
Abstract
Flexible intramedullary nailing (FIN) is the gold standard treatment for femur fracture in school-aged children. It has been performed successfully in younger children, although Spica cast immobilisation (SCI) has been the most widely used strategy to date.
Method
A retrospective analysis was performed between two comparable groups of children aged 1–4 years with a femoral shaft fracture. Two University hospitals, each using specific treatment guidelines, participated in the study: SCI in Group I (Basel, Switzerland) and FIN in Group II (Lausanne, Switzerland).
Results
Group I included 19 children with a median age of 26 months (range 12–46 months). Median hospital stay was 1 day (range 0–5 days) and casts were retained for a median duration of 21 days (range 12–29 days). General anaesthesia was used in six children and sedation in four. Skin breakdown secondary to cast irritation occurred in two children (10.5%). The median follow-up was 114 months (range 37–171 months). No significant malunion was noted. Group II included 27 children with a median age of 38.4 months (range 18.7–46.7 months). Median hospital stay was 4 days (range 1–13 days). All children required general anaesthesia for insertion and removal of the nails. Free mobilisation and full weight bearing were allowed at a median of 2 days (range 1–10 days) and 7 days (range 1–30 days), respectively, postoperatively. Nail exteriorisation was noted in three children (11%). The median follow-up was 16.5 months (range 8–172 months). No significant malunion was reported.
Conclusions
Young children with a femoral shaft fracture treated by SCI or FIN had similarly favourable outcomes and complication rates. FIN allowed earlier mobilisation and full weight bearing. Compared to SCI, a greater number of children required general anaesthesia. In a pre-school child with a femoral shaft fracture, immediate SCI applied by a paediatric orthopaedic team following specific guidelines allowed early discharge from hospital with few complications.
Introduction
Flexible intramedullary nailing (FIN) is a standard treatment for femoral shaft fractures in children between 5 and 10 years of age [1]. It is also an option in children younger than 5 years of age [2, 3]. However, in this young age group, Spica cast immobilisation (SCI) with or without previous traction has so far been the method of choice. With SCI, 3–4 weeks of immobilisation are necessary and leg length discrepancy, malunion, skin breakdown, foot drop or even compartment syndrome have been described [4–6]. FIN shortens the period of limb immobilisation and avoids cast-specific complications [7]. FIN has recently been performed in pre-school children with the same advantages as for older children [2, 3]. To our knowledge, no one has yet compared FIN with SCI in pre-school children with a femur fracture. The aim of our study was to compare the benefits and outcomes of two clinically comparable groups of children aged 1–4 years with a femoral shaft fracture treated with FIN or SCI.
Method
A retrospective comparative analysis of two groups of children aged 1–4 years who sustained a non-pathological femoral shaft fracture was performed. Group I consisted of children treated by SCI between 1992 and 2002 at the University Children's Hospital of Basel, Switzerland. Immediate SCI was the treatment of choice in this institution. A period of traction up to 24 h was applied for fractures with significant shortening. A hip spica including the foot, the thigh of the injured leg and a pelvic ring was applied for a period of 2–4 weeks, depending on callus formation as assessed on follow-up radiographs. General anaesthesia was performed if pain control was insufficient with sedation or if the fracture was considered very unstable by radiological evaluation. Oral pain medication including AINS (analgesic-antipyretic-anti inflammatory) and paracetamol was always prescribed. Standard AP and lateral radiographs were performed on days 0 and 7, and following removal of the cast.
Group II consisted of children treated by FIN between 1991 and 2006 in the department of paediatric surgery at the University Hospital of Lausanne, Switzerland. Shortly after Metaizeau's original description [8], FIN was used extensively in this institution without strict age limitation. A standardised surgical procedure was conducted by seven board-certified paediatric surgeons. Mobilisation on oral pain medication was allowed the day after surgery. Weight bearing was started on a case by case basis. Standard AP and lateral radiographs were performed before discharge, and on days 30 and 90 post-operatively (as illustrated below).
The differences in treatment protocol between the two institutions gave us the opportunity to compare two clinically comparable groups of children with similar femur shaft fractures. Hospital care, outcome and complications rate were assessed. In both institutions, the patients were followed at regular intervals for a minimum of 2 years. The age of the child and the characteristics of the femur fracture were recorded. The defined primary outcome was evaluation of malunion 6 months after trauma. Malunion was defined as a visible lower leg deformity, which could be secondary to more than 10° rotation discrepancy by means of clinical evaluation, clinically visible angulation when compared with the healthy leg, confirmed and measured on the radiographs, or more than 2 cm leg length discrepancy. General anaesthesia, reoperations, secondary fracture displacement, infection or local skin irritation by cast or pin were recorded. The length of stay in hospital was calculated. Time to return to free weight bearing was evaluated.
