
Abstract
Introduction
Optimal paediatric femoral shaft fracture patterns or lengths amenable to titanium elastic nail stabilization have not been well defined. The purpose of this study is to identify radiographic parameters predictive of treatment failure with flexible intramedullary nails based upon fracture morphology.
Methods
A retrospective review was performed of all femoral shaft fractures treated with flexible intramedullary nails over a five-year period. All patients with at least six weeks of postoperative radiographic imaging were included. Fracture characteristics included location, pattern, length, obliquity, angulation, translation and shortening. Postoperative radiographs were reviewed to determine shortening and angulation.
Results
There were 58 patients with 60 femoral shaft fractures stabilized with titanium nails, with 46 healing within acceptable parameters and 14 considered malunions. Six of the 14 malunions developed complications requiring early unplanned intervention. No patients in the treatment success group had a complication. Between the treatment success and failure groups, fracture pattern, location, length, obliquity, angulation, translation or shortening were not statistically different. Mean nail canal fill was significantly lower in the failure group (0.72 versus 0.81; p = 0.0146), with a receiver operating characteristic curve identifying canal fill 76% as the optimal threshold.
Conclusion
This is the first study to measure the length and obliquity of paediatric femoral shaft fractures and to determine their relationship to radiographic alignment after healing. None of the preoperative fracture characteristics were predictive of malalignment or shortening. We recommend the use of larger nail sizes in the treatment of paediatric femoral shaft fractures, especially if there is concern for residual instability.
Level of evidence
IV
Introduction
The treatment of femoral shaft fractures in the paediatric population typically depends on the patient's age, weight and injury pattern. Titanium elastic nails (TENs), a type of flexible intramedullary nail, are an accepted treatment for paediatric femoral shaft fractures in ages five to 11 years and in those weighing < 50 kg.1,2 The fracture pattern can also play a significant role in the surgical treatment of these injuries. 3 Length-stable patterns, such as transversely oriented fractures, are ideal candidates for flexible intramedullary nailing due to the fracture configuration's ability to resist shortening. Length-unstable patterns can shorten or angulate due to the pattern of the fracture, and flexible intramedullary nails are often discouraged in these cases. To our knowledge there is no literature in this patient population defining the spectrum of stability in paediatric femoral shaft fractures based on fracture pattern or obliquity when using TEN fixation.
Prior literature on this subject has analyzed fracture stability from a binary perspective – first, by defining fractures as stable or unstable, and then reviewing the outcomes and complications.2–5 Instead, our aim was to examine fracture stability in a continuous manner. Our hypothesis is that there is a certain threshold at which the length, obliquity or initial displacement of a given fracture becomes amenable to TEN fixation and, therefore, can be considered a stable fracture pattern. Specifically, we sought to determine whether fracture length, fracture obliquity, initial displacement, angulation or shortening had any correlation with final shortening or angulation following TEN stabilization.
Materials and methods
After approval by the institutional review board, a retrospective review was performed of all patients who underwent TEN stabilization for femoral shaft fractures at a single regional Level 1 trauma centre between January 1, 2013 and March 31, 2019. Inclusion criteria included all patients who underwent operative stabilization of a traumatic femoral shaft fracture. Exclusion criteria included patients with pathological fractures, neuromuscular disorder or underlying congenital musculoskeletal disorder. The indication for TEN use was at the discretion of the treating surgeon. Patient demographic data and concomitant injuries were obtained through medical chart review. Operative reports were reviewed for pertinent surgical details including implant size.
Initial injury radiographs were reviewed to determine fracture location (subtrochanteric, supra-isthmic, isthmic, infra-isthmic, meta-diaphyseal), fracture pattern (transverse, oblique, spiral butterfly), fracture line obliquity relative to the anatomical axis of the femoral shaft (degrees), fracture angulation in the coronal and sagittal planes (degrees), maximal fracture translation in either the coronal or sagittal planes (measured as percent of the cortical width at the fracture) and fracture shortening (percentage of cortical width). Final saved intraoperative fluoroscopic images obtained prior to leaving the operating room were reviewed to measure operative reduction, specifically fracture angulation, shortening and translation. Postoperative full-length anteroposterior (AP) and lateral femur radiographs obtained within six weeks after surgery, after bridging callus formation but before full healing and remodelling, were used to measure final angulation, shortening and translation. Nail canal fill relative to the femoral isthmus was measured on the AP femur radiograph. Shortening as a percentage of canal width was then converted to millimeters based on radiographic calibration using the nail diameter from intraoperative documentation. We selected 5° of apex anterior sagittal plane angulation as the normal baseline to represent normal anatomical femoral bowing.
