
Abstract
Abstract
Purpose
The purpose of this study was to identify if any correlation between size of the proximal femoral epiphysis and avascular necrosis (AVN) exists.
Methods
We retrospectively reviewed 111 patients with developmental dysplasia of the hip treated by closed reduction (124 hips). The diameter and height of both femoral head and ossific nucleus were assessed on preoperative MRI.
Results
The diameter and the height of the femoral head as well as of the ossific nucleus of the contralateral side were significantly greater than the dislocated side. AVN occurred in 21 (16.9%) out of 124 hips. The rate of AVN gradually decreased with age: 30.0% at six to 12 months, 18.2% at 12 to 18 months and 3.7% at 18 to 24 months. Spearman correlation analysis showed that age is negatively correlated with the incidence of AVN (r = -0.274; p = 0.002) and the diameter of the femoral head has a significantly negative association with the incidence of AVN (r = -0.287; p = 0.001). No significant association was observed between the incidence of AVN and height of the femoral head or size of the ossific nucleus. Hips with AVN were significantly smaller than hips without AVN.
Conclusions
The size of both the femoral head and the ossific nucleus increase with age although the dislocated femoral head is smaller compared with the contralateral side. The diameter of the femoral head and not the size of the ossific nucleus negatively correlate with the risk of AVN, with a bigger femoral head showing lower risk of AVN.
Level of evidence
III
Keywords
Introduction
Avascular necrosis (AVN) of the proximal femoral epiphysis is a potential complication in children with developmental dysplasia of the hip managed by closed reduction (CR). The goal of treatment is to achieve early, stable reduction of the hip joint and to avoid AVN as it can lead to early degenerative arthritis and/or lower limb length discrepancy, and may ultimately require hip salvage surgery or hip joint replacement.
The reports of AVN in children with developmental dysplasia of the hip (DDH) treated by CR varies between 0% and 67% although its cause remains unknown.1–6 Age, 6 high dislocation 7 and absence of ossific nucleus 8 have been reported as risk factors for AVN in children with DDH treated by CR.
Although several studies have suggested an association between the presence of the ossific nucleus and a lower rate of AVN in children with DDH treated by closed means, others have raised the concern as to whether its presence truly protects the proximal femoral epiphysis from the occurrence of AVN.7–15 Moreover, there is a lack of studies investigating the potential association between the size of the proximal femoral epiphysis and the occurrence of AVN.
The aim of this study was to retrospectively evaluate: 1) the size of the proximal femoral epiphysis measured with preoperative MRI in children with DDH treated by CR and spica cast immobilization; and 2) to evaluate the presence of AVN on anteroposterior (AP) pelvis radiographs taken at last follow-up visit. The secondary aim was to identify if any correlation exists between the size of the proximal femoral epiphysis and AVN, the hypothesis being that patients with bigger proximal femur epiphysis have a lower risk of developing AVN.
Materials and methods
After obtaining approval from our institutional review board, we retrospectively reviewed the medical records of 276 patients diagnosed with DDH and treated with CR and cast immobilization at our centre between June 2011 and December 2015.
The inclusion criteria were as follows: 1) diagnosis of DDH; 2) age six to 24 months at initial treatment by CR and spica cast immobilization; 3) complete clinical and radiographic data including preoperative MRI and postoperative AP radiographs; 4) at least 24 months of clinical follow-up.
Exclusion criteria were as follows: 1) concomitant diagnosis of cerebral palsy, arthrogryposis multiplex congentita, myelomeningocele, tethered cord syndrome or other neuromuscular condition; 2) patients older than 24 months at initial treatment; 3) follow-up less than 24 months; 5) incomplete clinical and radiographic data.
A total of 111 out of 276 (40.2%) patients (99 girls, 12 boys; 124 hips) met the inclusion criteria. The left hip was involved in 57 patients (51.4%) and the right hip was involved 41 patients (36.9%); 13 patients had bilateral involvement (11.7%). The mean age at the time of CR was 15.6 months (sd 3.6; 6 to 22.2), and the mean follow-up time was 38.7 months (sd 10.0; 24 to 63).