The two groups were compared using the Mann–Whitney test. A P value of less than 0.05 was considered statistically significant. The 95% confidence intervals and odds ratio were provided for presented outcomes when appropriate.
Results
The fracture types of both groups are illustrated in Table 1.
Distribution of fracture type in the two patient groups
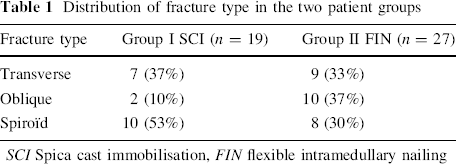
SCI Spica cast immobilisation,FIN flexible intramedullary nailing
Group I included 19 children with a median age of 26 months (range 12–46 months). There were 7 transverse, 2 oblique and 10 spiral femoral mid-shaft fractures. SCI was applied within hours following admission, except for one child in whom traction was applied for 24 h prior to casting. General anaesthesia was used in six children and sedation in four children. The median hospital stay was 1 day (range 0–5 days) and the cast was kept for a median of 21 days (range 12–29 days). After removal of the cast and radiographic evaluation of the callus, the child was allowed to start walking without restrictions. Complications occurred in two children (10.5%); one had clinically significant skin pressure points over a wet cast and one suffered from local skin breakdown. Both healed completely after cast replacement and local skin care. The median follow up was 114 months (range 37–171 months). No significant malunion was noted, with a leg length discrepancy of 0.5–1 cm measured in only five children.
Group II consisted of 27 children with a median age of 38.4 months (range 18.7–46.7 months) with 9 transverse, 10 oblique and 8 spiral fractures. All children required general anaesthesia for nail insertion and removal, with a median of 101 days (range 59–161 days) between the procedures. They stayed in hospital for a median of 4 days (range 1–13 days). Unrestricted mobilisation and weight bearing were allowed at a median of 2 days (range 1–10 days) and 7 days (range 1–30 days), respectively, following FIN. Distal nail exteriorisation was noted in three children (11%). One child required general anaesthesia and antibiotics to shorten the nail and close the skin. This complication occurred only prior to year 2000, when a new nail cutter became available. This devise allowed shorter cuts of the nail, leaving less metal protruding out of the bone, therefore avoiding skin breakdown. One child made an uneventful recovered following a short post-anaesthetic anaphylactic shock of unknown origin (Figs. 1, 2).
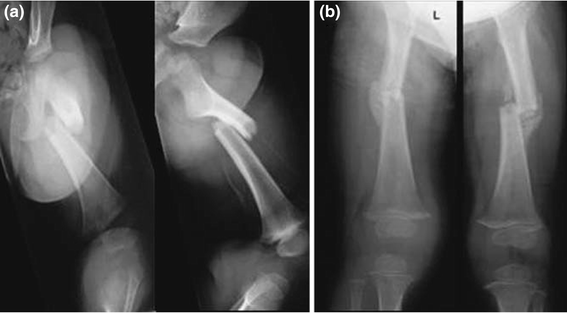
Spica cast. An 18-month-old boy with femoral shaft fracture.

Radiographic studies of flexible intramedullary nailing (FIN).
Two children left Switzerland soon after FIN and three children did not come back to the clinic after nail removal. For the remaining 22 children, a median of 16.5 months (range 8–172 months) follow up was available. No significant malunion was reported, and a leg length discrepancy of 0.5–1.7 cm was measured in four cases (18.2%).
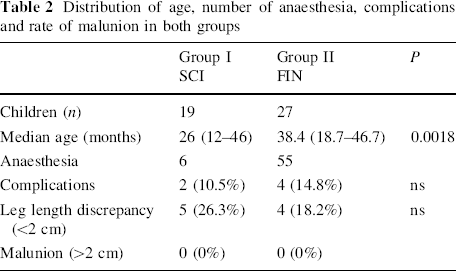
Table 2 and Fig. 3 summarise the results and illustrate age, complication rate and outcome in both groups. The relative risk of a child treated with SCI to have a complication was 0.67 (95% CI 0.11–4.13) when compared with a child treated with FIN. The relative risk of child treated with SCI to have a <2 cm leg length discrepancy was 2.05 (95% CI 0.47–8.95) when compared with a child treated with FIN. These results did not reach statistical significance.
