modified Oxford bone score10,11 could serve as a factor to aid in the decision of whether prophylactic fixation should be recommended or not.
Methods
Based on the Swedish Paediatric Orthopaedic Quality Register (www.spoq.se), children diagnosed with SCFE in the index hip between 1 January 2007 and 31 December 2013 were identified. Inclusion criteria were children living in Sweden, registered in the Swedish Population Register, and with a Swedish personal identity number diagnosed with SCFE in their index hip (first hip affected by SCFE) during the study period. Exclusion criteria were SCFE due to high energy trauma or septic coxitis. Only complications requiring subsequent surgery or possible to verify through the assessment of a radiograph or from the medical records at the final follow-up has been registered in this study. The SPOQ database was compared with individual-based data from the Swedish National Board of Health and Welfare (National Patient Register) for completeness’s control purpose. A scientific database was then created with a total national population for the study period, including data from medical records and radiographs with a 3-year follow-up. 1 However, the six children, with age below 9 years when they were diagnosed with SCFE in their index hip, were followed until the closure of the proximal femoral physis. This scientific database was used for this study. The study population is described in Figure 1.
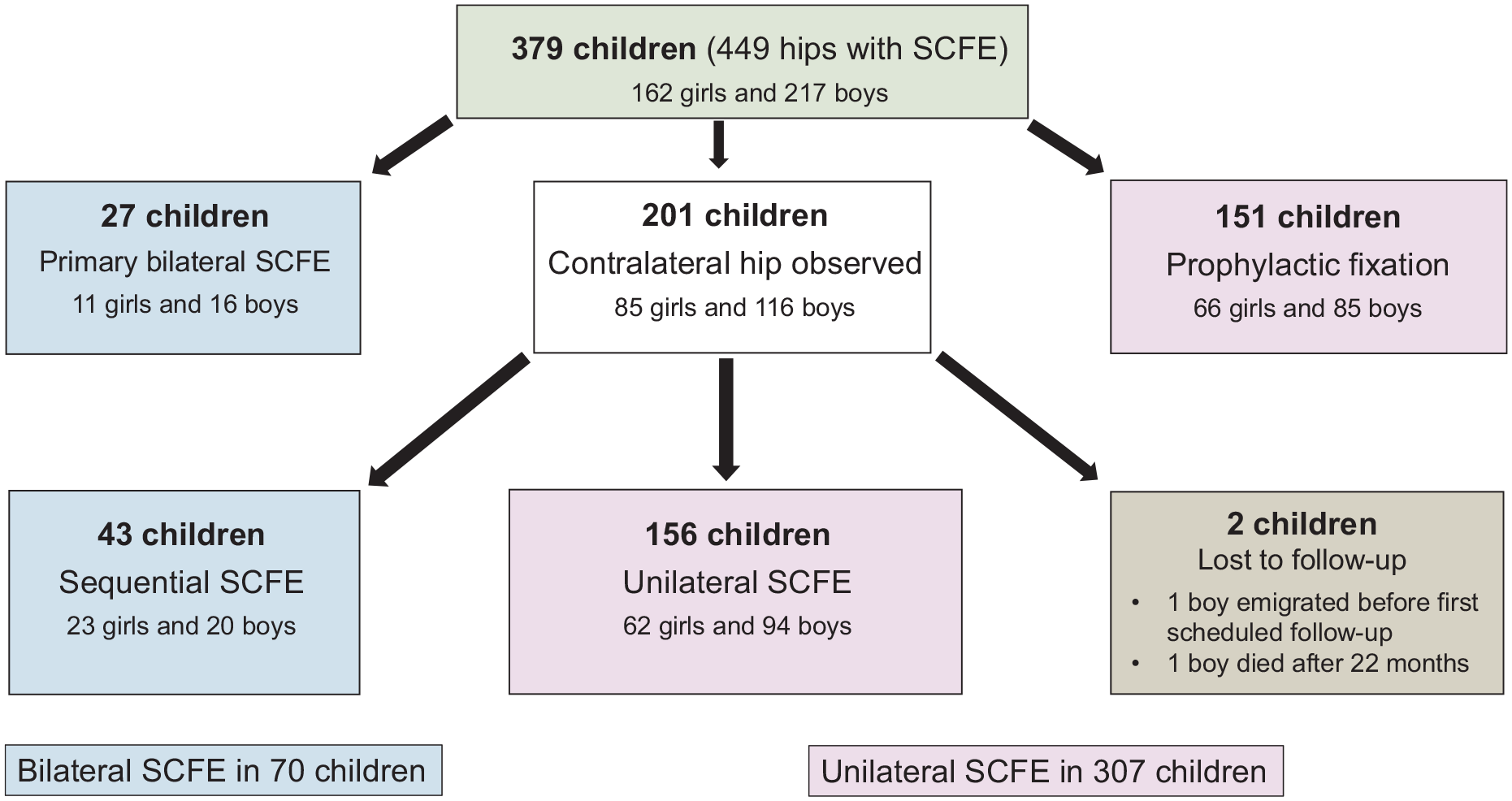
Study population.