CR was performed under general anaesthesia in all cases. Arthrogram of the hip joint was performed to evaluate the hip position and to assist reduction. Adductor tenotomy was performed if the adductor was considered an obstacle to CR. After CR, an abduction cast was applied for three months in order to maintain reduction, and it was changed once after six to seven weeks. After cast removal, patients were placed into an abduction brace for an additional six months (three months full-time and three months night-time use only).
Radiographic assessment
All patients were followed up for at least 24 months. MRI was obtained prior to CR in all patients. AP pelvis radiographs in neutral and frog position were obtained prior to CR, immediately after CR and at each follow-up visit. Acetabular index (AI) and centre-edge angle (CEA) was measured on AP pelvis radiographs prior to CR and at last follow-up visit. 16
The severity of hip dislocation was rated according to the Tönnis grading system. 17
AP and frog lateral radiographs taken at last follow-up visit were used to evaluate the primary outcome measure, namely, if AVN was or was not present. AVN of the femoral epiphysis was graded according to method described by Kalamchi-MacEwen. 18 With type I AVN, changes are limited to the femoral head, and the metaphysis was not involved, therefore, type I AVN is thought to represent transient ischemia of the femoral head that can recover completely. 19 Therefore, we grouped type I AVN within the normal hip category.
Final outcome was evaluated with the Severin classification. Severin grades I and II were considered satisfactory outcomes, while Severin grade III and IV were considered unsatisfactory outcomes. 20
Two independent raters (WJ and LY) evaluated AVN. If they could not come to an agreement on the type of AVN, a discussion with at least three other senior paediatric orthopaedic surgeons was performed.
Ossific nucleus and size of the proximal femoral epiphysis
All radiographic measurements were performed using standard picture and archiving communication system software (PACS, Beijing, China).
MRI (T2-FFE; Philips, Best, The Netherlands) was used to measure: 1) the diameter of femoral head; 2) the height of femoral head; 3) the diameter of ossific nucleus; 4) the height of ossific nucleus (Fig. 1).
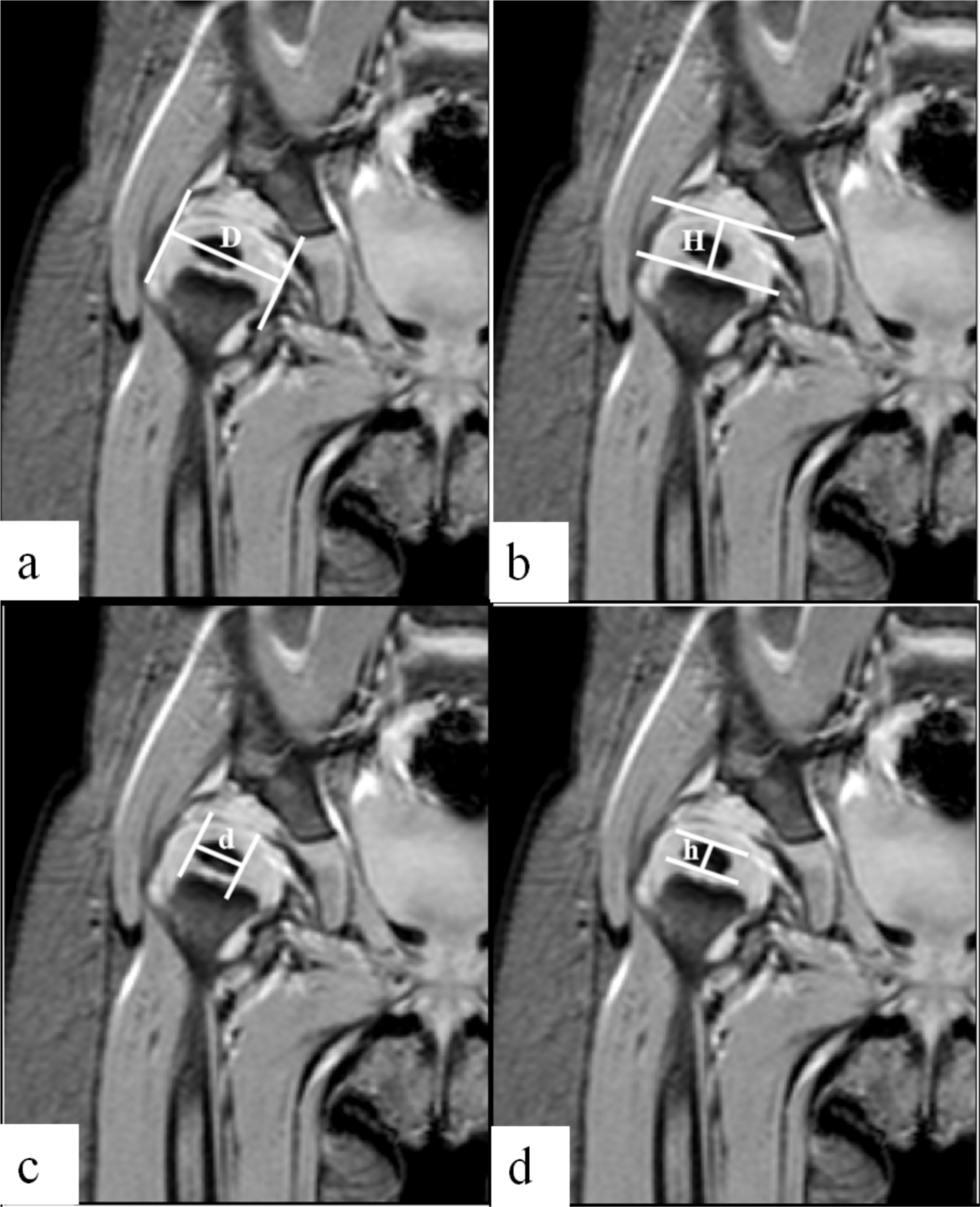
