
Abstract
Abstract
Purpose
Distal femoral physeal fractures (DFPF) can cause growth disturbance that requires further surgical intervention. The aim of this study is to determine if Tibial Tuberosity Ossification Stage (TTOS) at the time of injury predicts secondary surgery for growth disturbance in patients who have sustained a DFPF.
Methods
We retrospectively investigated all patients who had operative treatment for a DFPF at a single centre over a 17-year period. Regression analysis was performed investigating associations between secondary surgery to treat growth disturbance and TTOS, age, Salter-Harris fracture classification type, mode of fixation or mechanism of injury.
Results
In all, 85 consecutive patients were identified. A total of 74 met the inclusion criteria. The mean age at time of injury was 13.1 years (2.0 to 17.1). Following fixation, 30 patients (41%) underwent further surgery to treat growth disturbance. Absence of tibial tuberosity fusion to the metaphysis was significantly associated with the need for further surgery (p < 0.001). Odds of requiring secondary surgery after tibial tuberosity fusion to metaphysis (compared with not fused) were 0.12 (95% confidence interval (CI) 0.04 to 0.34). The estimate of the effect of TTOS on reoperation rates did not vary when adjusted for gender, mechanism, fixation and Salter-Harris type. When accounting for age, the odds of any further operation if the tibial tuberosity is fused to the metaphysis (compared with not fused) were 0.28 (95% CI 0.08 to 0.94).
Conclusion
TTOS at the time of injury is a predictor of further surgery to treat growth disturbance in paediatric distal femoral fractures.
Level of Evidence
Diagnostic Level II
Introduction
Distal femoral physeal fractures are a recognized cause of growth disturbance and deformity in paediatric trauma patients.1–5 Both surveillance and management of the sequelae of distal femoral physeal fractures place a significant burden on patients, families and healthcare systems. This process could be facilitated if the likelihood of further procedures was established.
In physeal fractures, the relationships between the potential for remaining growth and the risk of progressive deformity (and hence the need for further surgery) are well understood.4,6,7 The tibial tuberosity is visible on plain radiographs taken to assess distal femoral physeal fractures either at initial injury or during the immediate perioperative period. The tibial tuberosity matures through an established sequence of radiologically progressive stages.8,9 This defined progression allows tibial tuberosity ossification to be used as a local estimation of remaining growth potential at the distal femoral physis. Our hypothesis is that tibial tuberosity ossification stage (TTOS) predicts the need for further reoperation in paediatric distal femoral physeal fractures.
Materials and methods
Ethical approval for this study was granted by the research and ethics committee at The Hospital for Sick Children, Toronto, Ontario, Canada.
Children with operatively managed physeal fractures of the distal femur were retrospectively identified by reviewing the theatre register at a level one paediatric trauma centre over a 17-year period since 2000.
The operative notes and radiographs at initial injury were reviewed. Fracture mechanism was divided into motor vehicle collision, field sports and snow sports (high-energy injuries from motorized snow vehicles were included in the first category). Fractures were classified in accordance with the Salter-Harris (SH) classification system. 10 Operative treatments were defined as manipulation and casting, crossed Kirschner-wires through the epiphysis, crossed screws through the epiphysis, open reduction with fixation via parallel screws through the Thurston Holland fragment, open reduction and plate fixation and external fixation.
TTOS at the time of initial injury was defined similarly to Vergara-Amador et al 9 as described in Figure 1. Stage 0 is when the secondary ossification centre of the tibial tuberosity is not visible on radiographs. Stage 1 is when the secondary ossification centre of the tibial tuberosity is evident but is distinct from both the metaphysis and proximal tibial epiphysis. Stage 2 is when the tibial tuberosity is fused with the proximal tibial epiphysis but not the metaphysis. Stage 3 is when the posterior vertical physis between the secondary ossification centre and the metaphysis is closing but the inferior notch is open. Stage 4 represents complete closure of the proximal tibial physis.
