
Abstract
Purpose
The aim of the study was a review of the literature in order to evaluate the results and complications of closed reduction in late-detected developmental dysplasia of the hip (DDH).
Methods
This study consisted of an analysis of the literature relative to late-detected DDH treatment options considering hip congruency, rates of re-dislocation and of avascular necrosis.
Results
Gradual closed reduction (Petit-Morel method) appears to be an effective method concerning joint congruency restitution. Dislocation relapse and avascular necrosis are more efficiently prevented with closed versus open reduction. The tendency for spontaneous correction of acetabular dysplasia decreases if closed reduction is performed after 18 months of age. Patient age at the beginning of traction should be considered for the prognosis, with a lower rate of satisfactory results showing after the age of 3 years.
Conclusion
In our opinion, the Petit-Morel method is a suitable treatment option for children aged between six months and three years with idiopathic DDH.
Keywords
Introduction
Early screening of developmental dysplasia of the hip (DDH) decreased the frequency of late diagnosis and treatment of this disease. 1 However, such cases may still be observed. 2
There is no current consensus between the therapeutic benefits of open and closed reduction. Closed reduction methods have improved significantly during the last 15 years. Originally, Somerville and Scott 3 applied traction followed with open reduction and femoral derotation osteotomy. In the early 1950s, a French team 4 used traction with closed reduction and femoral osteotomy. Later, Morel 5 advocated hip traction with abduction and internal rotation in order to achieve a progressive reduction of the dislocation, followed with a hip spica cast providing a penetration of the femoral head in the acetabulum. 6 Such treatment was named the Petit-Morel technique. 7
The aim of the study was a review of the literature in order to evaluate the published results and complications of closed reduction in late-detected DDH.
Methods
This article analyzes the literature relative to late-detected DDH treatment options considering hip congruency, rates of re-dislocation and of avascular necrosis.
Indications and technique of closed reduction
Indication of gradual closed reduction in late-detected DDH at our hospital is unilateral or bilateral idiopathic DDH over the age of six months and below five years. The child's weight should be at least 6 kg.
The aim of the first stage is to achieve the descent of the femoral head. To this end the child is fitted with a Berck harness (Sté FAG Medical SAS, St Georges de Reneins, France) which is fixed to the bed. Bilateral longitudinal skin traction is then applied with the hips in flexion of 45° for children aged below one year and with hip extension after this age. Horizontal traction is adequate because the iliopsoas tendon is already stretched by the adoptive stance and gait demonstrated after walking age (Fig. 1a). The initial weight used for traction, which corresponds to 10% of the body-weight, is gradually increased depending on the child's weight (up to 50% of their body-weight on each limb) and the degree of migration of the femoral head is assessed on weekly radiographs. When the ossific nucleus is at the level of Hilgenreiner's line, 8 progressive abduction (30° to 50°) and internal rotation equal to the femoral anteversion are applied in order to render the proximal femoral metaphysis horizontal and orientate the epiphysis towards the triradiate cartilage (Fig. 1b). In patients where the ossific nucleus is not radiologically visible, the appropriate time for beginning abduction is when Shenton's line had been restored on the radiographs. The amount of traction is then gradually reduced to allow for reduction of the femoral head into the acetabulum. The average duration of traction in Rampal et al's (2008) 7 experience was 5.3 weeks. Thanks to recent shortening of the traction period, the duration of the traction is now between 3.5 and four weeks.
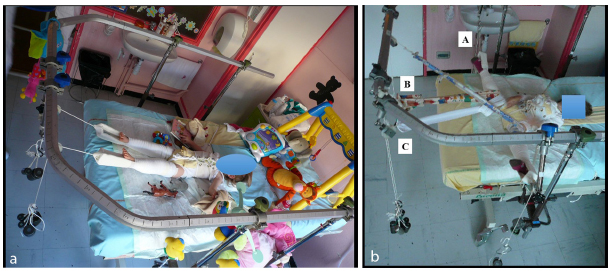
Treatment of a two-year-old girl with right developmental dysplasia of the hip: (
The second stage consists of the stabilization of the ‘presented’ femoral head, in order to allow its progressive ‘seating’ into the acetabulum and a spontaneous definitive concentric reduction. A hip spica cast is applied under general anaesthesia in the reduced position (20° flexion, 45° abduction and slight internal rotation) obtained at the end of the traction stage. Two successive casts, spaced two months apart, are applied.