Measurement of the diameter and height of both femoral head and ossific nucleus on preoperative MRI. The diameter of the femoral head (D) is the distance between two lines tangent to the inner and outer border of the femoral head, and perpendicular to the growth plate of the proximal femoral epiphysis
The diameter of the femoral head (D) is the distance between two lines tangent to the inner and outer border of the femoral head, and perpendicular to the growth plate of the proximal femoral epiphysis (Fig. 1a).
The height of the femoral head (H) is the distance between two parallel lines, one passing through the growth plate of the proximal femur epiphysis, and the second tangent to the top of the femoral head (Fig. 1b).
The diameter of the ossific nucleus (d) is the distance between two lines tangent to the inner and outer border of the ossific nucleus, and perpendicular to the growth plate at its bottom (Fig. 1c).
The height of the ossific nucleus (h) is the distance between two lines parallel to the growth plate of the proximal femur epiphysis and tangent to the top and the bottom of the ossific nucleus (Fig. 1d).
All measurements are expressed in cm.
Statistical analysis
Statistical analysis was performed with SPSS software (version 20.0; SPSS, Chicago, Illinois). Spearman correlation analysis was used to analyze the diameter or height of femoral head or ossific nucleus between age, Tönnis grade, preoperative AI and AVN. The chi squared test, analysis of variance and t-test were used to further confirm the results of Spearman correlation analysis. The tests were two-sided, and a p-value of < 0.05 be significant.
Results
Radiographic measurements showed good to excellent interobserver reliability for AI (intraclass correlation coefficient (ICC) = 0.901), CEA (ICC = 0.843), femoral head height (H) (ICC = 0.919), ossific nucleus height (h) (ICC = 0.928), femoral head diameter (D) (ICC = 0.949) and ossific nucleus diameter (d) (ICC = 0.936).
Among the included 124 hips, three hips (2.4%) were Tönnis grade I, 51 (41.1%) grade II, 66 (53.3%) grade III and 4 (3.2%) were grade IV.
Preoperative mean AI was 35.6° (sd 4.3°; 25° to 44.9°). At the final follow-up, mean AI was 20.7° (sd 5.8°; 3.2° to 37.2°) and mean CEA was 23.7° (sd 9.2°; 0° to 42°). According to Severin classification, 93 hips (75.0%) were grade I, seven (5.7%) grade II, 22 (17.7%) grade III and two2 (1.6%) were grade IV; overall, 100 hips (80.6%; I + II) had satisfactory outcome and 24 hips (19.4%; III + IV) had unsatisfactory outcome.