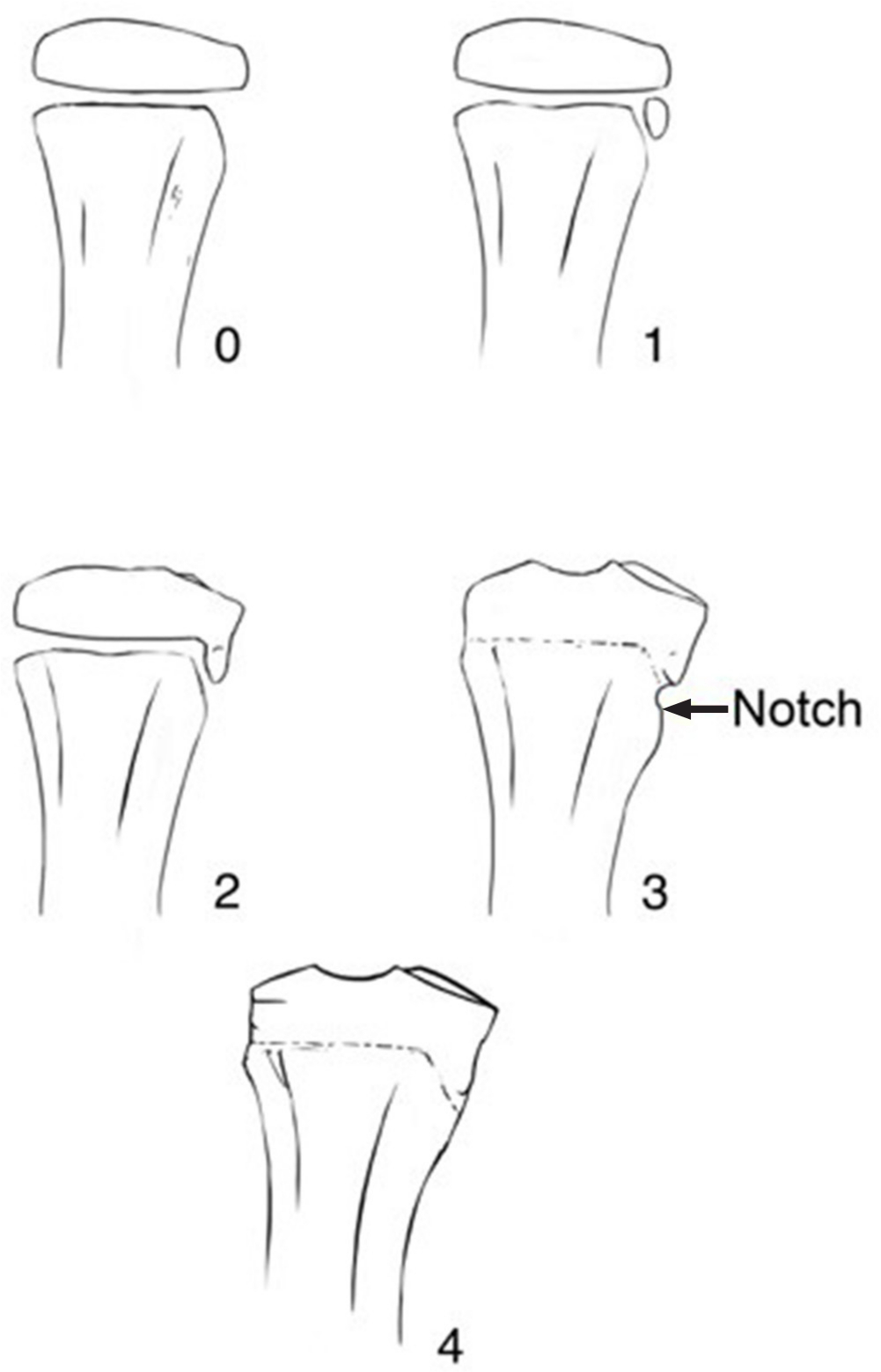
Tibial Tuberosity Ossification Stages.
TTOS was judged on the lateral radiograph of the injured limb taken at the time of injury or the first postoperative visit. In each case, the TTOS was assessed independently by two fellowship-trained paediatric orthopaedic surgeons (JK, DW) blinded to the other's assessment.
Medical records and radiographs for all patients were followed until discharge and any further surgical intervention was recorded. Where further operative treatment was required, surgery was classified by indication, treatment type and laterality.
