
Abstract
Abstract
Purpose
The purpose of this study was to explore whether increasing the hip abduction angle would increase the incidence of avascular necrosis (AVN) in patients with late- detected developmental dysplasia of the hip (DDH) treated by closed reduction (CR) and spica cast immobilization.
Methods
A total of 55 patients (59 hips) with late-detected DDH underwent MRI after CR. Hip abduction angle and hip joint distance were measured on postoperative MRI transverse sections. The acetabular index and centre-edge angle were measured on plain radiographs at the last follow-up. The presence of AVN according to Kalamchi and McEwen's classification was assessed. We retrospectively analyzed the associations among abduction angles, hip joint distances, radiographic parameters, AVN and final outcomes, exploring the relationship between hip joint abduction angle and AVN rate.
Results
The mean age at the time of CR was 14.4 months SD 5.5 (6 to 28), and the mean follow-up was 26.2 months SD 8.1 (12.4 to 41.7). The mean hip abduction angle was 70.2° SD 7.2° (53° to 85°) on the dislocated side and 63.7° SD 8.8° (40° to 82°) on the normal side; the mean hip joint distance was 5.1 mm SD 1.9 (1.3 to 9.1) on the dislocated side and 2.2 mm SD 0.6 on the normal side (1.3 to 3.3). Eight of 59 hips (13.6%) developed AVN. Neither the amount of abduction nor hip joint distance increased the AVN rate (p = 0.97 and p = 0.65, respectively) or the dislocation rate (p = 0.38 and p = 0.14, respectively).
Conclusion
Abduction angle up to 70.2° following CR did not increase the AVN rate in children aged six to 28 months with late-detected DDH treated by CR.
Level of evidence
III.
Keywords
Introduction
At present, closed reduction (CR) and spica cast immobilization under general anaesthesia is the preferred method of treatment in patients with developmental dysplasia of the hip (DDH) aged six to 24 months,1,2 although many practitioners are evolving toward open reduction and pelvic osteotomy as a standard approach after 18 months of age. 3 The aim of treatment is to obtain a stable reduction of the hip while limiting the risk of avascular necrosis (AVN) of the femoral epiphysis.
AVN is one of the most serious complication following CR, with reported rates ranging from 0% to 73%.4–8 Previous studies identified several risk factors for AVN in DDH patients undergoing CR. In particular, increased hip abduction angle, age at reduction, delayed appearance of the ossific nucleus and adductor tenotomy at the time of CR have been reported as potential risk factors.4–12 Despite these findings, the exact aetiology of AVN remains unknown.
To decrease the risk of AVN, it is currently accepted that DDH patients undergoing CR should be immobilized with hip abduction not exceeding 55° to 60°. In 1976, Ramsey et al 13 introduced the concept of the ‘safe zone’. Specifically, the hip should be placed within a ‘safe zone’ in order to decrease both the risk of redislocation (if abduction was not enough) and AVN (if abduction was too much). The so-called ‘Ramsey safe zone’ is between 35° to 40° and 55° to 60° of hip abduction. Nevertheless, there is a paucity of scientific literature, with conflicting results, investigating the correlation between the amount of hip abduction and AVN rates in DDH patients treated by CR. Moreover, this lack of studies has not been corrected with the advent of more sophisticated imaging studies such as MRI.14,15
Dibello et al 14 reported that the degree of hip abduction should be < 70° in order to maintain hip reduction and to preserve femoral head perfusion, thus decreasing the risk of AVN. 14 However, Schur et al 15 found no significant association between hip abduction and AVN in DDH patients older than six months of age at the time of CR.
The aim of our study was to investigate whether hip abduction angle exceeding the ‘Ramsey safe zone’ upper limit correlated with the AVN rate and to explore the potential limits of acceptable degrees of abduction. The hypothesis was that increased abduction would not necessarily correlate with the increased rate of AVN in children with DDH undergoing CR and spica cast immobilization.
Materials and methods
After institutional review board approval, a retrospective review of children aged six to 28 months with late-detected DDH was performed.
