
Abstract
Abstract
Background
Tibial tubercle fractures often occur in athletic adolescents close to skeletal maturity. These fractures can present with marked displacement of the apophysis, intra-articular extension, and associated soft tissue injuries, such as tibial meniscal ligament tears. Here, we present our surgical technique which focuses on recreating the meniscal–articular relationship (using suture anchors) in severely displaced fractures.
Methods
We retrospectively reviewed all tibial tuberosity fractures treated with this technique over the last 2.5 years. Fractures with a minimum of a 12-month follow-up post-fixation were identified. Clinical records and radiographs were reviewed. Data included patient age, gender, involved side, injury classification (modified Ogden), mechanism of injury, treatment, return to activity, and complications.
Results
Six patients met the inclusion criteria. Mean age at time of surgery was 14.9 (range 13.2–16.8) years. All patients were male and the mean follow-up period was 14 (12–26) months. Range of motion was started at 4 weeks post-operatively in a hinged knee brace, and return to sports occurred at an average of 3.75 months postoperatively (range 3–5 months). No evidence of growth disturbance of the proximal tibia or recurvatum at final follow-up was evident.
Conclusion
We speculate that patients who sustain a tibial tubercle avulsion fracture types III or V will likely have intra-articular pathology, specifically capsular avulsion or coronary ligament disruption. By utilizing suture anchors, our technique emphasizes renewing the anatomic articular environment to ensure better long-term results and maintaining these active individuals in sports.
Keywords
Introduction
In the pediatric population, tibial tubercle fractures are uncommon. These fractures account for approximately 3% of all proximal tibial fractures and for less than 1% of all physeal fractures [1–4]. The incidence compared to all epiphyseal fractures has been reported to be 0.4–2.7% [1, 2, 5, 6]. Tibial tubercle fractures often occur in athletic adolescents approaching physeal closure who have strong quadriceps muscles that lead to avulsion following eccentric contraction [7, 8]. These fractures can present with marked displacement of the apophysis, intra-articular extension, and associated soft tissue injuries [1, 5, 9–13]. Meniscal damage along with disruption of the patellar tendon can occur in tibial tubercle fractures that are markedly displaced [1, 5, 9–14]. We present our surgical technique with specific tips that allows for stable fixation as well as re-creation of the meniscal–articular relationship in these severely displaced fractures. We also present results in our small series of patients treated with this technique.
More than 80% of fractures involving the tibial tuberosity occur between the ages of 15–17 years [5, 7, 12, 17, 18]. During skeletal maturity the tibial tubercle changes and can be vulnerable during extreme traction situations, such as powerful jumping [16]. Two possible mechanisms of injury have been described: (1) violent knee flexion against a contracting quadriceps, as in landing from a jump [3–5, 8], or (2) a powerful contraction by the quadriceps against a fixed foot, as in jumping [5]. As such, basketball and high jump are the sports most often associated with this injury, although others have been reported, such as football, gymnastics, walking, diving and springboard [2, 3, 5, 6, 12, 15].
Classification
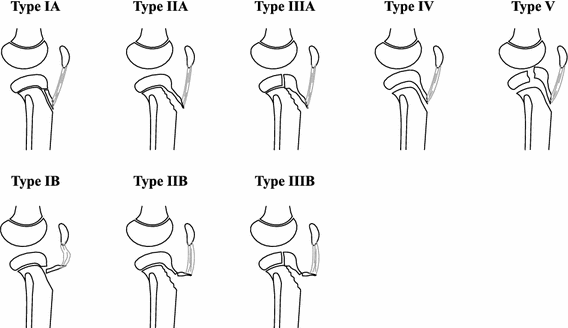
The classification of tibial tubercle fractures has evolved over the years. All classification schemes are based on the original Watson–Jones classification [8]. Type I is an avulsion of the small part of the tibial tubercle. Type II extends across the physis but does not enter the joint. Type III is similar to Type II, but an extension of the fracture occurs and enters the joint [8]. Ogden added A and B to each of the types to indicate displacement and comminution, respectively [12]. Type C was added later by Frankl et al. [19] for associated patellar ligament avulsions, originally described in two cases. Ryu et al. [20] added a Type IV, which is complete tibial epiphysis involvement. Finally, Type V was described by Mckoy et al. [3] as a Type IIB with an associated Type IV fracture that created a ‘Y’ fracture configuration (Fig. 1).
