
Abstract
Abstract
Purpose
The purpose of this study was to identify risk factors for developing a subsequent contralateral slipped capital femoral epiphysis (SCFE) and provide a prediction score to quantify risk of subsequent slip at the time of initial presentation.
Methods
This retrospective study included patients that presented with a unilateral SCFE between 2006 and 2017. Chart and radiographic review were performed to collect demographic, clinical and radiographic risk factors. Descriptive statistics, univariate analyses and multivariate regression analysis were used to compare risk factors between patients that did or did not develop a subsequent contralateral SCFE.
Results
This study included 183 patients and 33 patients (18%) developed a subsequent contralateral SCFE. Younger age at time of initial presentation, lower modified Oxford Score and smaller difference in epiphyseal-diaphyseal angle between both sides during index presentation were significant predictors of subsequent contralateral SCFE. Specifically, age ≤ 11 years, modified Oxford Score ≤ 20 and difference in epiphyseal-diaphyseal angle of ≤ 21° between both hips were predictive of a contralateral slip (Area Under the Curve = 0.78; p < 0.05). The presence of each risk factor increased the risk of subsequent contralateral SCFE and having all three risk factors increased the risk to 73%.
Conclusion
There is a significant risk of subsequent contralateral SCFE in patients with unilateral SCFE, and predictive risk factors include younger age, lower modified Oxford Score and smaller difference in epiphyseal-diaphyseal angle between the affected and unaffected hips.
Level of Evidence
Level III
Keywords
Introduction
Slipped capital femoral epiphysis (SCFE) is a relatively common condition that affects children and adolescents. The incidence of SCFE varies greatly and it has been reported to range from 0.22 per 100 000 children to 24.58 per 100 000 children. 1 This variability in incidence is likely related to differences in study populations.2–4 There have been several risk factors associated with the development of SCFE;2,5,6 however, the aetiology of SCFE remains unclear. SCFE poses a considerable burden on affected patients and long-term complications include osteonecrosis, chondrolysis and degenerative arthritis.7–10
Patients may initially present with either unilateral SCFE or bilateral SCFE. However, a common scenario seen in clinical practice is the development of subsequent contralateral slip after unilateral SCFE. Some authors have reported that 40% of patients may develop a contralateral slip in the first 18 months but other studies have reported a wider range from 11% to 60%.11–17 Moreover, the risk of subsequent contralateral SCFE is 2335 times greater than the risk of presenting initially with a unilateral SCFE.15,18 Several factors have been reported to be associated with an increased risk of developing contralateral SCFE including age, metabolic disorders, skeletal maturity, as well as numerous radiographic measures such a as posterior sloping angle, alpha angle, epiphyseal tilt angle and epiphyseal extension ratio.19–22 In a previous systematic review and meta-analysis, younger age and a higher posterior sloping angle were significant risk factors for the development of subsequent contralateral SCFE. 23 Some authors have commented that SCFE is a bilateral disease, and it is plausible that similar clinical and radiographic risk factors place both hips at risk of a slip.
Prophylactic pinning of the contralateral hip is often considered in patients presenting with unilateral SCFE, and this decision is typically based on qualitative factors. Prophylactic pinning has several associated risks and complications, and accurate patient selection is critical. 24 Previous decision analyses on this topic have arrived at contradictory conclusions, and there is a paucity of literature to guide clinical decision making.18,25 The purpose of this study was to assess the rate of contralateral slip in our patient population, study and identify risk factors associated with subsequent contralateral slip, and ultimately, provide a prediction score to quantify the risk of subsequent contralateral SCFE.
Patients and methods
After obtaining institutional review board approval, we performed a retrospective cohort study. The first phase of this study included a retrospective chart review of all paediatric patients that were treated at our institution for a unilateral SCFE between 2006 and 2017. We included male patients < 16 years of age and female patients < 14 years of age. We excluded patients that were treated for bilateral SCFE at the time of index presentation, underwent prophylactic pinning at time of index procedure or did not have adequate radiographs for review (Fig. 1). The most common reasons for prophylactic pinning were young age, skeletal immaturity signified by an open triradiate cartilage or presence of an endocrine disorder. We also excluded patients that presented with an index SCFE after 2017 in order to ensure a minimum two-year follow-up for all patients. Follow-up protocol was as per the surgeon's discretion but all included patients had clinical and radiographic follow-up for a minimum of two years. Data collected from chart review included age, sex, weight, height, body mass index and ethnicity. Clinical data regarding comorbidities, presence of endocrine abnormality, duration of symptoms, laterality, slip stability, slip chronicity, type of fixation, perioperative complications and time to subsequent slip was also collected from chart review.