Information about the severity of the slip,12–15 clinical classification of stability as described by Loder, 13 sex, age when the index hip was diagnosed with SCFE, and comorbidity are presented in Table 1. However, information about the age-adjusted body mass index (BMI) 16 was only available for 81% of the participants. Therefore, these factors were used in a regression analysis to identify any risk factor for the subsequent development of a slip in the contralateral hip.
Group characteristics of the group with prophylactic fixation versus the study group.
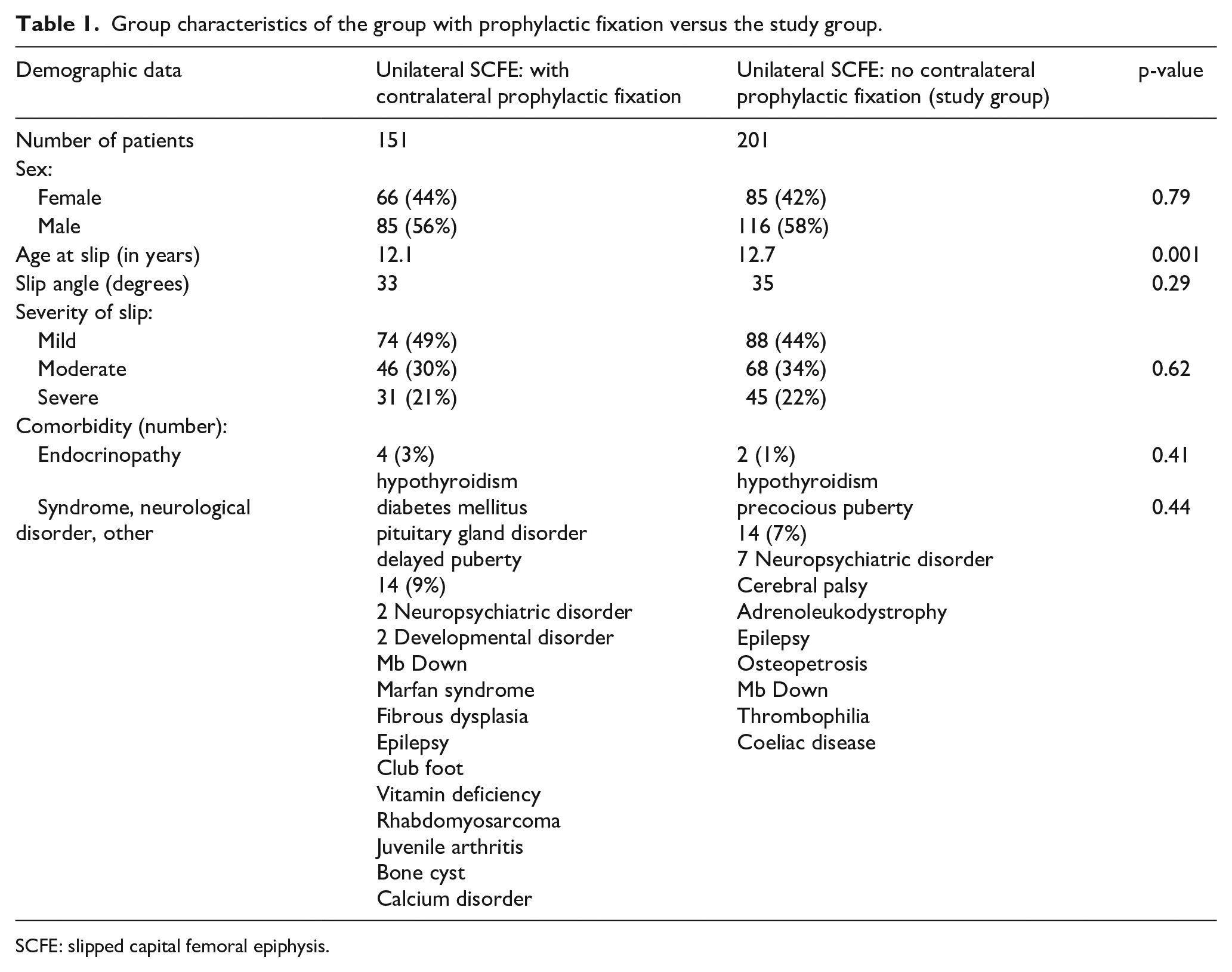
SCFE: slipped capital femoral epiphysis.