We defined treatment failure radiographically, specifically as excessive shortening or angulation based on previously published and widely accepted age-based standard guidelines. 6 Patients fall into one of three age groups: ages two to five years, six to ten years and > 11 years. Acceptable varus or valgus angulation is < 15°, < 10° and < 5°, respectively. Acceptable anterior/posterior angulation is < 20°, < 15° and < 10°, respectively. Acceptable shortening is < 20 mm, < 15 mm and < 10 mm, respectively. Complications were defined as loss of reduction requiring a secondary intervention such as manipulation, cast placement or adjustment or unplanned return to the OR for revision or removal of implants. Treatment success was defined as those who healed within the standard radiographic parameters without any secondary intervention. A power analysis was performed to ensure that an effect size of 1.0 between the treatment success and failure groups would be detectable, and this revealed a sample size of 44 fractures for 80% power. To compare our cohort with the prior literature, instead of separating patients by treatment outcomes, patients were also separately analyzed by dividing the cohort into two groups based on fracture length irrespective of treatment success or failure. This created a length stable group with fracture length less than twice the cortical width, and a length unstable group with fracture length greater than twice the width.
Surgical technique
All patients were treated by fellowship-trained orthopaedic paediatric or trauma surgeons. Retrograde TENs (Depuy Synthes, Raynham, Massachusetts) were inserted in standard fashion through small several-centimetre incisions along the medial and lateral aspects of the distal femur, approximately 2 cm to 3 cm proximal to the distal femur physis. 7 All rods were bent manually in a C-shape and specific surgical techniques were up to the discretion of the treating surgeon. The decision to use adjunctive casting or knee immobilizer at the conclusion of the procedure as well the length of immobilization was determined by the surgeon.
Statistical analysis
Continuous variables (e.g. angle) were reported as mean (sd) and range. Categorical variables (e.g. sex) were reported as number of patients or percentage of patients. A Fisher's exact test was used to determine differences between categorical variables. Either a paired t-test or Wilcoxon rank-sum test was used to determine differences between continuous variables depending on the distribution of data. Multiple logistic regression was used to assess associations between injury variables and treatment outcomes. A receiver operating characteristic (ROC) curve was utilized to determine thresholds for continuous variables. Computations were performed with statistical software (JMP Pro, 15.0, Cary, NC, USA) and significance was set at p < 0.05.
Intraobserver reliability
Each measurement was performed by four co-authors (AKS, AMS, KSH, HBL) viewing the same screen and measurement tool until there was complete agreement for that measurement, yielding a consensus measurement for the given variable. We, therefore, chose to consider all measurements to be done by a single observer. To assess intraobserver reliability, the same measurements were repeated by the same four co-authors five months later based on ten randomly selected patients. Statistical software was used to generate intraclass correlation coefficient (ICC) for each specific measurement. The mean ICC was 0.89 (0.60 to 0.98), indicating good to excellent reliability.
Results
There were 58 patients and 60 femoral shaft fractures treated with TEN who met the inclusion criteria. Patient demographic data is listed in Table 1. All radiographic parameters such as angulation, translation and shortening were within acceptable age-based ranges at the immediate postoperative period. Final postoperative radiographic measurements were obtained at a median of 36 days (interquartile range (IQR) 28 to 43). Radiographic follow-up was available for a median of 203 days (IQR 108 to 305). Of the 60 femora included in this study, 46 (77%) went on to heal without any notable angular deformity based on the criteria previously mentioned, whereas 14 (23%) developed excessive malalignment or shortening. 6 There were no nonunions. A total of 15 fractures were placed into a cast at the conclusion of the surgical procedure for additional immobilization. Three of these 15 casted fractures (20%) went on to radiographic failure. When removing the 15 casted fractures from the entire cohort, there were 45 femoral shaft fractures and 11 failures, giving a 24% failure rate when evaluating only fractures without adjunctive cast immobilization.
