
Abstract
Abstract
Purpose
Type 6 is an open fracture in which part of the physis is missing. It is the least common physeal fracture, but has the highest rate of complications, particularly the formation of a physeal bar. Without preemptive treatment, a physeal bar always forms, producing growth retardation and angular deformity, and excision of these physeal bars has been uniformly unsuccessful. The distal medial malleolus is a common site for the fracture.
Methods
Strategies for the treatment of two varieties of acute medial malleolar type-6 fractures and two types of late deformities following type-6 fracture are given. The acute fractures were treated with either fat or cartilage applied to the exposed physis. The late deformities were treated with corrective iliac bone grafting.
Results
The acute fractures were prevented from forming physeal bars and the two late deformities were fully corrected with good outcomes.
Conclusion
Fat applied to an acute type-6 physeal fracture has a good chance of preventing bar formation. Ankle deformities due to bars can be corrected by means of iliac bone grafting.
Keywords
Introduction
Type 6 is a fracture in which part of the physis is missing [1–3]. Usually, an accompanying part of the epiphysis or metaphysis, or both, is also missing. This is a result of an open fracture, caused by such things as a lawn mower, grain auger, motorboat propeller, motorized traffic accident, etc. It is the least common physeal fracture, but has the highest rate of complications, particularly the formation of a physeal bar [2, 3]. Without preemptive treatment, a physeal bar always forms—producing angular deformity and growth retardation—and their excision in these cases has been uniformly unsuccessful [2, 3]. The distal tibial medial malleolus is a common site for this fracture; we suggest strategies for the treatment of the distal tibial medial malleolus acute type-6 fracture and its otherwise inevitable physeal bar [3].
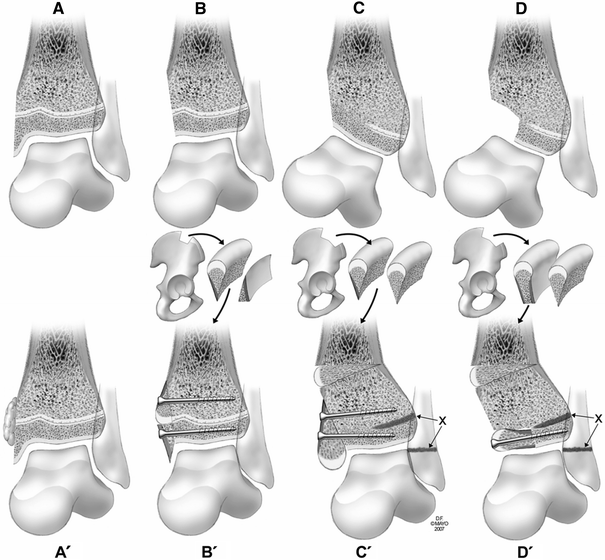
Part A. Acute care for loss of a superficial portion of the medial malleolus: Talar stability maintained
When there is loss of the superficial portion of the medial malleolus (Fig. 1a), the physis is exposed, predisposing it to premature arrest. Ankle joint integrity and stability are maintained. In this instance, application of fat against the physis at the time of initial repair (Fig. 1a′) may prevent bar formation temporarily or indefinitely. The fat could be on a flap transfer [4] (free or pedicle) or free fat (vascularized or nonvascularized), depending on the nature of the wound. In a thin person, there may be a paucity of fat within the injured area. In this instance, fat may be taken from a small incision in the buttock crease. This strategy was successful in maintaining growth without bar formation in one case performed immediately and unsuccessful in another performed 10 months post-injury [4].
Loss of medial malleolus.
Part B. Acute care of loss of the entire medial malleolus: Talar stability questionable
Loss of the entire medial malleolus (Fig. 1b) predisposes the exposed physis to premature arrest and the talus to instability. In such a case, reconstruction of the medial malleolus with the goal of maintaining growth may be attempted by substituting the missing physis with iliac apophyseal cartilage (Fig. 1b′). A block of iliac crest bone is divided obliquely and the apophyseal cartilage is placed adjacent to the physis. The second piece, without cartilage, is used to reconstruct the missing medial malleolus. Both parts of the iliac crest block are attached with their cancellous surfaces facing the tibia with screws. The bone graft is covered with free soft tissue graft. One successful case performed 12 days post-injury has been reported [5].
Utilization of the strategies presented in Fig. 1a′ and b′ will depend on the nature and severity of the bone and soft tissue loss. Ideally, there would need to be immediate soft tissue coverage without concern for infection.
Part C. Late care of absence of the medial malleolus with medial physeal bar
Complete absence of the medial malleolus resulting in a medial physeal bar causes varus angulation (Fig. 1c) and predisposes to talar instability and degenerative arthrosis. This can be treated by inserting a piece of iliac crest longitudinally, using the apophysis for the tip of the malleolus, combined with closure of the physes of the distal fibula and lateral tibia, and corrective tibial osteotomy when appropriate (Figs. 1c′, 2)

An 11-year and 9-month-old boy was struck and dragged by a car, sustaining a distal tibial medial malleolar type-6 physeal fracture with extensive soft tissue loss. The anterior medial part of the distal tibia (the entire medial malleolus) was missing. Treatment consisted of debridement and free flap soft tissue graft.
Part D. Late care of absence of the medial malleolus plus part of the distal medial epiphysis
Loss of the medial malleolus plus part of the medial epiphysis resulting in a medial physeal bar causes varus angulation (Fig. 1d), predisposes to talar instability, and ensures rapid degenerative arthrosis. It can be managed by inserting iliac crest block graft transversely into the defect (Fig. 1d′), combined with arrest of the distal fibular and lateral tibial physes and corrective tibial osteotomy (Fig. 3). The concave contour on the inner side of the iliac crest is nearly congruent with the sagittal convexity of the dome of the talus.

A 9-year 9-month-old boy sustained a distal tibial type-6 physeal fracture and extensive soft tissue loss of the left ankle in a farm auger injury.
Osteotomy and graft preparation
In cases with substantial medial malleolar defects and physeal bars, as noted in Figs. 1c, d, 2, and 3, staging of the osteotomy for angular correction and of the malleolar reconstruction will depend on the degree of the deformity and the particulars of the soft tissue coverage. Open-wedge osteotomy using a wedge of iliac crest bone [6] corrects the deformity, adds a little length and, if done concurrently with repair of the malleolus, the same iliac donor site can be used for both grafts (Figs. 1c′, d′, 3). Preparation of the iliac crest graft defects, depicted in Fig. 1b′, c′, and d′, requires contouring by means of an osteotome or a motorized bur, excoriating or removing cortical bone, so that the graft fits the defect snuggly and cancellous bone opposes the recipient bone. Any remaining cortical bone opposing the recipient bone may be punctured multiple times with a small drill bit to enhance blood flow into the graft to facilitate bone union.
Prognosis
All patients with type-6 fracture of the medial malleolus, regardless of initial outcome, are prone to develop degenerative arthrosis and should be cautioned against excessive weight gain and activities detrimental to the ankle.