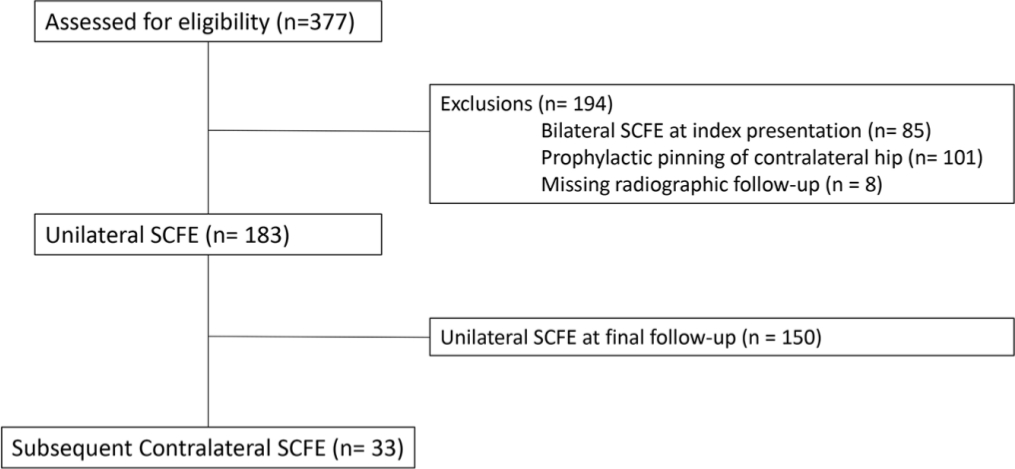
Consolidated Standards Of Reporting Trials diagram of included patients.
Radiographic measurements of interest included epiphyseal-diaphyseal angle of each hip, difference in epiphyseal-diaphyseal angle (Southwick angle), alpha angle, physeal sloping angle, posterior sloping angle, frontal tilt angle, lateral tilt angle, superior epiphyseal extension ratio (SEER) and modified Oxford Score (see Supplementary Material). All measurements were performed on anteroposterior (AP) and frog-lateral radiographs of the affected and unaffected hips obtained at the time of initial presentation. All measurements were performed by a single observer (RS), who was blinded to the presence or absence of subsequent contralateral SCFE. The epiphyseal-diaphyseal angle was measured on the frog-lateral radiograph and it was measured on the affected and unaffected hips. 26 Epiphyseal-diaphyseal angle measurements were reported as the absolute epiphyseal-diaphyseal angle of the affected hip and the difference in epiphyseal-diaphyseal angles between the affected and unaffected hips as reported by Southwick. 27 All other measurements were performed on the unaffected hip. Specifically, the alpha angle, posterior sloping angle and lateral tilt angle measurements were performed on the frog-lateral view, and the physeal sloping angle, frontal tilt angle and SEER were assessed on the AP view.26,28–30 Lastly, the modified Oxford Score was determined for each patient on the AP pelvis radiograph20,31 (Fig. 2).