The medical records of 71 consecutive patients with late-detected DDH treated by CR and spica cast immobilization during the period January 2015 to December 2016 were retrospectively reviewed.
Inclusion criteria were as follows: 1) diagnosis of DDH; 2) initial treatment by CR and spica cast immobilization; 3) more than six months and < 30 months of age at the time of index procedure; 4) postoperative MRI; 5) complete clinical and radiographic data; and 6) at least 12 months of clinical and radiographic follow-up. Exclusion criteria were as follows: 1) concomitant diagnosis of cerebral palsy, myelomeningocele, tethered cord syndrome, arthrogryposis multiplex congenita or other neuromuscular disorders; 2) follow-up < 12 months; 3) postoperative MRI not available; and 4) incomplete clinical and radiographic data.
A total of 55 patients (50 girls, five boys; 59 hips) met the inclusion criteria; the remaining 16 patients were excluded due to incomplete clinical and radiographic data, including follow-up < 12 months (nine patients; 13.6%), concomitant diagnosis of arthrogryposis multiplex congenita (five patients; 7.6%) and cerebral palsy (two patients; 3%).
All patients underwent CR under general anaesthesia. Adductor tenotomy was performed if the adductor was thought to hinder the reduction. Arthrography was performed through an adductor longus muscle approach using 1 ml of Iopromide as contrast agent to evaluate the position of the hip and to assist in the reduction.
After CR, a spica cast with the hips abducted and flexed (90°, at least) was applied for three months to maintain reduction and was changed at six weeks. After cast removal, patients were placed in an abduction brace for six additional months (three months full-time and three months night-time only).
MRI measurements
Following CR and spica cast immobilization, MRI examination was obtained to confirm the reduction. MRI examination was performed using a 1.5T Philips Gyroscan Achieva MRI system (Philips, Best, The Netherlands) with the standard examination including the whole pelvis and the proximal femur with axial, sagittal and coronal plane sequences. The MRI examination was carried out under sedation with the patients placed supine, legs immobilized in the spica cast and with body array coils placed anteriorly and posteriorly to the pelvis. The sequences included T1-weighted spin-echo images in the coronal and sagittal planes, T2-weighted (T2-W) fast field-echo in coronal and sagittal planes and T2-W spectral presaturation attenuated inversion recovery (SPAIR) in coronal and sagittal planes.
Using standard Picture Archiving and Communication Systems (PACS) software hip abduction angle and hip joint distance were measured on the transverse section of the best reduced MRI postoperative image (T2-W-SPAIR) (Fig. 1).
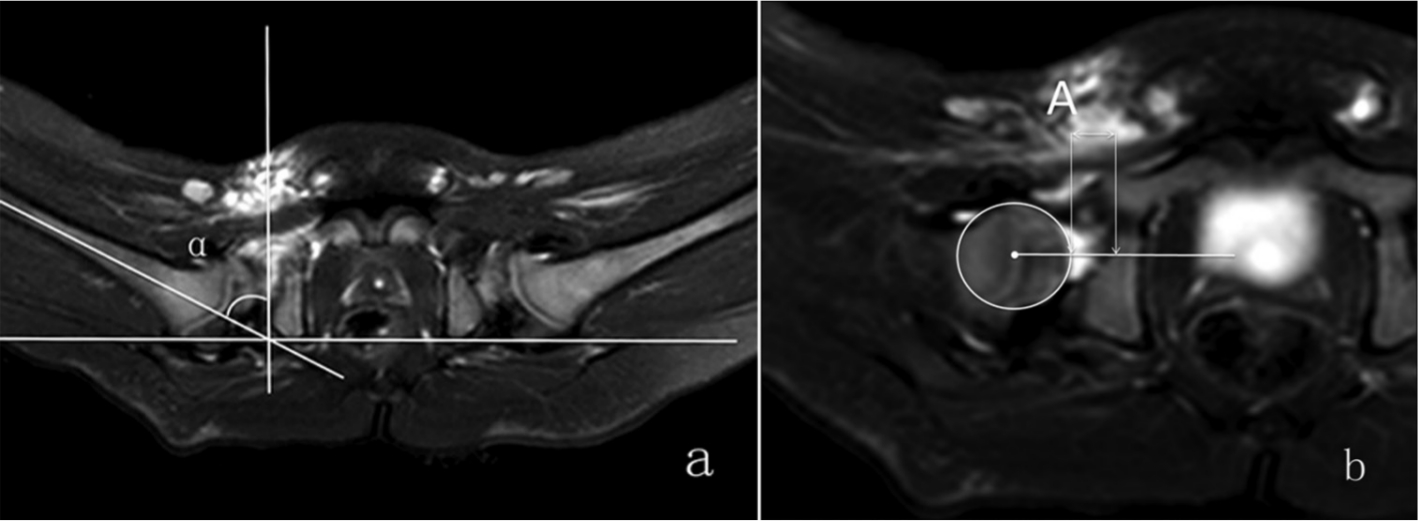
Abduction angle and hip joint distance (HJD) and were measured on transverse plane of magnetic resonance imaging (T2-weighted spectral presaturation attenuated inversion recovery) performed after closed reduction: (a) abduction angle is the angle between the perpendicular to a line connecting the posterior ischial tuberosities and the femoral shaft axis (α angle); (b) HJD is the distance, in mm, between the femoral head and the acetabular socket according to Gans and Sankar 17 (length A).