The third stage consists of the operative management of residual acetabular dysplasia by a pelvic osteotomy. 9 A pelvic osteotomy is indicated if acetabular dysplasia did not show sufficient spontaneous correction at the age of five to six years, or if a tendency to early subluxation was noted.
Results
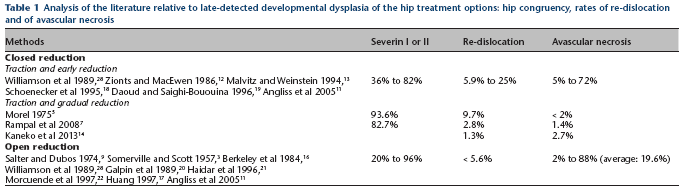
Table 1 displays the results of studies on late-detected DDH applying closed reduction or open reduction considering the hip congruency (Severin score), the rate of re-dislocation and the rate of avascular necrosis.
Analysis of the literature relative to late-detected developmental dysplasia of the hip treatment options: hip congruency, rates of re-dislocation and of avascular necrosis
Discussion
Literature reports good results in term of hip congruency (Severin 10 ) grade I or II) after preliminary traction and early reduction in between 36% and 82%11,12 of hips (Fig. 2). Unsatisfactory evolution was related to residual acetabular dysplasia9,11,13 which did not sustain pelvic osteotomy. After gradual closed reduction and pelvic osteotomy, Morel, 5 Kaneko et al 14 and Rampal et al 7 reported satisfactory results in, respectively, 85.4% and 82.7% and 93.6% of the hips. Thus, considering hip congruency, the Petit-Morel method seems to be the closed reduction method of choice. Open reduction provides excellent or good outcome rates in between 20% 11 and 100%. 15 The best results9,16,17 achieved with open reduction do not differ to those obtained with the Petit-Morel method. Thus, considering hip architecture: closed reduction may not be preferred to open reduction.
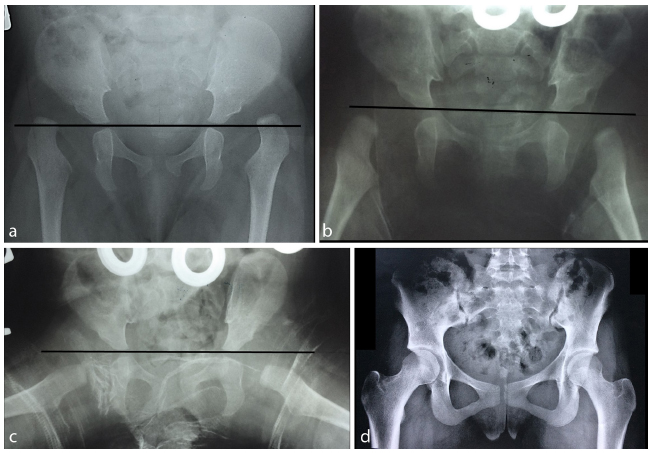
Bilateral developmental dysplasia of the hip in a six-month-old girl: (
Progressive closed reduction may fail in 9.7% of cases. 5 However, a lower rate (4.3%) has been reported. 7 Reduction failure is more frequent after acute closed reduction, with rates varying between 5.9% and 25%.7,17–19 Relapse of dislocation is also reported with open reduction in up to 5.6% of procedures.11,16,17,19,20–22 Thus, it appears that the Petit-Morel method may be more efficient than open reduction in preventing recurrent dislocation. Moreover, relapse of dislocation after open reduction requires surgical revision which is very demanding and often provides non-satisfactory results with avascular necrosis in more than half of cases, with one-third of the hips rated Severin III or worse.20,23 According Angliss et al, 11 the frequency of long-term osteoarthritis was 25% and 49% after, respectively, closed and open reduction. Long-term follow-up displayed a rate of total hip arthroplasty at 45 years after open reduction reaching 46%, revealing significant decreasing of good outcomes after 30 years of age. 24
The tendency for spontaneous correction of acetabular dysplasia 25 decreases if closed reduction is performed after 18 months of age.7,21,26,27 Before pelvic osteotomies, the task of acetabular dysplasia correction was given to femoral varus derotational osteotomy, which did not succeed in correcting this flaw.7,9,13 Pelvic osteotomy, which successfully replaced femoral osteotomy, is an integral part of the Petit-Morel method.