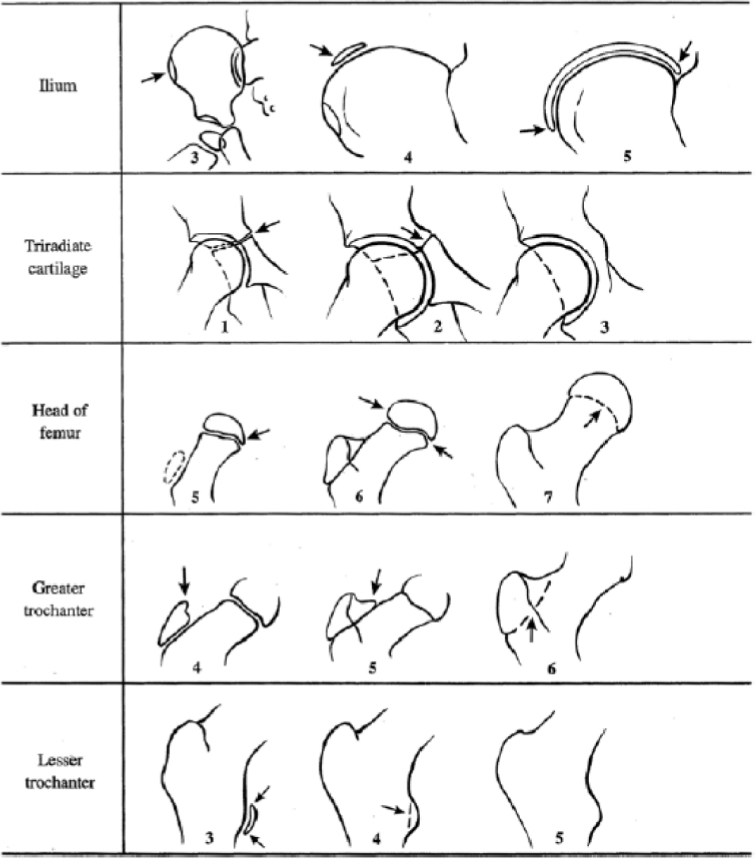
Modified Oxford Score. Source: Popejoy D, Emara K, Birch J. Prediction of contralateral slipped capital femoral epiphysis using the modified Oxford bone age score. J Pediatr Orthop 2012;32: 292, Figure 2.
Statistical analysis
Descriptive statistics were performed to obtain frequencies and measures of central tendency. All categorical data was analyzed using Pearson chi-squared test or Fisher's Exact test for statistical significance. Continuous variables were analyzed using t-test, Mann-Whitney U test, or analysis of variance. Correlations were made using Pearson's or Spearman's test. Multivariate analysis was performed using binary logistic regression using backwards likelihood ratio methodology, with criteria on univariate for entry into the model of 0.10 of significance. Simpler models were developed using cutoff points developed from receiver operator curves (ROCs) and analyzed using logistic regression. Negative 2 log likelihood methodology was used to compare models. We then converted these risk factors to simply present or absent in order to compare risk based on number of risk factors present. All statistics were calculated using SPSS Version 25 (IBM Corp, Armonk, New York).
Results
All patients
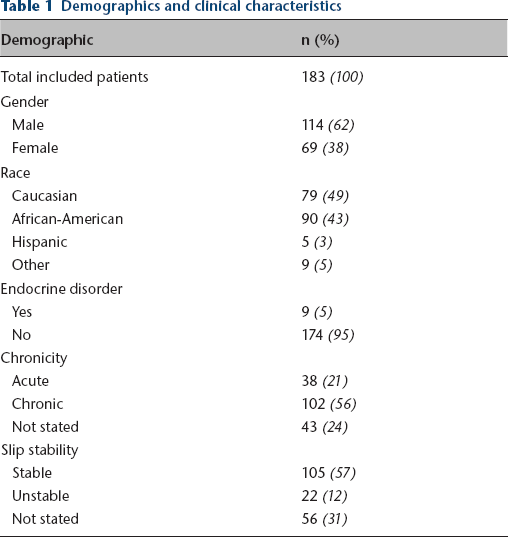
This study included 183 patients who presented with an index unilateral SCFE (Table 1). In this cohort, 114 were male patients (62%), and the majority of patients were African-American (49%, 90 patients) or Caucasian (43%, 79 patients). In total, nine patients had a documented endocrine disorder (5%). Almost all patients presented with pain as their primary complaint (85%, 155 patients). Approximately half of all patients had chronic SCFE, defined as symptoms lasting over three weeks (56%, 102 patients) and a stable SCFE was noted in 105 patients (57%). Data regarding chronicity of symptoms and slip stability was unavailable for 24% and 31% of patients, respectively.