Femoral head height (H), ossific nucleus height (h), femoral head diameter (D) and ossific nucleus diameter (d) of the unaffected side were significantly greater compared with the dislocated side (p < 0.001) (Table 1).
The size (cm) of the femoral head and of the ossific nucleus in patients with developmental dysplasia of the hip
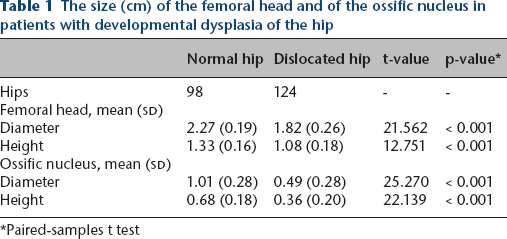
Paired-samples t test
Spearman correlation analysis showed that Femoral head height (H), femoral head diameter (D) and ossific nucleus diameter (d) significantly increased with age (Fig. 2). Femoral head height (H), femoral head diameter (D) and ossific nucleus diameter (d) in patients aged six to 12 months at the time of CR were significantly smaller compared with patients aged 12 to 18 months and 18 to 24 months at the time of index procedure (Table 2).
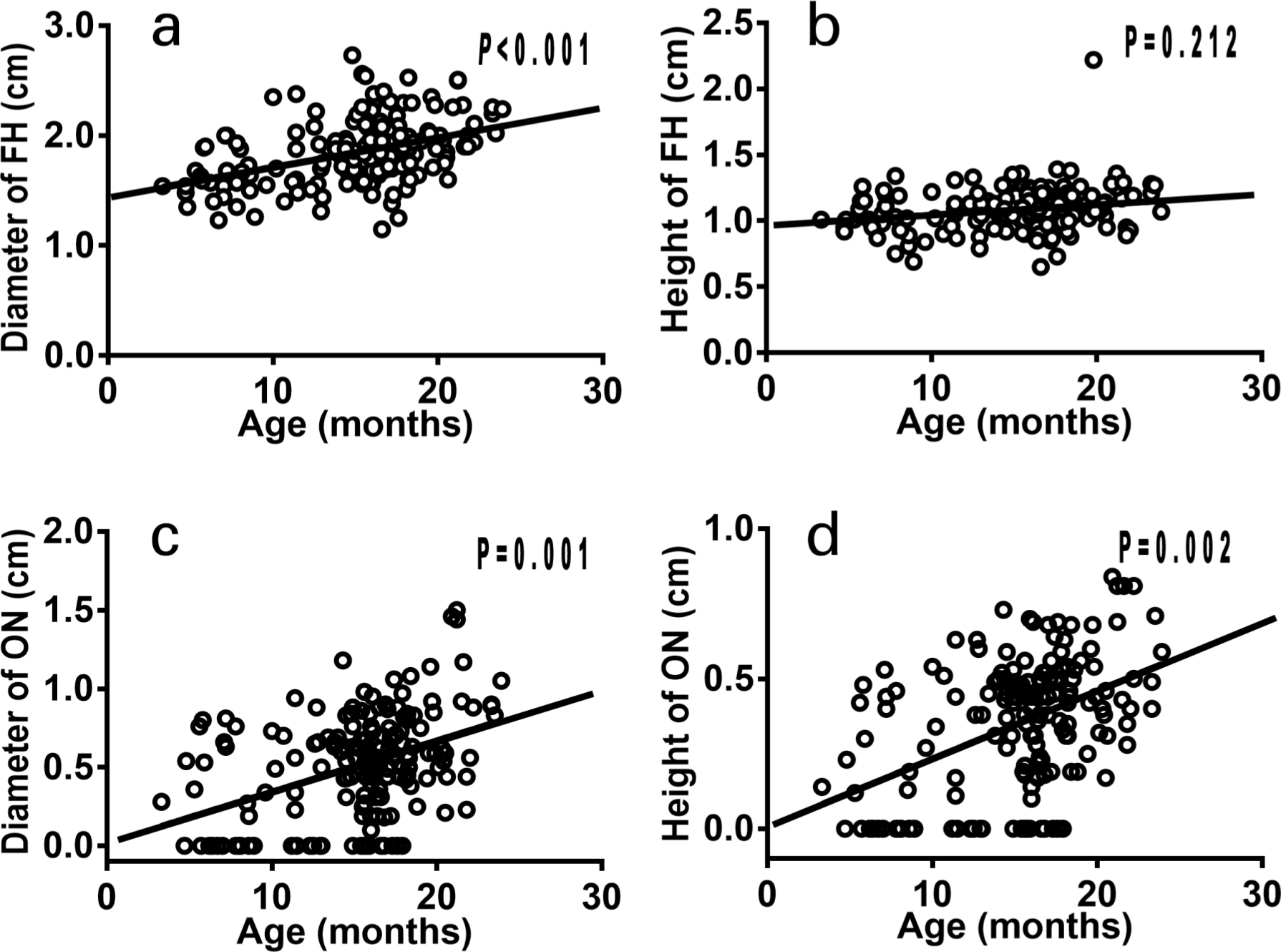
Scatter plot of actual measurement of femoral head (FH) or ossific nucleus (ON) diameter or height (cm) by MRI and age (months).