The slip severity was measured using either the calcar femorale technique 14 on a Lauenstein view or the Billing technique 15 on a Billing lateral view. Slip severity was graded as mild (13° to 29°), moderate (30° to 50°), or severe (>50°). 12 The difference in epiphyseal–diaphyseal angle was measured by an experienced observer on all 130 preoperative Lauenstein view radiographs; 30 of these patients developed a subsequent slip in the contralateral hip. In 71 patients, Lauenstein lateral views were not available to measure the epiphyseal–diaphyseal angle. For 13 of these 71 patients, a subsequent slip was later diagnosed.
It was impossible to utilize the complete modified Oxford bone score for the assessment since, for most children, the preoperative radiographs did not include the iliac crest. Instead, preoperative radiographs were used to evaluate the triradiate cartilage according to the modified Oxford bone score grade 1–3: grade 1—wide open, grade 2—partial physeal closure, or grade 3—closure of the triradiate cartilage.10,11
Four observers independently assessed the maturity grade of the triradiate cartilage of the acetabulum. Two of the observers were specialists in orthopedic surgery, and two were orthopedic residents.
All four observers received written instructions for the triradiate cartilage assessment, including examples of typical grades with plain radiographs and simplified drawings.10,11 The observers used their standard picture archiving and communication system. A training period was included where radiographs with dubious quality for the assessment could be discussed. Independent of the side affected by SCFE, the maturity was assessed using the side that best visualized the triradiate cartilage. The primary outcome, that is, the occurrence of a subsequent contralateral slip, was used to analyze this method’s sensitivity (the ability of the test to correctly identify patients with the disease) and specificity (the ability of the test to correctly identify individuals without the disease). All radiographs for the 201 children (see Figure 1), with a unilateral SCFE where no prophylactic fixation was performed, were randomly presented in a list independently to all observers without a chronological or age-dependent rank.
Statistics
T-test, chi-square test, and Fisher’s exact test compared the study group with those already treated with prophylactic fixation. Chi-square test, Fisher’s exact test, and linear regression analysis were performed when analyzing factors that could predict a secondary slip. In addition, a multivariate regression analysis was done, including variables with p-value < 0.1 using IBM SPSS Statistics for Windows (version 24; IBM Corp, Armonk, NY, USA). The significance threshold was set at 0.05 with a two-tailed p-value.
Results
The characteristics of the study group and the group that already received prophylactic fixation are presented in Table 1.
For the 201 children with primary unilateral SCFE scheduled for clinical and radiological follow-up, the median age was 13.4 (3.9–16.8) years for boys and 12.1 (8.4–14.7) years for girls. In the group of 43 children (20 boys and 23 girls) who developed a subsequent SCFE in the contralateral hip, the median age for boys was 12.3 (9.5–15.1) years and for girls 11.4 (9.4–14.7) years. The median age for a subsequent contralateral slip was 13.2 (10.7–15.8) years for boys and 12.3 (9.8–14.8) years for girls. Overweight or obesity, according to age-adjusted BMI, was present in 85 children of 125 (68%) in the group with prophylactic fixation (missing values: n = 26). In children with clinical and radiological follow-up, the corresponding value was 109 of 161, that is, 68% (missing values: n = 40).
For the whole group of 201 children who had clinical and radiological follow up, the median age was 12.7 (3.9–16.8) years. The 151 children who had a prophylactic fixation of the contralateral hip had a median age of 12.1 (7.2–17.7) years. This age difference was significant between the two groups. For most of the 151 children, the surgeon’s operation report specified the main indication for a prophylactic procedure. Examples from the operation report were a very young age, long symptom duration for the index hip, an unstable SCFE in the index hip, a severe slip in the index hip, assessment of the family compliance capacity for a follow-up without prophylactic surgery, obesity, or a departmental routine in the hospital concerned for the treatment of children with a unilateral SCFE.
In the group of 43 children with a delayed involvement of the contralateral hip in unilateral SCFE, the slip angle of the second hip was distributed as follows: 31 mild, 11 intermediate, and 1 severe. The clinical classification showed only one child with an unstable SCFE in the second hip in this group. One early postoperative complication was registered for the contralateral hip in this group. The fixation implant was located outside the epiphysis on the postoperative radiographs, and a re-operation had to be performed.