Hip abduction angle was the angle between the axis of the femoral shaft and the horizontal line tangent to ischial tuberosity, bilaterally. 16 Values were expressed in degrees.
Hip joint distance was measured as the distance between the femoral head and the acetabular socket according to Gans and Sakar 17 (Fig. 1). Values were expressed in millimetres.
Each rater assessed MRI images twice at one-week intervals. The kappa coefficient for correlated data were calculated in order to measure the inter-observer reliability at the first rating and intra-observer reliability between first and second ratings. According to the usual recommendations the concordance was examined as follows: < 0.2 (bad), 0.2 to 0.4 (low), 0.4 to 0.6 (moderate), 0.6 to 0.8 (good) and > 0.8 (excellent).
Radiographic measurements
All patients were followed for at least 12 months (12.4 to 41.7) after cast removal, and anteroposterior (AP) pelvis radiographs in neutral and frog-leg positions were obtained at each follow-up visit.
Preoperatively, all hip dislocations were evaluated on plain AP radiographs of the pelvis according to the method described by Tönnis. 18
Postoperatively, the acetabular index and the centre-edge angle were measured in all patients on AP pelvis radiographs. AVN of the femoral epiphysis was identified using the criteria described by Salter et al 19 and was graded according to Kalamchi and McEwen's classification. 20 With type I AVN, changes are limited to the femoral head, and the metaphysis is not involved, therefore, type I AVN is thought to represent transient ischaemia of the femoral head that can recover completely. Therefore, we grouped type I AVN with the normal hip category.
AP and frog-leg radiographs were assessed to evaluate the primary outcome measures, namely, AVN of the femoral epiphysis. Two trained pediatric orthopaedic surgeons (LY, FC) assessed all radiographs independently. In case of disagreement, radiographs were shown to a pediatric radiologist (Liu Hongsheng) to make the definitive diagnosis.
Statistical analysis
Statistical analysis was performed using Stata software, version 13 (StataCorp, College Station, Texas). The tests were two-sided, with a type I error set at α = 0.05. Continuous data were presented as the mean and sd or the median and interquartile range according to statistical distribution (assumption of normality checked using normal probability plots and the Shapiro-Wilk's test). The relationships between continuous parameters were studied using correlation coefficients (Pearson or Spearman, depending on statistical distribution), in addition to random-effects models. A multivariate logistic model was used to determine whether factors were independently associated with risk of AVN.
Results
Among the 55 included patients (59 hips), there were 51 unilateral (92.7%) and four bilateral (7.3%) hip dislocations. The mean age at the time of CR was 14.4 months sd 5.5 (6 to 28) and the mean follow-up was 26.2 months sd 8.1 (12.4 to 41.7) (Figs 2 and 3).