Patient demographics
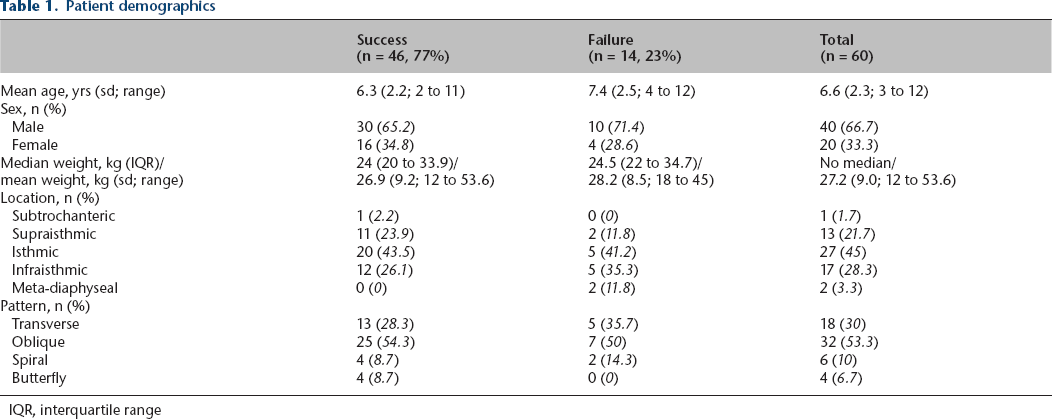
IQR, interquartile range
There were no statistically significant differences in patient age (p = 0.14), weight (p = 0.52), sex (p = 0.76), the distribution of fracture patterns (p = 0.70) and fracture locations (0.13) between the treatment success and failure groups. There were also no statistically significant relationships between any preoperative injury measurement and treatment failure. Specifically, fracture length (p = 0.54), fracture obliquity (p = 0.61), angulation (coronal p = 0.62 and sagittal p = 0.87), translation (p = 0.12) and shortening (p = 0.71) were not statistically different between the success and failure groups. Mean canal fill was significantly lower in the failure group than the success group (0.72 (sd 0.10) versus 0.81 (sd 0.08); p = 0.0146; Fig. 1). Based on the resulting ROC curve, the optimal threshold for canal fill was 76.47% (area under curve 0.74).
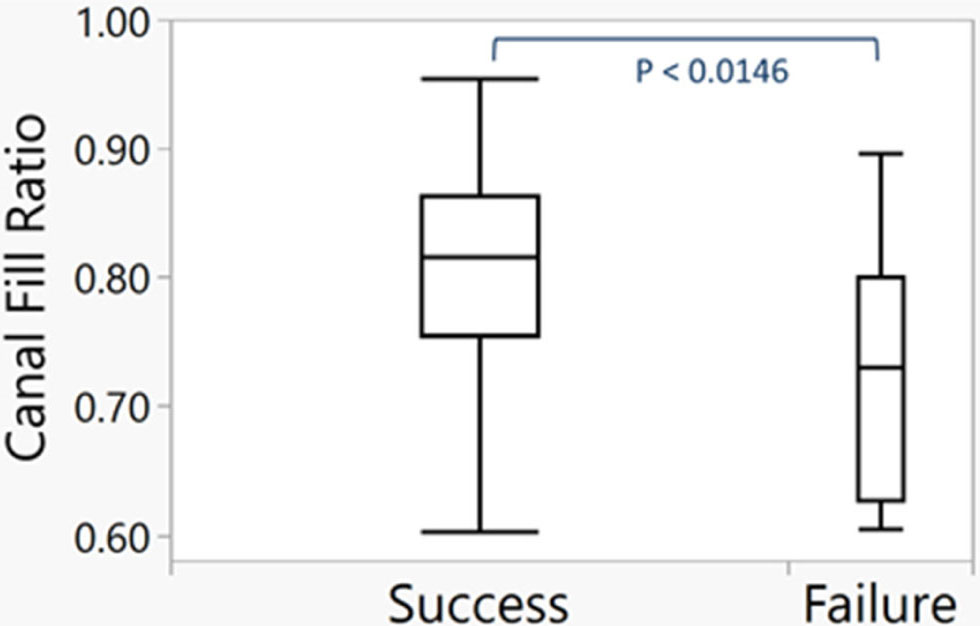
Box and whiskers plot demonstrating significant difference between nail canal fill of the success and failure groups (p = 0.0146).
Failures
Examining the treatment failures, 11 cases had excessive angulation and three cases had shortening > 2 cm. Seven fractures were oblique, five were transverse and two were spiral. Median fracture length was 54% (IQR 19% to 160%) of cortical diameter and median obliquity was 23.5° (IQR 4.5° to 41.5°). Compared with the treatment success group, the median fracture length and median fracture obliquity were not significantly different (p = 0.5350 and p = 0.6060, respectively). Canal fill was < 80% in 12 patients while two patients had canal fill ≥ 90%. These two patients with canal fill ≥ 90% had transverse and short oblique (fracture angle of 26° and fracture length of 76% cortical diameter) patterns and failed by angulation without any shortening. Of the three fractures that shortened excessively, all had fracture length greater than twice the cortical width and canal fill < 80%.