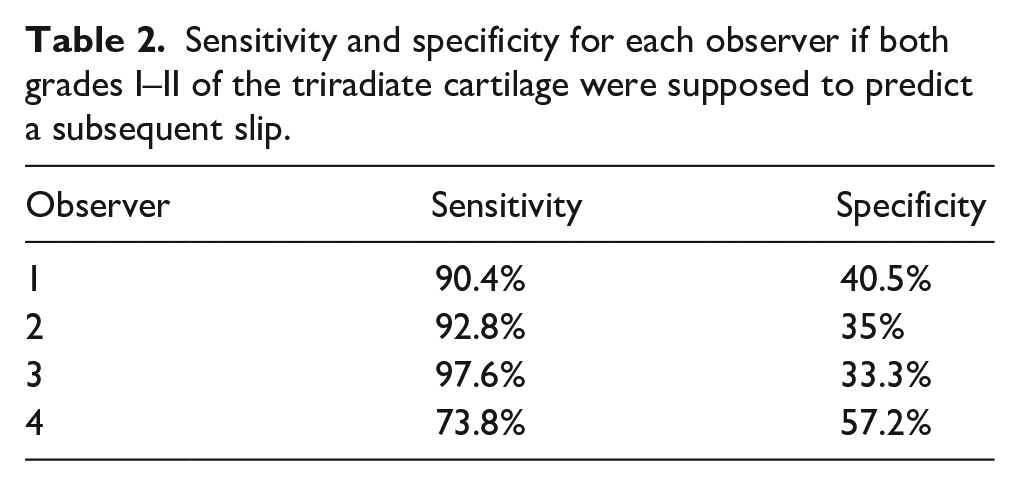
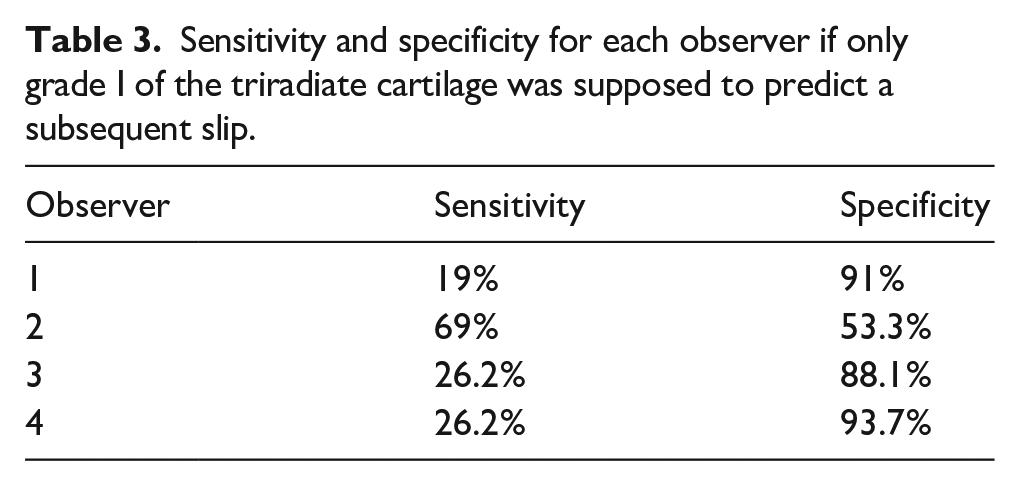
The assessment results of the triradiate cartilage with sensitivity and specificity for each observer, if used as a tool for deciding when to do prophylactic fixation, are presented in Tables 2 and 3. If both grades I and II of the triradiate cartilage (wide open or partial physeal closure of the triradiate cartilage) were used as a predictor for subsequent slip, the sensitivity among observers ranged from 73.8% to 97.6%, and specificity ranged from 33.3% to 57.2%. When only grade I (wide open) of the triradiate cartilage was used, the sensitivity ranged from 19% to 69%, and specificity ranged from 53.3% to 93.7%.
Sensitivity and specificity for each observer if both grades I–II of the triradiate cartilage were supposed to predict a subsequent slip.
Sensitivity and specificity for each observer if only grade I of the triradiate cartilage was supposed to predict a subsequent slip.
Univariate analysis was performed, including the following parameters: slip severity, clinical classification (stable/unstable), age-adjusted BMI, age, sex, the difference in epiphyseal–diaphyseal angle, and comorbidity. The results are shown in Table 4.
Univariate analysis of factors that might predict a subsequent slip for the 201 children with a unilateral SCFE and no prophylactic fixation. The group of 43 children with a subsequent slip is compared with the group of 156 children with no subsequent slip.