Results
In all, 82 patients were identified. Six patients were excluded due to inadequate follow-up. One patient was excluded due to incomplete medical records. A further patient was excluded as they underwent bilateral distal femoral epiphysiodesis at the time of fracture treatment. Of the remaining 74 patients, there were 57 boys (77%) and 17 girls (23%). The mean age at time of initial injury was 13.1 years (2.0 to 17.1). The initial surgical management was parallel screws into the Thurston Holland fragment in 42 cases, crossed Kirschner-wires in 24 cases, closed reduction and casting in three cases, crossed screw fixation in three cases and plate fixation in two cases.
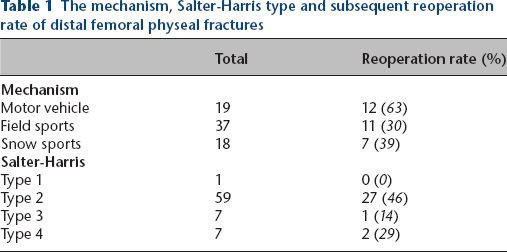
Table 1 details the mechanism of injury and Salter-Harris fracture type, and the associated reoperation rate.
The mechanism, Salter-Harris type and subsequent reoperation rate of distal femoral physeal fractures
Of the 74 physeal fractures of the distal femur, 30 patients (40.5%) required further surgical treatment to correct either limb-length deficiency or angular deformity. Five of these patients had surgery to address an angular deformity (due to growth disturbance rather than malreduction of the fracture), 23 were treated for limb-length difference and two for length and angulation. One patient had acute correction of an angular deformity, one had excision of a physeal bar, six were managed with a circular frame or magnetically-driven intramedullary lengthening device (with or without contralateral epiphysiodesis) and 22 patients underwent epiphysiodesis. These surgical cases are detailed in Table 2.
Cases requiring reoperation
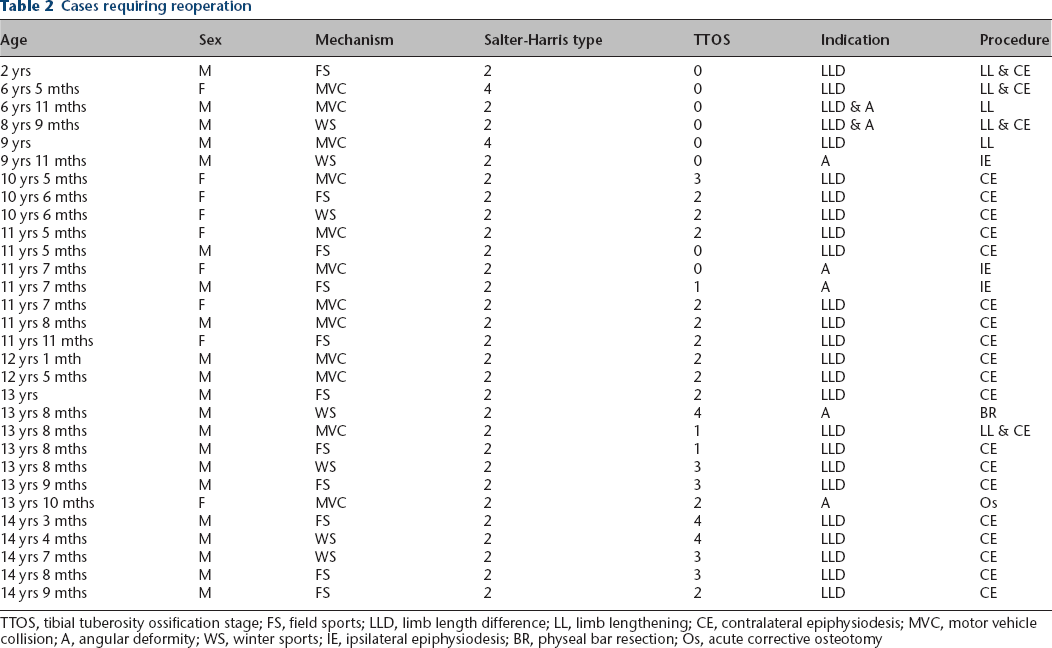
TTOS, tibial tuberosity ossification stage; FS, field sports; LLD, limb length difference; LL, limb lengthening; CE, contralateral epiphysiodesis; MVC, motor vehicle collision; A, angular deformity; WS, winter sports; IE, ipsilateral epiphysiodesis; BR, physeal bar resection; Os, acute corrective osteotomy
Inter-rater reliability of TTOS between the two independent blinded reviewers was calculated via kappa test. This gives a kappa coefficient of 88.4 (the expected random agreement of 27% versus actual agreement of 91%) indicating a high degree of inter-rater reliability.