Complications
Six patients had loss of reduction leading to an unplanned or early secondary intervention and all of these were a subset of the treatment failure cohort. No complications were seen in the treatment success group. Four patients had loss of fracture reduction that led to early implant prominence thereby prompting early removal of a nail. Two patients were noted to have early loss of reduction that required repeat reduction and cast placement; one hip spica cast and one long leg cast. The patient with the hip spica cast developed an early postoperative neurovascular concern that required cast removal and subsequent submuscular plating. Two patients with early implant removal had shortening > 2 cm. One patient with excessive sagittal plane malalignment also had clinical malrotation noted on postoperative examination, though the nails were removed routinely and no secondary intervention was performed by the one-year postoperative follow-up visit.
Length unstable group
To compare our cohort with the prior literature, patients were also analyzed by dividing the cohort into two groups based on fracture length: a length stable group with fracture length less than twice the cortical width, and a length unstable group with fracture length greater than twice the width. There were 48 length stable fractures with 11 failures (23%) and 12 length unstable fractures with three failures (25%). These three failures within the length unstable group all occurred via shortening beyond acceptable criteria rather than by angulation, and the canal fill for each of these three were below 70%.
Discussion
To our knowledge, this is the first study to measure the length and obliquity of femoral shaft fractures and to determine their relationship to radiographic alignment after healing. Fracture length as a percentage of cortical diameter, fracture angle relative to the anatomical axis, and fracture location were not correlated with shortening, malalignment or complications. Injury severity based on parameters measured from static injury films, including initial displacement, angulation and shortening, were not predictive of treatment failure or complications. Alignment after TEN stabilization seen on intraoperative fluoroscopy also were not predictive of treatment outcomes. The only variable found to correlate with treatment failure was nail canal fill or nail diameter to medullary canal diameter. Consequently, this study suggests that femoral shaft fractures previously thought to be unstable patterns can be successfully treated with TENs (Fig. 2).

Example of a five-year-old patient with a (a) long oblique pattern that was treated with titanium elastic nail and (b) healed within the acceptable radiographic parameters.
Historically, TEN was thought to be best suited for transverse fracture patterns given the ability for bony apposition at the fracture to maintain axial length, and these were considered length stable patterns. On the other hand, length-unstable patterns, such as long oblique, spiral or comminuted fractures, have been thought to be poor candidates for TEN due to their ability to slide and/or shorten with axial load. No studies have attempted to objectively define the threshold between length stable and unstable patterns. The literature is mixed on whether certain fracture characteristics place some fractures at higher risk of treatment failure.2–5 This discrepancy may be related to the manner in which fracture stability is defined in this population, and we attempted to build off of that work by assessing stability in a more objective manner.
Complications associated with fracture pattern stability were first reported on by Sink et al, 3 who reviewed their experience with TEN use by dividing all of their patients into two stability groups. Comminuted and long oblique fractures were combined into a length-unstable group, with long oblique defined as fracture length greater than twice the femoral diameter at the fracture site. They found a major complication rate of 25% which was similar to our findings, and the rate was much higher in the length unstable group. Shortening or angulation occurred in 75% of their length unstable patterns compared with 12.5% in the length-stable group. Of the patients who required reoperation, 75% had length-unstable injury patterns. They also found a higher complication rate when the canal fill was < 80%. In a follow-up study after narrowing their use of TEN to mostly stable fracture patterns, Sink et al 4 found a significantly decreased complication rate, though they also noted an increased use of larger nail diameters than in their first study. More recently, Siddiqui et al, 5 attempted to determine treatment outcomes in length-unstable patterns using the same definition of stability as described by Sink et al.3,4 They found an overall complication rate of 47% but major and minor complication rates were not statistically different between the length-stable and length-unstable groups. Although the length-unstable group had lower mean canal fill compared with the length-stable group, there were no differences in incidence of angular deformity or symptomatic implant between the two groups, supporting the use of TEN in all fractures regardless of pattern. Patients with complications had no difference in mean canal fill compared with those without complications. In contrast, our study attempted to objectively define fracture stability by analyzing final radiographic alignment and correlating those measurements with fracture length, obliquity and displacement as continuous variables.