Distribution of age, number of anaesthesia, complications and rate of malunion in both groups
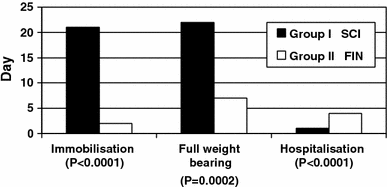
Difference in median length of immobilisation, median time to full weight bearing and median length of stay in hospital in both groups
Discussion
Spica cast immobilisation is a simple, effective and safe treatment for a femoral shaft fracture in children. It remains universally used in all aged groups, but is especially suited for children under the age of 5 years, when there is still significant potential for remodelling [6, 9] and the weight of child and cast allow for easy carrying and transfer. Over the last 20 years, FIN has proven more effective than SCI, avoiding the burden of the cast while significantly shortening the duration of immobilisation and the time to full weight bearing [1]. The lower age limit for FIN has yet to be defined and most publications now refer to the onset of the school-aged period (5–6 years old) as the lower limit [10]. The AAOS 1 Clinical Practice Guideline for the treatment of paediatric diaphyseal femur fracture suggests early SCI or traction with delayed SCI in children aged 6 months to 5 years [11]. In today's Western society, children are going to kindergarten at a young age. Often both parents are working. Applying FIN to pre-school children is attractive and feasible [2, 3] but its advantages over SCI had yet not been evaluated.
AAOS: American Academy of Orthopaedic Surgeons.
In group I, pre-cast traction for 24 h was deemed necessary only in one child, allowing an early return home shortly after SCI. Complications were limited to cast and skin issues. This did not affect fracture healing. No permanent skin damage was observed and the two affected children healed completely. We conclude that, in treating pre-school children with femoral shaft fractures, a trained medical team applying immediate SCI using a strict protocol could achieve optimal results. In Basel, the paediatric trauma team could also count on compliant, well informed and trusting parents.
In group II, the lower end nail exteriorisation was a technical failure, but this has been avoidable since 2000 when a new nail cutter (TEN Cutter 359.217; Synthes®, Oberdorf, Switzerland), became available. In accordance with a previous study, we did not find any relationship between the type of fracture and the occurrence of nail exteriorisation [3]. From a review of both medical records and the literature, we found no evidence to support a relationship between the anaphylactic shock and the titanium nails used for FIN. Therefore, we do not consider it to be a complication of FIN.
General anaesthesia or sedation was required 55 times in group II (100%) compared to only 10 times in group I (52.7%). This difference is significant and has safety, financial as well as emotional impacts that are beyond the scope of the study.
As in older children, the muscle of the injured thigh can be painful and relative stability of FIN can produce anxiety when mobilising the leg for the first time. It always takes time for the injured child to start to move without difficulty. The median length of stay in hospital was limited to 1 day in group I, compared to a median of 4 days (1–13 days) in group II (P < 0.001). This period of time resting in bed was necessary to control pain and allow progressive safe mobilisation after FIN. The amount of pain in children discharged home following FIN and SCI was not properly recorded in the medical records and could not be assessed.
Compared to group I, mobilisation was faster (2 days, P < 0.0001) and weight bearing was allowed earlier (7 days, P = 0.0002) in group II. This was in accordance with the basic principles of FIN, which aims at early mobilisation and weight bearing. This retrospective study did not allow us to further assess the advantages of early mobilisation, especially with regards to the impact on muscle atrophy and social development, as well as on parents or guardians missing days at work. The theoretical positive impact of early mobilisation and full weight bearing on a very young child remains to be evaluated.
The rate of leg length discrepancy in groups I (26.3%: 0.5–1 cm) and II (18.2%: 0.5–1.7 cm) was never clinically significant, and was similar to what is found in the literature [1, 12]. A significant malunion, as defined by our criteria, did not occur. Overgrowth was not specifically evaluated, but did not affect bone length negatively in either group. However, the number of cases studied was not large enough to evaluate the risk of malunion with either treatment modality.
In conclusion, children younger than 5 years old with a femoral shaft fracture treated by SCI or FIN had similarly favourable outcomes and rates of complication. FIN required more time in hospital and more anaesthesia, but allowed earlier mobilisation and weight bearing.
In a child aged 1–4 years with a femoral shaft fracture, immediate SCI applied by a paediatric orthopaedic team following specific guidelines allowed early discharge from the hospital, few complications and general anaesthesia without significant malunion. Although a valuable and feasible option, FIN did not show any significant advantage over immediate SCI.
A prospective study between FIN and SCI including evaluation of total costs, post-immobilisation pain and socio-economic consequences is necessary to further refine current AAOS recommendations [11].