Demographics and clinical characteristics
Subsequent contralateral SCFE
In total, 33 patients developed a subsequent contralateral SCFE (18%). The most common symptom at subsequent presentation was pain (88%, 29 patients). In this group, 14 patients presented with chronic contralateral SCFE (42%), and the majority of patients presented with a stable contralateral slip (64%, 21 patients).
Univariate analysis
Based on univariate analysis, there were significant differences in several variables between patients that did and did not develop a subsequent contralateral SCFE (Table 2). Specifically, the group that developed a contralateral SCFE were younger (11.5 years old versus 12.7 years old), had a higher proportion of female patients (55% versus 34%), lower modified Oxford Scores (19.8 versus 21.2), higher incidence of an open triradiate cartilage (52% versus 26%), lower absolute epiphyseal-diaphyseal angle (36.4° versus 45.2°), smaller difference in epiphyseal-diaphyseal angles during index presentation (18.6° versus 29.6°), lower frontal tilt angle (9.3° versus 11°) and smaller SEER (0.7 versus 0.72) (p < 0.05). There were no differences in other demographic, clinical or radiographic factors (p > 0.05).
Clinical and radiographic differences between groups
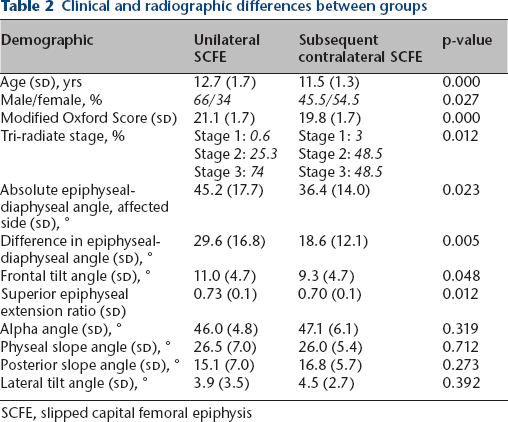
SCFE, slipped capital femoral epiphysis
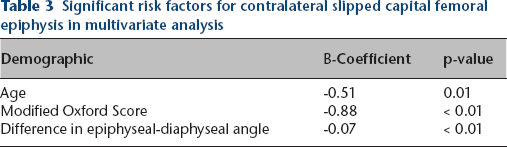
In the multivariate regression model, younger age (β = -0.51; p = 0.01), lower modified Oxford Score (β = -0.88; p < 0.01) and smaller difference in epiphyseal-diaphyseal angle between both sides during index presentation (β = -0.07; p < 0.01) remained significant (Table 3). The other risk factors that were significant in the univariate analysis did not reach significance (p > 0.05).
Significant risk factors for contralateral slipped capital femoral epiphysis in multivariate analysis
Prediction score
Age, modified Oxford Score and difference in epiphyseal-diaphyseal angle were investigated between patients that did and did not develop a subsequent contralateral SCFE. ROCs were used to determine optimal thresholds for these factors with good predictive ability (Area Under the Curve, AUC = 0.78; p < 0.01, Fig. 3). Specifically, risk factors for subsequent contralateral SCFE included age ≤ 11 years, modified Oxford Score ≤ 20 and difference in epiphyseal-diaphyseal angle ≤ 21°. The baseline risk of subsequent contralateral SCFE was noted to be 2.6%, and the presence of each risk factor increased the risk of subsequent contralateral SCFE (Table 4). If all three risk factors were present, the risk of subsequent contralateral SCFE was noted to be 73%. Furthermore, the number needed to treat or prophylactically pin to prevent a subsequent contralateral SCFE in patients with all three risk factors was calculated to be 1.4 patients.