The literature is mixed on whether canal fill is predictive of complications. Early on, multiple authors recommended achieving a nail canal fill of 80% and this was subsequently supported by biomechanical data showing the strongest resistance to torsional and bending loads with higher canal fill.8–11 Other recent studies have shown no correlation between canal fill and radiographic outcome.5,12,13 The treatment failure group in our patient series had a significantly lower mean canal fill than the success group. Our ROC analysis identified 76% as the minimum optimal canal fill to prevent treatment failure, which closely matches the generally accepted recommendation of at least 80%. Notably, two patients with canal fill ≥ 90% still went on to failure, and both were in stable patterns, demonstrating that neither adequate canal fill nor having ‘stable’ fracture pattern guarantees acceptable alignment at fracture union. Additionally, of the so-called ‘length unstable’ fractures, all failures occurred in those with canal fill ≤ 70%. Lastly, all four patients with butterfly fragments went on to heal without malunion, further highlighting successful use of TEN for fractures traditionally considered to be unstable. We believe that the literature may be in disagreement over the importance of canal fill because most studies are retrospective and underpowered to identify the specific fracture patterns that would benefit from larger canal fill. That is, canal fill may be an important surgical factor in a certain subset of paediatric femoral shaft fractures, and our results suggest that the more ‘unstable’ fracture patterns are the ones more likely to benefit from increased canal fill. Formulating a larger, prospective study to investigate canal fill would be a useful addition to the literature.
In our series, all complications were a subset of the treatment failure cohort, demonstrating a clear association between need for additional intervention and loss of reduction. This is demonstrated by the fact that all six patients who required casting or early implant removal had radiographic treatment failure based on our evaluation criteria. Therefore, although minor changes in fracture length or alignment after TEN stabilization do not always lead to complications, it can progress and necessitate an unplanned secondary intervention and increase patient morbidity. This highlights the importance of maintaining alignment during the healing period.
This study has several limitations. First, this is a retrospective review from a single institution with a relatively small sample size and with the usual biases associated with a retrospective analysis. Specifically, the patient selection, indications for flexible intramedullary nailing, surgical techniques and decision for adjunctive casting were dependent upon the treating surgeon. Delineating the population that would benefit from adjunctive immobilization would be an important area of future research. Second, the follow-up period was short while the radiographic measurements were performed at non-uniform timepoints following surgery. Measurements were performed prior to full healing and remodelling to more accurately measure fracture displacement following stabilization. Rotation is challenging to measure on plain radiographs and therefore was not assessed during this study. The one patient with malrotation determined on physical examination also had a sagittal plane malalignment, placing him in the failure cohort, but there could be additional unrecognized patients with rotational deficits. We may, therefore, be underestimating the incidence of malunion by underappreciating malrotation during routine radiographic follow-up, and identifying a quick, objective measurement poses an interesting challenge as we refine our treatment for these injuries.
The results of this study do not consider the long-term remodelling potential of the fracture and of the entire limb as the patient ages.14–16 Although this calls into question the clinical significance of our radiographic findings, we believe our goal as orthopaedic surgeons is to restore native limb length, alignment and rotation whenever possible and especially with our surgical procedures. These results can help identify patients or injury characteristics that can be expected to exhibit some angulation or shortening during the healing period and require closer follow-up.
Conclusion
In conclusion, no specific measurement on injury radiographs was suggestive of fracture ‘stability’ in our series of paediatric femoral shaft fractures and they were not predictive of radiographic failure when measured after bridging healing. Fractures that went on to malalignment or shortening had lower mean nail canal fill. Our analysis showed an optimal threshold of at least 76% canal fill to minimize the incidence of malunion. With our cohort of patients, fractures with longer fracture length or greater obliquity were not shown to be at increased risk of shortening, malalignment or complications than short oblique or transverse patterns. Therefore, this study adds objective data to the body of literature for TEN use and suggests that TEN is a viable treatment option for paediatric femoral shaft fractures, irrespective of fracture length, pattern or location, as long as sufficiently large nail diameters are used.
Footnotes
AKS: Study design, chart review, performed measurements, data analysis, statistical analysis, manuscript preparation.
AMS: Study design, chart review, performed measurements, statistical analysis, manuscript preparation.
KSH: Chart review, performed measurements, statistical analysis, manuscript preparation.
BMH: Study design, data analysis, manuscript preparation.
HBL: Study design, performed measurements, data analysis, statistical analysis, manuscript preparation.