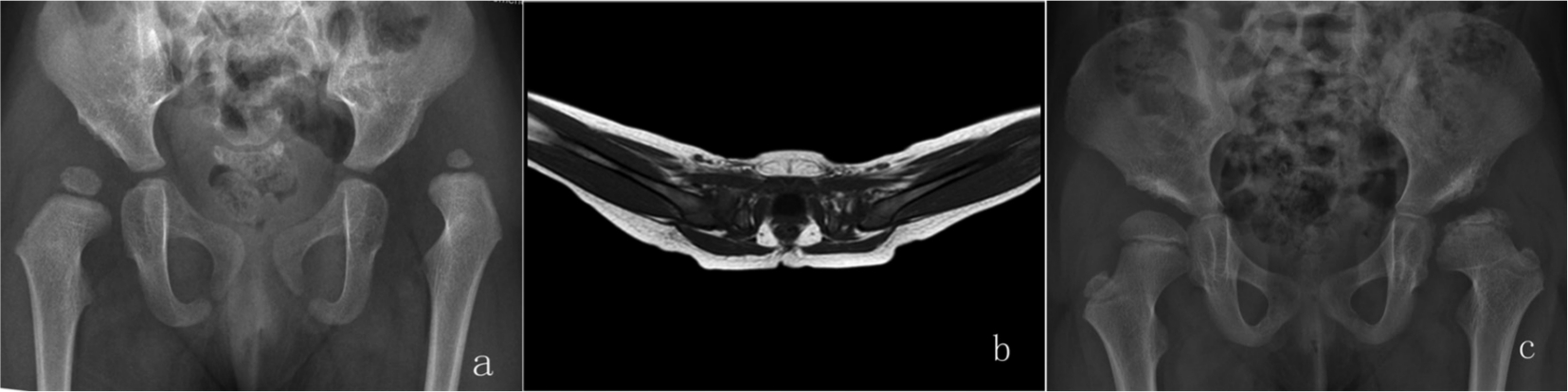
(a) A 19-month-old girl with left developmental dysplasia of the hip, Tönnis grade 3. (b) Spica cast immobilization with 61° of abduction. (c) Radiographs at 22-month follow-up show evidence of type III avascular necrosis.
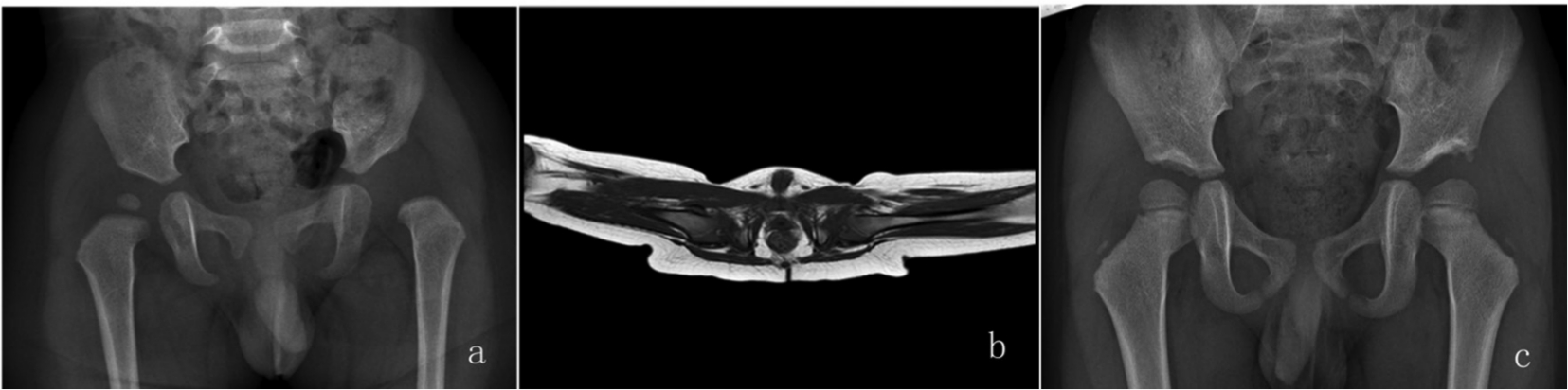
(a) A 12-month-old boy with left developmental dysplasia of the hip, Tönnis grade 2. (b) Spica cast immobilization with 85° of abduction. (c) Radiographs at 39-month follow-up show hips concentrically reduced.