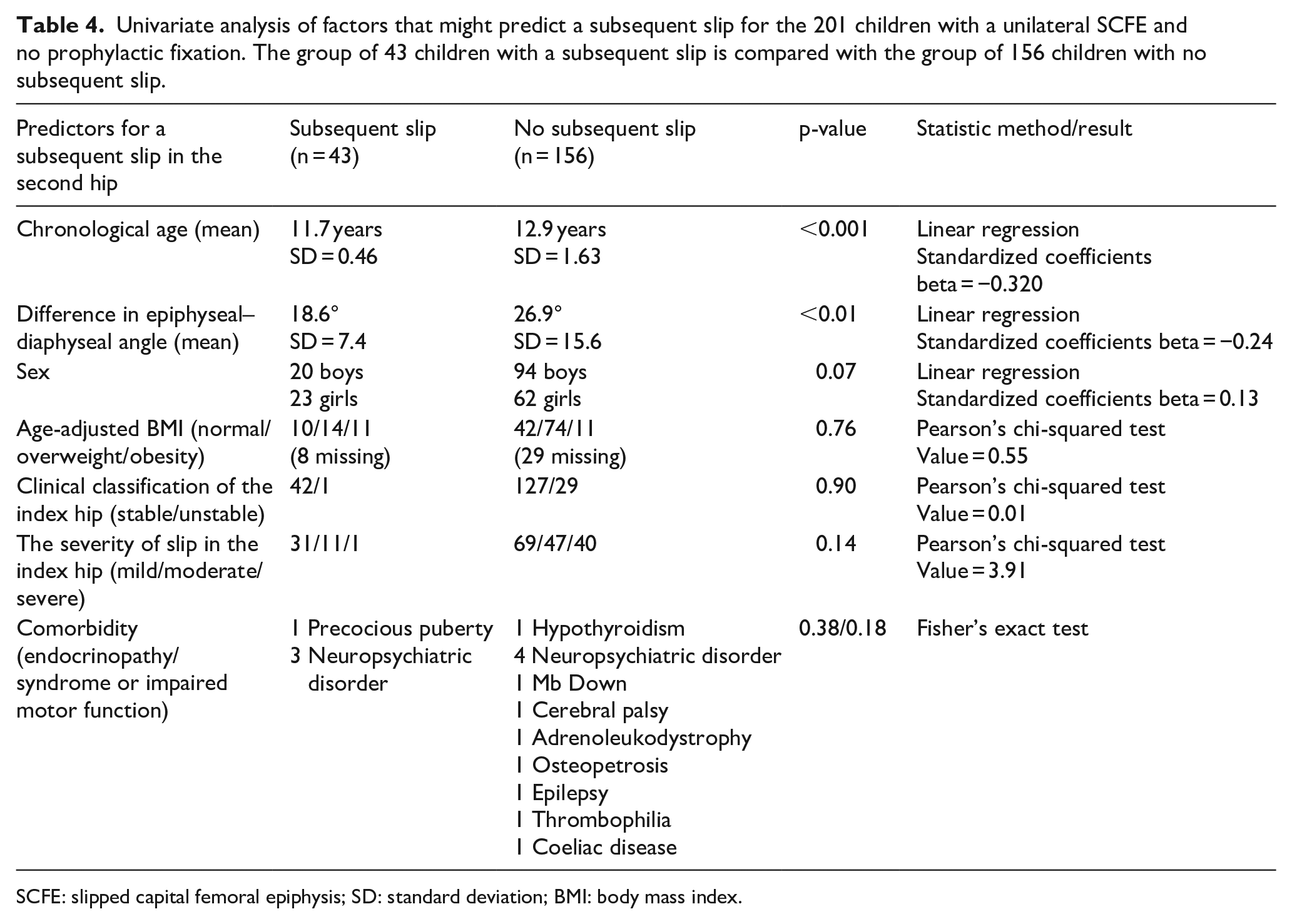
SCFE: slipped capital femoral epiphysis; SD: standard deviation; BMI: body mass index.
The following multivariate regression analysis included age, the difference in epiphyseal–diaphyseal angle, and sex (Table 5). However, only lower chronological age was associated with a risk of developing a subsequent slip in the contralateral hip. This relationship was statistically significant with a standardized coefficients beta −0.32 with p < 0.001.
Results of the multivariate analysis.

The proportion of children with a subsequent contralateral slip divided into different age categories is presented in Figure 2. For boys 13 years or older at primary diagnosis of SCFE in the index hip, 3 of 65 had a subsequent contralateral slip. The corresponding proportion for girls 13 years or older was 1 of 15. However, following a careful re-evaluation of the radiographs of the contralateral hip, we found that one girl who was diagnosed with a unilateral slip and primarily treated accordingly, in a retrospective analysis, was found to have a mild slip on her contralateral hip radiograph already at the initial presentation with her index hip. For children ≥12 years but <13 years, 5 of 30 girls developed a subsequent SCFE in the second hip, whereas the boys’ proportion was 7 of 28. Sensitivity and specificity when using age as the only predictor for subsequent contralateral slipping vary according to Figure 3. When using <13 years as a cut-off for prophylactic fixation, the sensitivity would be 88% and specificity 51%.