The proportions of patients who required further surgical intervention due to growth disturbance grouped by TTOS are shown in Figure 2. The relationship between reoperation and TTOS was investigated using the R statistical analysis package (R Core team, A Language and Environment for Statistical Computing, Vienna, Austria). Chi-squared testing with four degrees of freedom indicated that TTOS was significantly related to need for further surgery (p < 0.001). When reoperation for limb-length difference and angular deformity were considered separately, significant relationships between both surgical indications and TTOS were established (p = 0.0047 and 0.0028, respectively).
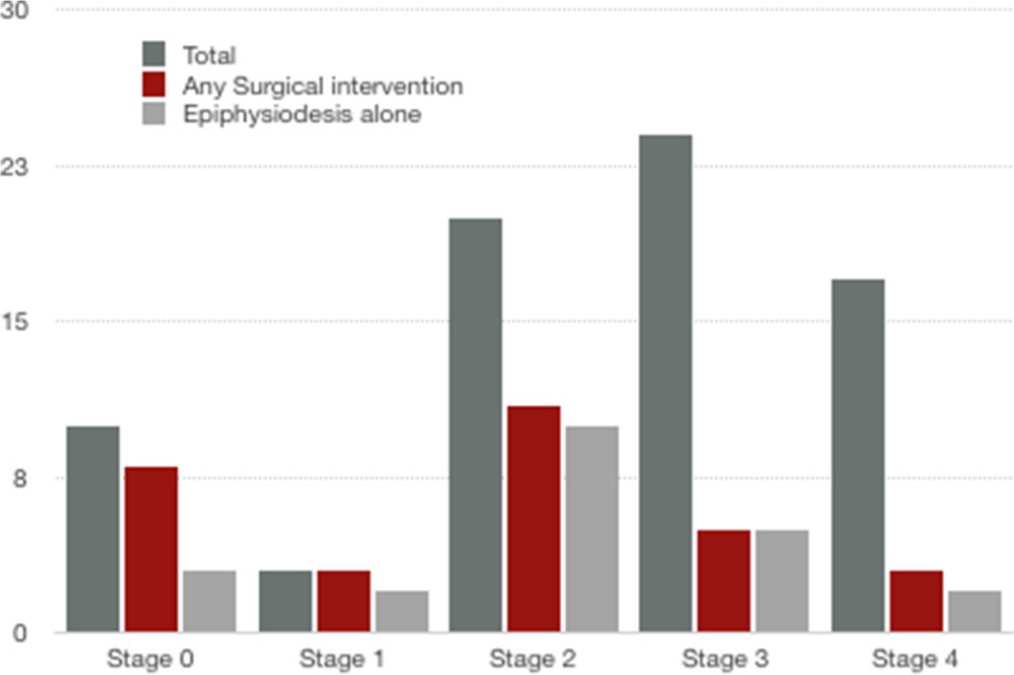
Surgical intervention for growth disturbance done in follow-up by Tibial Tuberosity Ossification Stages 0 to 4.
Logistic regression analysis showed the odds of receiving any further surgery if TTOS is 3 or 4 (tuberosity fused to metaphysis), compared with 0 to 2 (tuberosity not fused to metaphysis) was 0.12 (95% confidence interval (CI) 0.04 to 0.34). Unless otherwise stated, a second operation was 8.3-times more likely for the immature (TTOS 0 to 2) children. The estimate of the effect of TTOS on reoperation rates did not vary when adjusted for sex, mechanism and Salter-Harris type. When accounting for age, the odds of any further operation when TTOS is 3 or 4 at initial injury (compared with 0 to 2) is 0.28 (95% CI 0.08 to 0.94). This demonstrates that TTOS at injury remains a significant, independent predictor even when the odds of secondary surgery are dropping because of age. An extra year of age reduced the odds of surgery to 0.40 compared with a patient a year younger.