Table 1 shows demographics of patients and final clinical and radiographic outcomes. AVN of the femoral head was detected in eight of 59 dislocated hips (13.6%) (Table 1).
Demographic of patients in this cohort
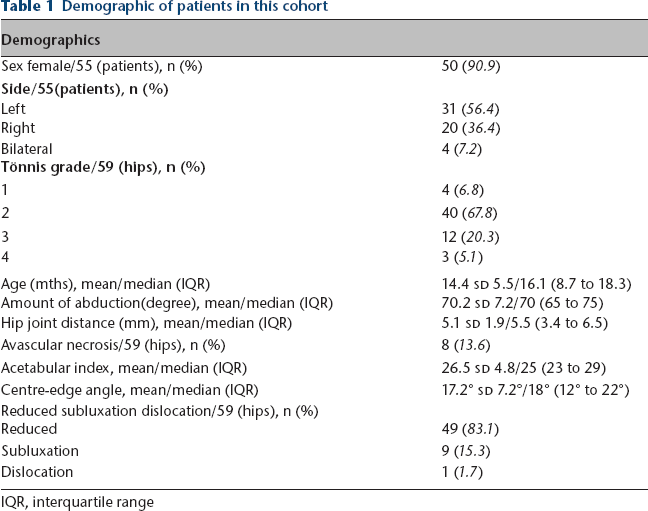
IQR, interquartile range
The mean hip abduction angle was 70.2° sd 7.2° (53° to 85°) on the dislocated side and 63.7° sd 8.8° (40° to 82°) on the normal side; the mean hip joint distance was 5.1 mm sd 1.9 (1.3 to 9.1) on the dislocated side and 2.2 mm sd 0.6 (1.3 to 3.3) on the normal side (Table 1). All hips were immobilized at, at least, 90° of flexion.
Hip abduction angle did not significantly increase the risk of AVN (p = 0.968; 95% confidence interval (CI) for relative risk 0.899 to 1.107). Intra and interobserver agreement was 0.85 and 0.82, respectively. The hip joint distance did not significantly increase the AVN rate (p = 0.65). Intra- and interobserver agreement was 0.75 and 0.77, respectively.
The abduction angle and the hip joint distance were not associated with increased dislocation rate (p = 0.38 and p = 0.14, respectively).
Pearson's correlation analysis found that hip joint distance may be associated with residual acetabular dysplasia (AI) during growth (p = 0.011) (Tables 2 and 3).
Correlation between abduction angle and avascular necrosis (AVN), outcome, final acetabular index (AI) and centre-edge angle (CEA)

logistic regression analysis
Pearson correlation analysis
SE, standard error; RR, relative risk; CI, confidence interval
Correlation between hip joint distance and avascular necrosis (AVN), outcome, final acetabular index (AI) and centre-edge angle (CEA)

logistic regression analysis
Pearson correlation analysis
SE, standard error; RR, relative risk; CI, confidence interval
Logistic regression analysis was performed to investigate the significance of risk factors for AVN (Table 4). There was no significant association between AVN rate and age or sex. On the other hand, severity of dislocation, according to the method described by Tönnis, 18 was found to be significantly associated with the development of AVN (p = 0.019).
Correlation between avascular necrosis (AVN) and age, sex and Tönnis grade

SE, standard error; RR, relative risk; CI, confidence interval
Discussion
Closed reduction and spica cast immobilization under general anaesthesia is the preferred method of treatment in patients with DDH aged six to 24 months,1,2 although many practitioners are evolving toward open reduction and pelvic osteotomy as a standard approach after 18 months of age. 3 The aim of treatment is to obtain a stable reduction of the hip while limiting the risk of AVN. Our findings highlighted the fact that mean hip abduction angle up to 70.2° did not increase the rate of AVN in children with DDH, aged six to 28 months, treated by CR and spica cast immobilization. All 59 hips were reduced at the time of MRI examination.