Progressive closed reduction provides the lowest rates of avascular necrosis, reaching 2%.5,7,14 Extemporaneous closed reduction after traction induces higher rates of up to 5.8%.9,12,18 Overhead traction 19 induced a frequency of avascular necrosis of 10%. Angliss et al 11 and Malvitz and Weinstein 13 published unusually high rates, linked to articles’ strict diagnostic criteria. Some articles dealing with closed reduction reported avascular necrosis mostly for relapsed dislocation which required open reduction.12,19 Open reduction7,15,17,19,21,22,28 resulted in poorer frequencies of avascular necrosis which were superior to 5%. This is three-times the rates observed after the Petit-Morel method, reflecting a major effect of open reduction on proximal femoral epiphysis perfusion. Open reduction combined with femoral shortening osteotomy16,20 may explain lower rates of avascular necrosis (< 5%), however, they remain higher than those observed after closed reduction. The Petit-Morel method decreases the risk of avascular necrosis occurring.
The prognosis influence of the age at the beginning of traction should be considered (Fig. 3). Morel 5 reported lower rate of satisfactory results after the age of three years. However, the number of patients older than three years treated according to the Petit-Morel method is too small 7 to draw conclusions from.
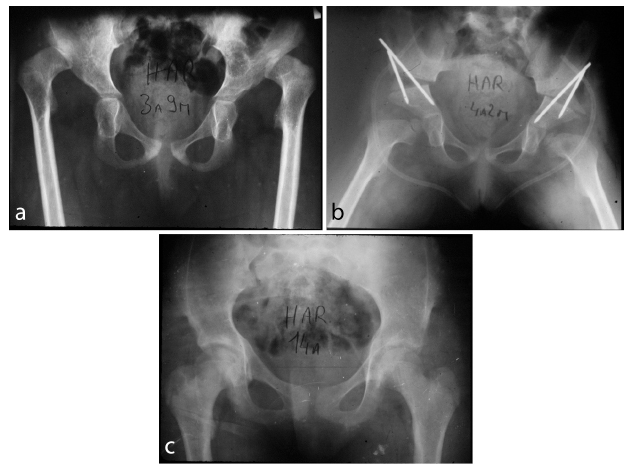
Bilateral developmental dysplasia of the hip in a three years nine months old girl: (
Future developments of this method may include closed reduction combined with open psoas and adductor releases in selected cases 29 and MRI after cast achievement in order to analyze the perfusion of the femoral epiphysis and the quality of the reduction. 30
Finally, mental aspects and inconvenience of traction duration for both children and family should be the focus of a future study.
Conclusions
A study 31 with a mean follow-up of 50 years, which is the longest follow-up published so far, reported satisfactory clinical and radiographic outcomes after gradual closed reduction by skin traction in approximately two-thirds 83 hips.
Regarding the quality of the long-term follow-up results, 32 displaying a hip survival reaching 95% at 40 years follow-up, we consider the Petit-Morel method to be the treatment of choice for children aged between six months and three years with idiopathic DDH.
Footnotes
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
None declared.