In all, 19 surgical interventions were performed on children where TTOS was 2 or greater. Only two of these 19 children required intervention more extensive than percutaneous epiphysiodesis.
Discussion
This report represents the largest published single centre series of operatively treated distal femoral physeal fractures. Previous studies have associated age at injury, fracture displacement, Salter-Harris type, operative fixation and mechanism of injury with growth disturbance in distal femoral physeal fractures,1–3,11 but they have been unable to quantify the relative risk associated with the above variables due to small diverse patient cohorts. This report is the first study to establish the relationship between TTOS and the need for further surgery to treat either angular deformity or limb length inequality. By classifying fractures by TTOS at time of injury, we have been able to quantify the relative odds of further surgery to treat growth arrest.
TTOS represents a local estimation of maturity and residual growth potential. While the concept of using a local growth potential surrogate to predict outcome in distal femoral fractures is novel, the principle of using local estimators of residual growth to guide treatment in paediatric orthopaedics is commonplace. The Risser staging of iliac wing and tri-radiate cartilage ossification are well accepted in the treatment of spinal deformity.12,13 Similarly, fusion of the tri-radiate cartilage and Oxford pelvic bone age have been used to estimate the risk of contralateral slip in slipped capital femoral epiphysis.14,15
The distal femoral growth plate grows at an average of up to 1.3 cm per year and provides the majority of longitudinal femoral growth. 16 This rapid local growth leaves patients with distal femoral physeal injuries particularly susceptible to significant growth disturbance. Fusion of the posterior aspect of the tibial tuberosity to the metaphysis does not protect the child from developing a growth arrest but rather indicates that there is likely not enough remaining growth for a clinically relevant deformity to occur.
Reoperation as an outcome measure is well accepted in broad range orthopaedic pathology.17,18 However, a potential weakness of all reports including this study that base outcomes on need for surgery is that thresholds for surgical intervention vary between clinicians, institutions and patient populations. This variability may mean that outcomes based on need for further surgery can be less transferable to the practice of others. We feel that our conclusions are broadly applicable, as our incidence of further surgical intervention closely matches the published reoperation rates from other institutions.1–3,11
A further limitation of this report is its retrospective nature. All studies of this type are inherently subject to selection bias. We have only investigated the outcomes of patients who have had operative treatment. It is reasonable to assume that the group of operatively treated patients represents the more severe fractures. Our conclusions may, therefore, be invalid for less severe injuries that do not require operative intervention. A prospective study relating TTOS to the need for surgery to address deformity following all distal femoral physeal fractures is required to overcome this limitation. To our knowledge there are no prospective studies investigating the outcomes of paediatric distal femoral fractures. This deficit represents an opportunity for further research.
TTOS can be easily defined on the plain radiographs used in the initial assessment of paediatric distal femoral fractures. TTOS provides a local estimation of bone age and thus potential for further growth at the distal femoral physis. The proportion of patients with growth plate fractures to the distal femur requiring further surgery to treat both angular deformity and limb-length inequality is significantly linked to TTOS. TTOS at injury remains a significant, independent predictor even when the odds of secondary surgery are dropping because of age. In patients where the secondary ossification centre of the tibial tuberosity is not fused to the metaphysis, further surgery to treat a growth disturbance is probable. Whereas, if the secondary ossification centre of the tibial tuberosity is fused with the metaphysis, future surgery to treat a growth disturbance is unlikely. In cases where the ossification of the proximal tibia has progressed beyond fusion of the ossification centre in the epiphysis to the ossification centre in the tibial tuberosity, intervention more extensive than percutaneous epiphysiodesis to halt progression of deformity is unlikely to be required. This knowledge will provide guidance useful in the consent, education and follow-up of patients and families.
Footnotes
DW: Manuscript preparation.
MC: Study design, Manuscript preparation.
AH: Study design, Data acquisition, Manuscript preparation, Statistical analysis.