Spearman correlation analysis indicates correlation between the size of the ossific nucleus and of the femoral head, age, Tönnis grade and preoperative acetabular index (AI)
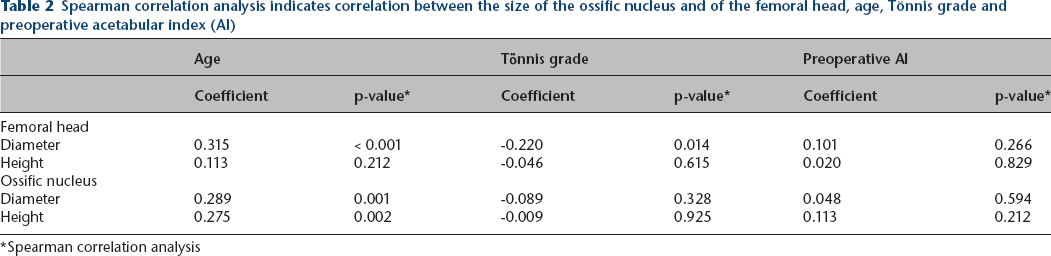
Spearman correlation analysis
Femoral head diameter (D) was negatively correlated with Tönnis grade (r = -0.220; p = 0.014); Tönnis grade I and II hips (1.95 cm (sd 0.33)) hips had significantly greater femoral head diameter (D) compared with grade III and IV hips (1.79 cm (sd 0.21)) (t = 3.048; p = 0.003). There was no significant association between preoperative AI and Femoral head diameter (D), femoral head height (H), ossific nucleus diameter (d) and ossific nucleus height (h) (Table 3).
Comparison between the size (cm) of femoral head and the ossific nucleus in dislocated hips among patients of different age (six to 12 months; 12 to 18 months; and 18 to 24 months)
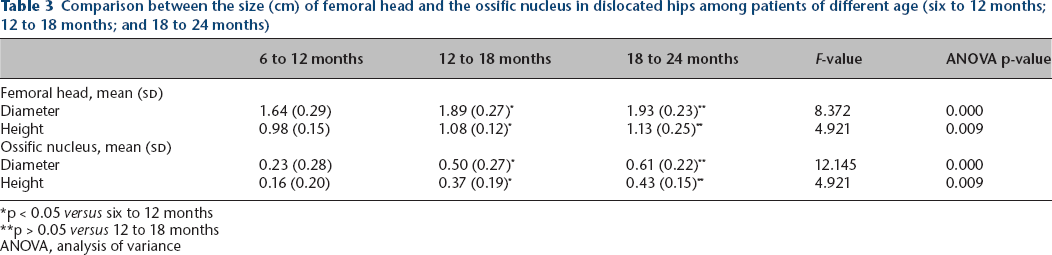
p < 0.05 versus six to 12 months
p > 0.05 versus 12 to 18 months
ANOVA, analysis of variance
In all, 21 out of 124 hips (16.9%) developed AVN, including 12 type II AVN (57.2%), seven type III AVN (33.3%) and two type IV AVN (9.5%). Spearman correlation analysis showed that age is negatively correlated with the incidence of AVN (r = -0.274; p = 0.002). The rate of AVN gradually decreased with age: 30.0% at six to 12 months, 18.2% at 12 to 18 months and 3.7% at 18 to 24 months (p = 0.033).