Treatment
The treatment of tibial tubercle fractures in skeletally immature patients depends on the type of injury. For non-displaced fractures, a 6-week course of non-weight bearing immobilization should be sufficient. However, displaced fractures need to be reduced and stabilized surgically, with the goal of restoring the extensor mechanism and the joint surface with all its associated components [5, 7, 12, 17, 21]. Open reduction with internal fixation typically involves fixation with implants that can achieve compression at the fracture site (most often screws and washers). Arthroscopic-assisted open fixation has been used. This technique can be helpful in variants with intra-articular extension to evaluate the joint line as well as any associated meniscal or osteochondral injuries [5, 10] and requires additional setup and equipment. We present a technique that in addition to anatomic fracture fixation can help re-create the meniscal articular relationship by repairing the coronary ligaments.
Surgical technique
After appropriate anesthesia, the patient is placed on a radiolucent table in the supine position with a non-sterile tourniquet as high on the affected leg as possible. It is important to pull down the quadriceps mechanism (with the help of one assistant) when placing the tourniquet to prevent the impaling of the quadriceps muscle mass while the tourniquet is insufflated. An assistant can help hold the patella articulated with the distal femur and gently flex the knee to assist in the process while applying and later insufflating the tourniquet. The leg is prepped and draped according to standard orthopedic protocol. The extremity may be exsanguinated with an Esmarch prior to inflation of the tourniquet or held elevated for 4–6 min (Lister's maneuver) [22].
A radiolucent triangle (small/medium) may be utilized for positioning the knee during surgical approach and fixation of fracture. A longitudinal, anterior midline incision is made on the knee from the distal pole of the patella to 2 cm past the previous original insertion position of the tibial tubercle. Deep flaps on either side of the fragment are developed to allow for exposure of the coronary ligament and menisci from within the fracture site. A small para-patellar arthrotomy is created to better visualize the menisci. Typically, the periosteum and deep fascia are torn, which will require repair later, but allows for improved visualization into the joint. Arthroscopic assistance may be utilized for both inspection of damage as well as subsequent confirmation of anatomic articular reduction. The fracture hematoma is irrigated and the fracture bed cleared of debris (i.e., periosteum). A specific bleeder (likely the anterior recurrent tibial branch) is carefully looked for and, if so, thermo-coagulated or ligated.
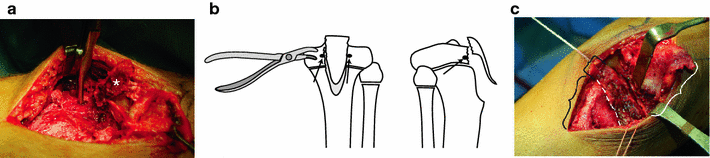
Following irrigation, both the medial and lateral menisci should be identified along with the coronary ligaments. The coronary ligaments are often disrupted and must be repaired. A small rongeur should be used to clear a space for two bio-absorbable suture anchors to be placed just above the growth plate and on either side of the fracture bed, making sure not to obstruct the reduction (Fig. 2). Care must be taken not to disrupt the physis (with a transphyseal suture-anchor) or to penetrate the articular surface with the suture anchor. Prior to reduction of the tibial tubercle piece(s), a portion of the coronary ligament is grasped with the superior arms of the suture. Reduction of the fractured fragment is then performed with the knee in extension. This can be facilitated by moving the radiolucent triangle towards the ankle allowing for full knee extension. A ball-spike pusher or a threaded guidewire is utilized to maintain the reduction, and fluoroscopy confirms the reduction. Arthroscopic camera assistance can also help in this step when available. Additional guidewires are placed parallel through the fracture fragments in either the metaphysis or epiphysis. Appropriately sized screws are used depending on the fragment size; 4.5-mm screws are typically used for smaller fragments and 6.5-mm screws can be used for larger fragments. We typically use a 4.5-mm cannulated screw. After confirming the appropriate trajectory and length of the guidewire with fluoroscopy, a 3.2-mm cannulated drill bit is used to enter the most anterior piece of the tubercle fracture fragment. A 4.5-mm partially threaded, cannulated screw with or without a washer is then inserted (Fig. 3).