In our patients, the amount of hip abduction was determined clinically based on stability of reduction. In particular, the more unstable the hip joint is, the higher the hip abduction angle required to preserve reduction. Although there is some controversy regarding the abduction angle of the hip after CR14,19,21,22 as to the ideal amount of abduction, it has come to be accepted that reduced hips should be immobilized in < 55° to 60° of abduction in order to prevent potential compromise of the vascular supply to the proximal femoral epiphysis with resulting epiphyseal osteonecrosis.13,21–23 On the other hand, some researchers think that in order to obtain a stable reduction, hip abduction angle can be increased without increasing the risk of AVN. Older reports by Stanton and Capecci 24 suggest extreme positions of abduction is not a potential contributor to the development of AVN. In the years following, this has been corroborated in more reports. Dibello et al 14 reviewed 25 patients with Graf's type IV DDH (29 hips) who underwent CR and spica cast immobilization at a mean age of 3.4 months. They found that none of them developed AVN during follow-up, and they concluded that abduction angle should be < 70° in order to maintain the hip reduction and to preserve the femoral head perfusion, thus avoiding the risk of AVN. However, this is based almost exclusively on the authors’ experience, as no comparative study nor statistical analysis were conducted to support this conclusion. On the other hand, Schur et al 15 found no significant association between hip abduction and AVN in DDH patients older than six months of age at the time of CR.
Our overall AVN rate was comparable with those of previously published studies. In this series of 55 patients with late-detected DDH (59 hips), the mean abduction angle was 70.2° and the overall incidence of AVN (grade II to IV) was 13.6% (8/59 hips), similar to values reported in previous studies; all hips were immobilized with at least 90° of flexion, as reported by previous studies. Li et al 25 comprehensively reviewed the rate of AVN following CR and spica cast immobilization in children with late-detected DDH. Bradley et al, 26 in a systematic review of 538 hips that had undergone CR, found that the overall rate of significant AVN (types II to IV in both the Kalmachi/MacEwan and Bucholz/Ogden grading schemes) was only 10% at 7.6-year follow-up (Fig. 4).
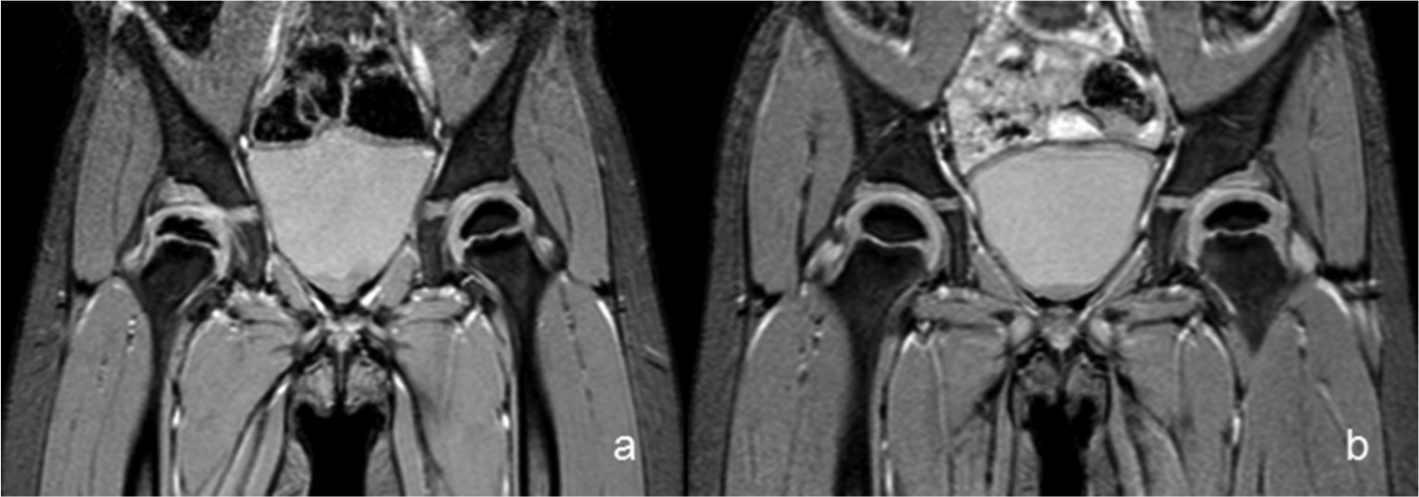
Four-year-old girl with right developmental dysplasia of the hip. MRI performed 2.5 years after CR shows right-side avascular necrosis. Compared with the contralateral side (a), and to unaffected patients (b) the affected epiphysis is smaller and fragmented, with no significant changes at the level of the articular cartilage. On the other hand, the acetabular side is flattened, although articular cartilage has normal appearance and thickness. No fat tissue nor effusion can be observed in the right acetabulum; the medial joint space appears to be slightly widened.