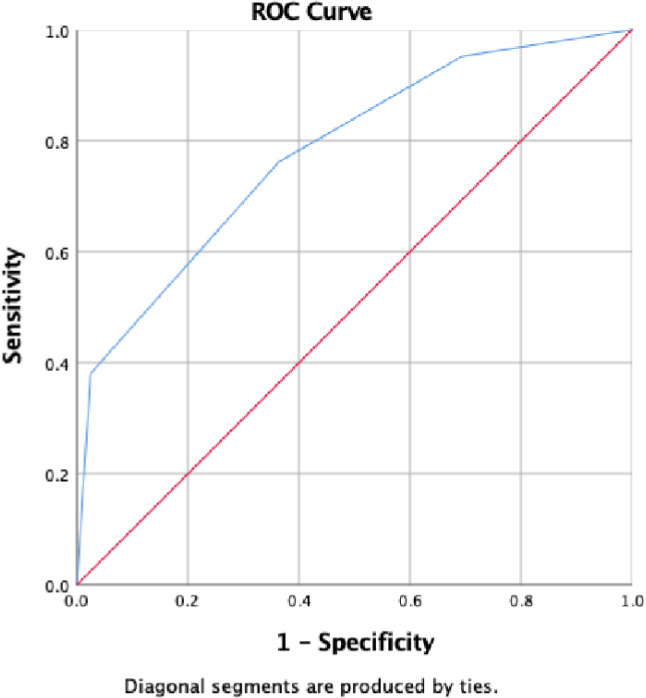
Receiver operating characteristic (ROC) curve for prediction score.
Prediction score and risk of developing subsequent contralateral slipped capital femoral epiphysis
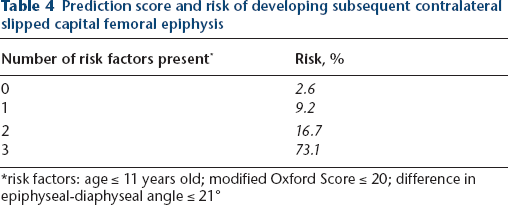
risk factors: age ≤ 11 years old; modified Oxford Score ≤ 20; difference in epiphyseal-diaphyseal angle ≤ 21°
Discussion
The risk of subsequent contralateral SCFE after index SCFE is relatively high, and varies based on the presence of several risk factors. In this study, the rate of subsequent contralateral SCFE was noted to be 18%, which is consistent with previously reported rates.15,17,32 We found several significant risk factors for the development of subsequent contralateral SCFE. Specifically, younger age, lower modified Oxford Score and a smaller difference in epiphyseal-diaphyseal angle between both hips were highly predictive of a contralateral slip. If a patient was ≤ 11 years of age, had a modified Oxford Score ≤ 20 and difference in epiphyseal-diaphyseal angle ≤ 21° at the time of index presentation, the risk of subsequent contralateral SCFE was 73%. The findings from this study suggest that these three risk factors should be assessed in each patient presenting with unilateral SCFE in order to stratify risk and identify patients at risk for developing a subsequent contralateral SCFE.
Previous studies have assessed risk factors for subsequent contralateral SCFE. For example, younger age at the time of index SCFE has been noted to be a risk factor for subsequent contralateral SCFE in several studies.14,17,23,33–35 More specifically, Bidwell and Susan Stott 34 noted that age < 12 years old had an odds ratio of 3.81 for the development of subsequent contralateral SCFE, and Swarup et al 17 noted that patients that developed a contralateral SCFE were significantly younger than patients that did not develop a contralateral SCFE (11.3 years old versus 12 years old) in a large database study. Similarly, a recent meta-analysis found that patients that developed a contralateral SCFE were approximately one year younger than patient that did not develop a subsequent contralateral slip. 23
The modified Oxford Score has also been studied as a proxy for skeletal maturity, and it has been noted to be lower in patients that develop a subsequent contralateral SCFE.20,23,36 Specifically, Stasikelis et al 36 noted that subsequent slips happened in 85% of patients with a modified Oxford Score of 16 and no patients with a score ≥ 22. Similarly, Popejoy et al 20 noted that a modified Oxford Score of 16 to 18 was 96% predictive of a subsequent contralateral SCFE. In addition, Popejoy et al 20 looked at the different components of the modified Oxford Score and noted that an open triradiate cartilage may be the strongest predictor. In this study, however, we did not find the status of the triradiate cartilage to be a significant predictor, but did find that the overall modified Oxford Score was a significant predictor of subsequent contralateral slip.