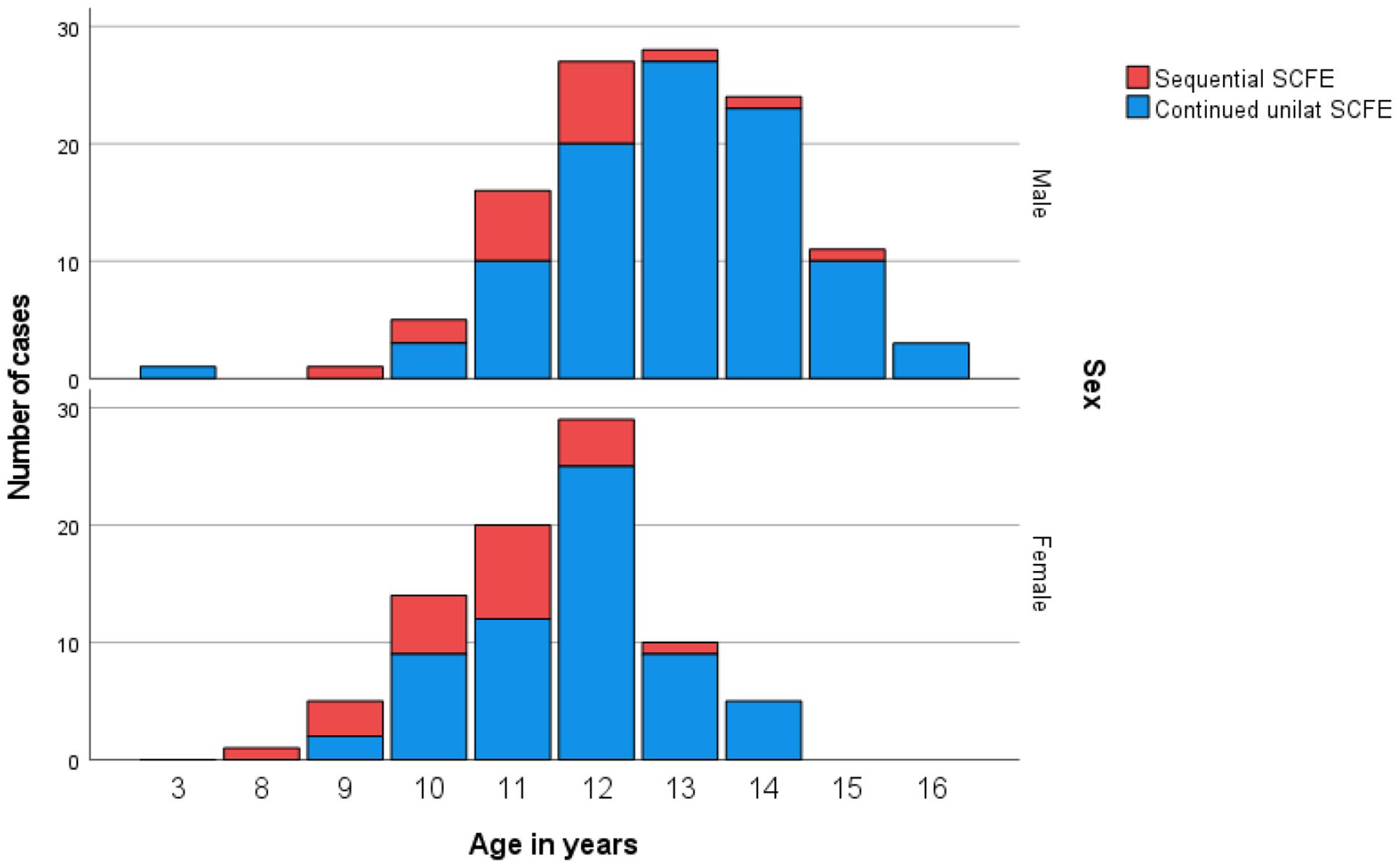
The proportion of girls and boys, respectively, with a subsequent slip in the second hip presented in different age categories.
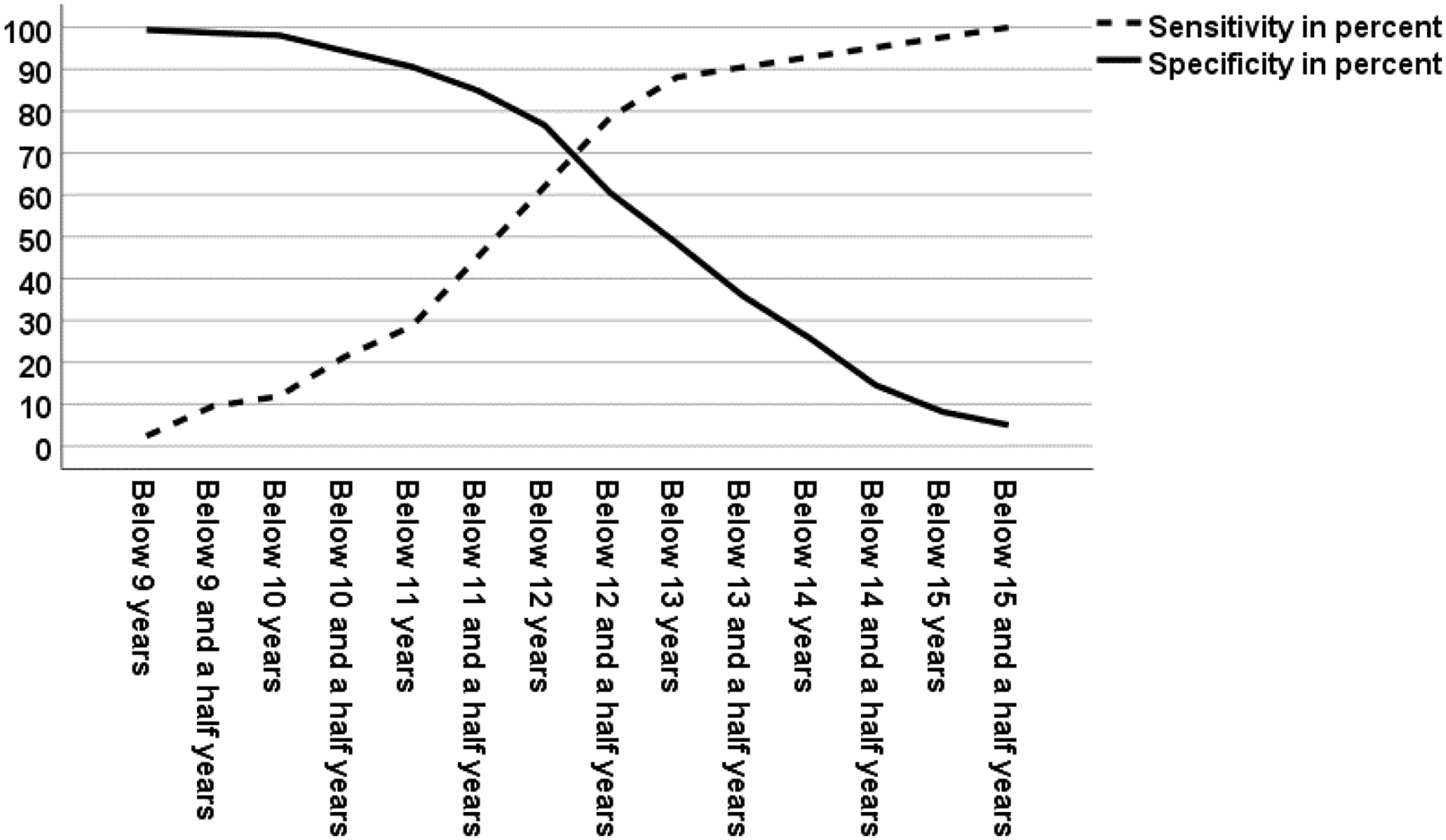
Sensitivity and specificity when predicting contralateral slip using different age categories.
Discussion
At age 13 years or older, only a tiny proportion of the children in this study had a subsequent slip in the contralateral hip after clinical follow-up, 1/15 in girls and 3/65 in boys. This finding implicates that for a child presenting with a primary unilateral SCFE at age 13 years or older, a subsequent contralateral slip risk is 5%.
The proportion of a subsequent slip in different age categories does not substantially differ between girls and boys in this study. One explanation might be that a high proportion of the boys are overweight or obese and probably have an earlier onset of puberty.17,18 Furthermore, very few children in this study were diagnosed with comorbidity at the surgery for the index hip. 1
In our study population, two peri-implant femur fractures occurred within 1 month after surgery. One child developed a deep infection secondary to surgery for the peri-implant femur fracture. Another child developed a subsequent SCFE in the contralateral hip despite a prophylactic fixation. No AVN or chondrolysis was found during the 36-month follow-up. 19 In addition, there was one early re-operation performed in the group of 43 children with a subsequent slip in the contralateral hip. The fixation implant was located outside the epiphysis on the postoperative radiographs in this particular child.
There are differing opinions expressed in the literature regarding prophylactic fixation for the contralateral hip in unilateral SCFE. Aversano et al. 20 suggest that strong consideration should be given to prophylactic stabilization of the contralateral hip in patients with SCFE presenting with a BMI-for-age ≥95% percentile. Nasreddine et al. 21 argue that prophylactic pinning might be considered for morbidly obese patients.