Spearman correlation analysis showed that the diameter of femoral head has significantly negative association with the incidence of AVN (r = -0.287; p = 0.001). In patients with Tönnis grade I to II dislocation, the diameter of the femoral head was negatively associated with the incidence of AVN (r = -0.453; p = 0.001). Similar results were observed in patients with Tönnis grade III to IV dislocations (r = -0.534; p = 0.001) (Table 4).
Subgroup analysis investigating the association between avascular necrosis and the size of the ossific nucleus and of the femoral head in Tönnis grade I to II and grade III to IV hips
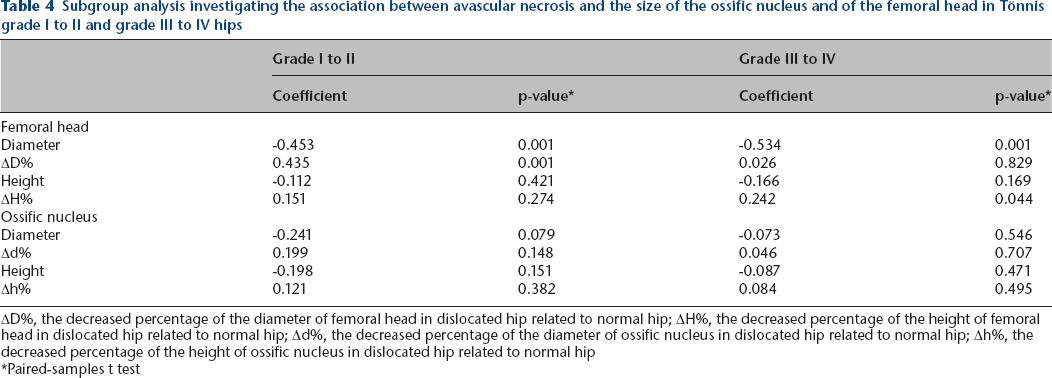
ΔD%, the decreased percentage of the diameter of femoral head in dislocated hip related to normal hip; ΔH%, the decreased percentage of the height of femoral head in dislocated hip related to normal hip; Δd%, the decreased percentage of the diameter of ossific nucleus in dislocated hip related to normal hip; Δh%, the decreased percentage of the height of ossific nucleus in dislocated hip related to normal hip
Paired-samples t test
No significant association was observed between the incidence of AVN and Femoral head diameter (D), femoral head height (H), ossific nucleus diameter (d) and ossific nucleus height (h). Femoral head diameter (D) was significantly smaller in patients with AVN (1.69 cm (sd 0.19)) compared with patients without AVN (1.89±0.28 cm); on the other hand, Femoral head height (H), ossific nucleus diameter (d) and ossific nucleus height (h) were similar between patients with or without AVN (p > 0.05) (Table 5).
The association between avascular necrosis (AVN) and the size (cm) of the ossific nucleus and of the femoral head in dislocated hips
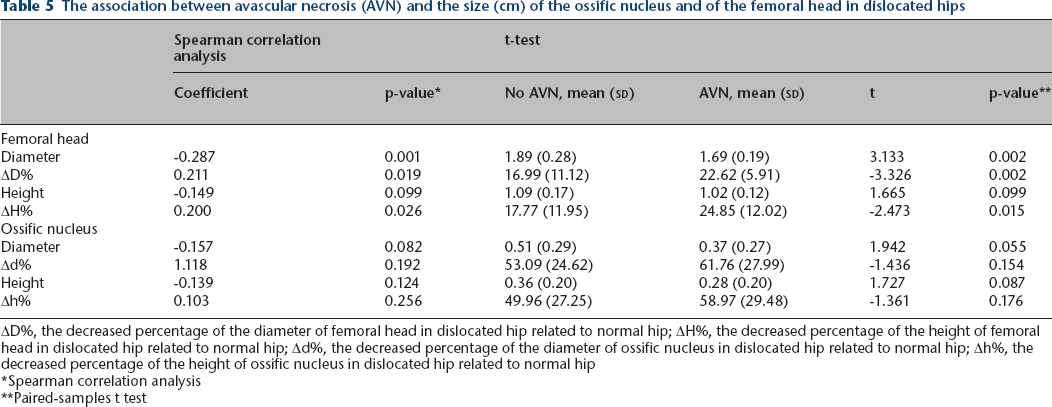
ΔD%, the decreased percentage of the diameter of femoral head in dislocated hip related to normal hip; ΔH%, the decreased percentage of the height of femoral head in dislocated hip related to normal hip; Δd%, the decreased percentage of the diameter of ossific nucleus in dislocated hip related to normal hip; Δh%, the decreased percentage of the height of ossific nucleus in dislocated hip related to normal hip
Spearman correlation analysis
Paired-samples t test
In all, 15.2% (16/105) of the hips with an ossific nucleus and 26.3% (5/19) of the hips without an ossific nucleus at the time of CR developed AVN; the AVN rate was not significantly different between the two groups (p = 0.394).