The magnitude of the epiphyseal-diaphyseal angle has been investigated as a risk factor for subsequent slip in two studies.26,35 Mestriner et al 26 looked at the epiphyseal-diaphyseal angle of the unaffected side in patients that did and did not develop a contralateral SCFE. They reported that a higher epiphyseal-diaphyseal angle of the unaffected side predicted a slip of the unaffected side 2 Similarly, Loder et al 35 evaluated the difference in epiphyseal-diaphyseal angle between both hips at the time of index SCFE, which represents the true slip angle as originally described by Southwick. 27 Loder et al 35 found a smaller difference in epiphyseal-diaphyseal angles between the affected and unaffected sides at the time of index SCFE, and interestingly, the difference in epiphyseal-diaphyseal angles in patients that developed a contralateral SCFE was 21°, the same criteria used in the present study. Intuitively, a higher epiphyseal-diaphyseal angle of the unaffected side and a smaller difference in epiphyseal-diaphyseal angles between the affected and unaffected sides are related, and these previous studies support the findings of this study.
The findings of this study have several implications to clinical practice. This study identifies significant factors for subsequent contralateral SCFE, which will aid in patient counselling and surgical decision making. Surgeons and trainees evaluating patients in the emergency room can obtain imaging of the contralateral hip and calculate the prediction score by assessing the patient's age, modified Oxford Score and difference in epiphyseal-diaphyseal angle between the affected and unaffected sides. If all criteria are satisfied, prophylactic pinning of the contralateral hip should be recommended. If some criteria are satisfied, the risk of subsequent contralateral SCFE should be discussed with the patient and caregivers based on the number of risk factors. Additionally, patients without any of these risk factors have a risk that is < 3% and can be safely observed. In general, stratifying risk using this algorithm will help to improve patient selection and minimize the risk of unnecessary surgery. 24
This study has several limitations. First, this is a retrospective study performed at a single tertiary care centre and it only includes patients that were treated for a subsequent contralateral SCFE at our institution. These limitations may introduce selection bias and decrease the generalizability of the findings. However, this patient sample includes patients of all major ethnicities and the distribution of sex is similar to previous studies. 17 Additionally, all patients had a minimum two-year follow-up and all cases of contralateral SCFE were confirmed by chart and radiographic review, which improves the reliability of the data. In general, future studies that include large prospective cohorts are needed to validate these findings. Secondly, all radiographic measurements in this study were performed by a single observer. We did not control for issues relating to interobserver and intraobserver reliability, and decided to use a single observer for internal consistency. Multi-centre studies are needed to confirm the reliability of these radiographic measures and confirm their utility in calculating this prediction score. Similarly, radiographic measurements are subject to variability based on patient positioning for radiographic views, and future studies with standard techniques are needed. Lastly, this study likely underestimates the risk of subsequent contralateral SCFE since patients were followed for a minimum of 24 months after unilateral SCFE, and we excluded patients that underwent prophylactic pinning of the contralateral hip during their index presentation. The most common reasons for prophylactic pinning at our institution are young age, skeletal immaturity and presence of endocrine abnormality, and the results of this study are specific to patients without these traditional risk factors. It is important to note that despite our practice, the presence of endocrine disorders was not found to be a significant predictor in this study. In general, additional studies are needed focusing on the natural history of patients with unilateral SCFE in order to clearly determine the time-frame, risk and risk factors for subsequent contralateral SCFE.
In conclusion, there is a significant risk of subsequent contralateral SCFE in patients with unilateral SCFE, and significant risk factors include younger age, lower modified Oxford Score and smaller difference in epiphyseal-diaphyseal angle between the affected and unaffected hips. Using a criteria of age ≤ 11, modified Oxford Score ≤ 20 and difference in epiphyseal-diaphyseal angle ≤ 21°, it is possible to predict most cases of subsequent contralateral SCFE. If patients present with all of these risk factors, prophylactic pinning of the contralateral hip should be performed. If none of these risk factors are present, patients can be safely observed for development of a subsequent contralateral slip. In general, this prediction score should be utilized when evaluating all patients presenting with a unilateral SCFE.
Footnotes
RS: Data acquisition, Data analysis, Manuscript preparation.
SG: Data acquisition, Manuscript preparation.
KB: Study design, Data analysis, Manuscript preparation.
WS: Study design, Data analysis, Manuscript preparation.