The potential for surgical complications and the risk for subsequent surgery due to a peri-implant femur fracture or the development of AVN or a deep infection are debated. Current recommendations for prophylactic fixation include known risk factors, for example, metabolic disorders, endocrinopathy, or expected difficulties in family compliance during follow-up. At the diagnosis of unilateral SCFE, young age, either chronological or skeletal age, has also been presented as a predictor for a subsequent slip in the contralateral hip.3–7,9–11,22
Others have focused on the assessment of the radiographs of the contralateral hip. Measurement of the epiphysis’ posterior tilt and superior extension of the epiphysis might affect the risk of a contralateral slip. 8 Younger age and minor differences in the epiphyseal–diaphyseal angle between both hips were predictors of contralateral slip in a recent study. 23 Our results show that age is an essential factor to consider when deciding upon a prophylactic fixation to be offered to a child with unilateral SCFE. However, our results do not support using the epiphyseal–diaphyseal angle in a decision algorithm for prophylactic fixation. The epiphyseal-shaft angle measurement on a frog-leg lateral view (Lauenstein) was initially described by Southwick 24 in 1967 as a measurement to correct the deformity in SCFE to prevent arthritic degeneration. The measurement achieved for one hip had to be adjusted according to the measurement found on the contralateral hip that was considered not affected. The normal interval described was relatively wide, with 0–25 degrees considered normal values. The epiphyseal-shaft difference measurement method was not intended to diagnose SCFE in the contralateral hip. However, we have found it advantageous to assess each hip individually, including measurements of the slip angle together with other radiographic signs, clinical findings, and the patient history to evaluate whether there is a simultaneous contralateral SCFE disorder or not. Therefore, using an epiphyseal-shaft angle difference of <21 degrees would for many patients with a mild SCFE in the index hip, with a short duration period with symptoms, tend to overestimate the risk for a contralateral slip or diagnose too many children with a contralateral SCFE despite other radiographic evidence of the disease.