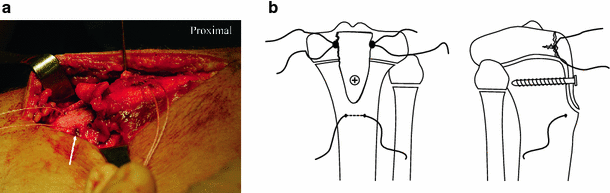
With the tubercle fragment(s) now in place, the sutures attached to the coronary ligament are tied with the needles left on the ends. Both the superior and inferior sutures are brought through the patellar tendon and tied over the more proximal screw. The suture anchors play two roles: (1) maintaining the meniscal–articular relationship and (2) providing additional fixation for smaller fragments. Finally, a drill hole is made into the distal tibia in order to pass an 0-vicryl suture through the tibia, and a modified Krakow-type suturing pattern is then used to tie down the remaining tissue (Fig. 4).
The arthrotomy and retinaculum are repaired with a non-absorbable suture, and the torn periosteum is re-approximated to further supplement the fracture fixation. The skin is closed to the surgeon's preference, and the patient should be admitted to the hospital for compartment checks and pain control.
The post-operative care plan varies based on fracture classification but generally includes a long leg cast in full extension for 4 weeks. The patient is limited to toe-touch weight-bearing on the affected leg for 4 weeks. After cast removal, all patients are prescribed physical therapy and are placed in a hinged knee immobilizer for 4–6 more weeks to work on a range of motion exercises and achieve progress in weight-bearing status as tolerated. Return to sport is allowed as early as 3 months if the following criteria are met: full, painless knee range of motion, quadriceps strength >90% on contra-lateral side, single-leg forward hop test of >80% of contralateral side, and medical clearance from physical therapy.
Data in our series of patients treated with this technique: Methods
After approval of the Institutional Review Board, we retrospectively reviewed all tibial tuberosity fractures treated with this technique by the senior author (HH) over the last 2.5 years. Fractures with a minimum of a 12-month follow-up post-fixation were identified. Clinical records and radiographs were reviewed. Data were collected to include patient age, gender, involved side, injury classification (modified Ogden), mechanism of injury, treatment, return to activity, and complications. The data are presented (Table 1).
Patients with tibial tubercle fractures treated with supplemental suture anchors
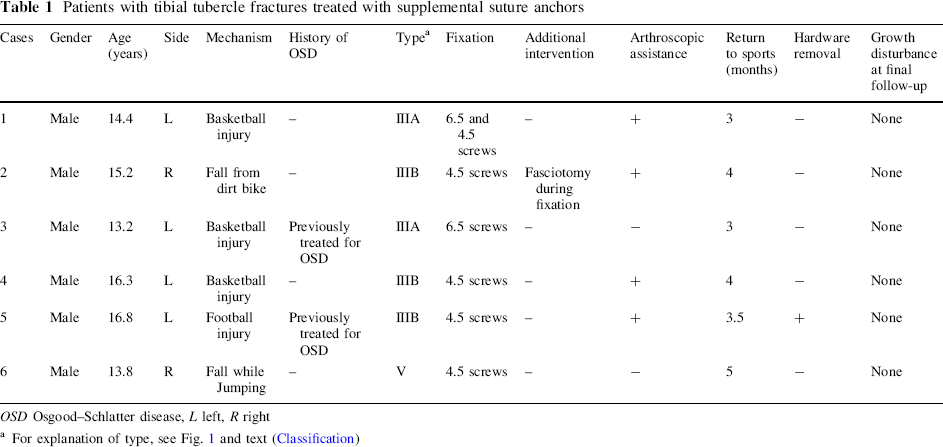
OSD Osgood–Schlatter disease, L left, R right
For explanation of type, see Fig. 1 and text (Classification)
Results
There were six patients who met all of the above criteria. Mean age at time of surgery was 14.9 (range 13.2–16.8) years. All patients were male, and there were four left-sided injuries and two right-sided injuries. The mean follow-up period was 14 (12–26) months. Three patients had injuries from basketball, one from football, one from a dirt bike injury, and one from a fall while jumping.