In our series, the contralateral side was placed at a mean of 63.7° of abduction, and none of the contralateral hips developed AVN. We found that the amount of hip joint abduction was not associated with an increased AVN rate. We found that the main factor significantly associated with the development of AVN was the severity of dislocation according to Tönnis. Similar to other studies, the risk of AVN in this series was not affected by age, sex 7 or hip joint distance following CR.
Fogarty and Accardo 6 reviewed 222 congenitally dislocated hips in 173 patients and reported that the incidence of AVN was not affected by the degree of abduction of the hips. More recently, Schur et al 15 reviewed CT scans of 70 patients who underwent successful CR. They measured hip abduction angle and evaluated risk factors for AVN. They found that 29 out of 82 hips developed AVN (35%) and that hip abduction angle did not affect the risk of AVN, consistent with our findings. However, they found that in patients under six months of age at the time of the CR, hip abduction angle > 50° may significantly increase the risk of AVN. They stated that the age-dependent association was consistent with prior clinical, experimental and anatomical investigations that described a changing vascular structure during the first six months of life, with significant vulnerability to extreme abduction. In our series, all patients were older than six months of age at the time of CR.
We encountered some limitations in the analysis of our results. First, the study was limited by available patient data because of its retrospective nature. Second, the mean follow-up was 26.2 months, too early to determine all the actual AVN cases, because the AVN rate increases with time, especially type 2, which may appear until 10 or 11 years of age. Therefore, our results should be considered preliminary and longer follow-up is needed to validate these findings. Third, DeFrancesco et al 16 have pointed out that traditional method for measuring hip abduction using axial imaging does not reflect the true angle, which usually lies in an oblique plane. They found that the traditional method is most accurate at 90° of flexion, but it increasingly overestimates abduction as hip flexion decreases. Although we used the traditional method to assess abduction, all hips were immobilized with at least 90° of flexion. According to DeFrancesco et al 16 hip flexion ≤ 40° exhibits ≥ 10° of error.
Despite these limitations, our preliminary findings highlighted the fact that mean hip abduction angle up to 70.2° did not increase the rate of AVN in DDH patients older than six months and younger than 28 months at the time of index procedure treated with CR and spica cast immobilization. In addition, MRI appears to be a useful method to assess the amount of abduction in DDH patients immobilized in spica cast following CR. In particular, Yong et al 27 have shown that postoperative radiographs are unreliable for assessing the quality of hip reduction in patients with DDH undergoing CR. Compared with standard radiographs, MRI allows more reliable interpretation while decreasing radiation exposure.
Footnotes
XH: Study design, Performed measurements, Manuscript preparation.
LY: Study design, Statistical analysis, Manuscript preparation.
HK: Performed measurements, Manuscript preparation.
LJ: Performed measurements, Manuscript preparation.
BP: Study design, Statistical analysis.
XF: Performed measurements.
FC: Study design, Manuscript modification.