Abnormal magnetic resonance imaging (MRI) findings combined with open triradiate cartilage could be a strong predictor of subsequent slip with a sensitivity of 100% and specificity of 80%. 25 Triradiate cartilage assessment for skeletal maturity as a predictor for a subsequent slip in the second hip has been advocated.11,23,25,26 However, Danino et al. 27 showed that triradiate status and Risser’s grade did not influence their final multivariate analysis strength, but so did epiphyseal extension ratio, posterior epiphyseal angle and posterior sloping angle. When evaluating radiographs, the experience and the variation between clinicians must be considered. Our study’s correlation between the four different observers with different experience levels was too low using the modified Oxford bone score. However, chronological age is an easy variable to analyze.
A number needed to treat (NNT) analysis has been presented in previous publications to justify prophylactic fixation of the contralateral hip in children with a unilateral SCFE. 28 However, due to the above-shown selection bias with the group of 151 children treated with a prophylactic fixation in our study, we believe that a calculation of the absolute risk reduction, relative risk reduction, or NNT would not add any important information.
When a clinician meets a patient with a unilateral SCFE, several factors must be considered before deciding whether to do prophylactic fixation. Advantages and disadvantages with follow-up versus prophylactic fixation also depend on the complication rate in the actual population and the family’s compliance. In our population, chronological age under 13 years will, in most cases, be an easy-to-use predictor to support prophylactic fixation. When the decision is made not to do prophylactic fixation, we recommend radiological and clinical follow-up every fourth month and conceivable information to the family about when and how to contact the responsible doctor.
If the complication rate is low and the resources to follow-up are limited, age below 14 years can be used as a cut-off (prophylactic overtreatment). If the complication rate is higher and there are enough resources to follow up, age below 12 years can be used as a cut-off. An apparent difference between chronological age and biological age must be considered when deciding about prophylactic treatment.
Conclusion
Based on all available data from our study population and populations with comparable demographic conditions, we would advocate a prophylactic fixation for children <13 years diagnosed with a unilateral SCFE as an easy-to-use algorithm.
Strengths and limitations
This was a retrospective study of a total national population of 379 children treated for SCFE; thus, the coverage ratio was high. One hundred fifty-one patients already received prophylactic fixation at the time of primary surgery. Therefore, they were excluded from the analysis. In addition, the time to follow-up was limited to 36 months. Therefore, possible complications after this period have not been included in the analysis. However, other studies have shown that the vast majority will develop a subsequent slip within 28 months.1,8,9,11,27,28 This study did not present the natural history for the contralateral hip in children with a unilateral SCFE. Children were already selected from the initial study population, where a prophylactic fixation of the contralateral hip was performed. A chronologic age of 13 years is not necessarily equal to the biological age of 13 years. This study did not evaluate the biological age using a radiograph of the hand.
Footnotes
Acknowledgements
The authors acknowledge Lovisa André, MD, Department of Orthopaedics, Jönköping, Region Jönköping County, Sweden, for radiographic measurements; Bo Rolander, PhD, statistician at the Futurum—Academy for Health and Care, Jönköping County, Sweden; and Futurum—Academy for Health and Care, Region Jönköping County, Sweden.
Author contributions
M.L. and B.H. contributed to the study design. M.L., M.S., and B.H. contributed to the data collection. M.L., M.S., M.Sr., P.M., and B.H. contributed to the data analysis. M.L., M.S., M.Sr., P.M., and B.H. contributed to the manuscript preparation.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval was obtained from the Regional Ethical Review Board in Lund, with registration numbers 2013/87 and 2015/320. The study was in accordance with the 1964 Declaration of Helsinki’s ethical principles for medical research involving humans and its later amendments.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Futurum—the Academy for Healthcare, Region Jönköping County, grant no. FUTURUM-964258 and the Medical Research Council of Southeast Sweden, grant number FORSS-906641.
Informed consent
Informed consent was obtained from all individual participants included in the study and one parent or guardian of each child.