Given our inclusion criteria and using the modified Ogden classification, we found two patients with Type IIIA fractures, three Type IIIB, and one Type V. All of these patients had surgical intervention with screw fixation (with or without washers) and supplemental suture anchor fixation. They were all placed into a long leg cast for 4 weeks with partial weight-bearing. None of these patients had clinical symptoms of compartment syndrome, although one patient received a prophylactic fasciotomy during surgery due to the extent of hematoma noticed intra-operatively. One patient required hardware removal secondary to prominence of the screw heads.
Range of motion was started at 4 weeks post-operatively in a hinged knee brace, and return to sports occurred at an average of 3.75 months postoperatively (range 3–5 months) (Table 1). All patients participated in physical therapy once out of the cast, and only one patient required additional therapy for quadriceps weakness after 8 weeks of physical therapy. No evidence of growth disturbance of the proximal tibia or recurvatum at final follow-up was evident.
Discussion
Tibial tuberosity fractures most often occur in the young male population in more than a 10:1 male to female ratio. Fewer than ten female tibial tuberosity fractures have been reported in the English literature [5, 7, 12, 17]. The strong predominance towards males with this injury is believed to result from the later age in which males experience physiologic epiphysiodesis of the proximal tibia [3, 5]. This leads to higher traction stresses on the tibial tubercle as males become larger and heavier, with stronger quadriceps [5]. In addition, the tibial apophysis is more vulnerable due to the change in histology occurring during this age range of 13–16 years [18].
Tibial tubercle fractures predominantly occur in active patients who likely expect to have many more years of athletic activities ahead of them. The powerful extensor mechanism is usually injured as part of its attachment is torn from the periosteum just below the tibial tubercle fragments. In order to return these patients to their previous high level of physical activity, it is imperative to restore the extensor mechanism, restore the articular cartilage surface, and re-establish the meniscal anatomy (repair the coronary ligaments) [5, 12, 17].
Our current technique addresses each point. First, the extensor mechanism is restored with the combination of reducing the bony fragments, but also with the suture repair from the anchors and the free suture passed through the anterior tibia. Second, by visualizing the menisci through the fracture site, one is able to assess blocks in reduction as well as articular step-offs. Third, by grasping the coronary ligament, one is able to maintain the meniscal–articular relationship that may have been disrupted secondary to the intra-articular fracture. The suture anchor method can also be applied to Ogden Type IIB fractures to further supplement fixation into the periosteum and smaller fragments.
Although many complications have been reported and can occur within the first year post-surgery (compartment syndrome, malunion, non-union, patella baja, and fracture through internal fixation, and genu recurvatum) [1, 3–5, 7, 12, 17], it is rare to see these sequelae given the near-skeletal maturity of these patients. We do believe that the use of suture anchors may allow smaller screws to be used, which may cause less irritation, a well-known complication usually requiring screw removal.
We speculate that patients who sustain a tibial tubercle avulsion fracture Types III or V will likely have intra-articular pathology, specifically capsular avulsion or coronary ligament disruption and less commonly meniscal tears. These injuries must be addressed to ensure the patient will have a good outcome later in life and prevent premature osteoarthritis. Our technique emphasizes renewing the anatomic articular environment to ensure better long-term results and maintaining these active individuals in sports.