Discussion
This study showed that the size of both the femoral head and of the ossific nucleus increase with age. However, the dislocated side showed a smaller femoral head and ossific nucleus compared with the contralateral side. These findings confirm previous studies. However, none of previously published reports correlated the size of femoral head and the ossific nucleus with occurrence of AVN in children with DDH treated by CR between six and 24 months of age.21–24
Wanner et al 21 measured the size of the proximal femoral epiphysis with ultrasound in 37 children with DDH and compared with 75 normal children; they found that the dislocated side was smaller in diameter compared with the contralateral side. Our findings also suggest that the severity of dislocation negatively correlates with the size of the femoral head; in particular, the higher the dislocation, the smaller the proximal femur epiphysis. O'Brien and Salter 22 reviewed 103 cases of untreated DDH adult patients, and found that the size of the femoral head of the dislocated side was smaller compared with the unaffected side; they also pointed out that dislocated hips had smaller femoral heads compared with subluxated hips. Similar findings were reported in children by works of Sugano et al 23 and of Crowe et al. 24 Therefore, we cannot recommend delaying CR until the femoral head has grown bigger; on the contrary, we suggest timely CR in order to enhance hip joint development thanks to the reciprocal interaction between femoral head and acetabulum.
Several studies have reported that the femoral head is important for promoting the development of the acetabulum regardless of its shape, round or ovoid. In particular, the femoral head with abnormal shape can also affect the development of the acetabulum by inducing progressive morphological modifications.25,26 Steppacher et al 27 and Clohisy et al 28 found that the morphological development of the acetabulum is influenced by the shape of the femoral head. Our study shows that the size of femoral head is not significantly associated with preoperative AI.
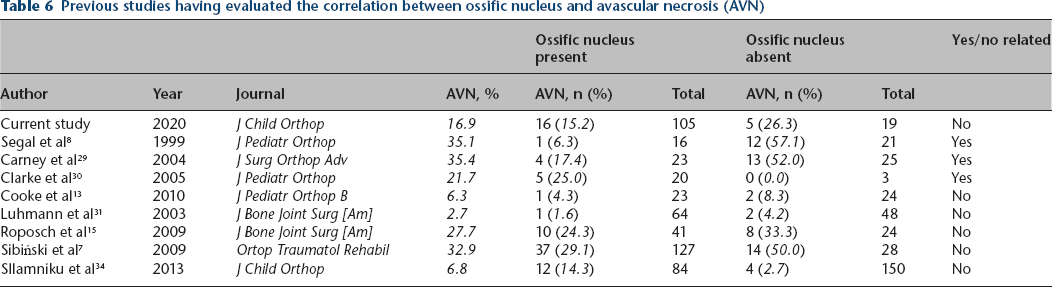
Moreover, our findings showed no significant correlation between the presence of the ossific nucleus and the occurrence of AVN. However, previously published data are conflicting.8–15,29–31 Some authors have suggested that the presence of ossific nucleus at the time of CR is protective against the occurrence of AVN. Carney et al 29 reviewed 45 cases (58 hips) of DDH treated by CR and concluded that delaying CR until ossific nucleus would lower the incidence of AVN and hypothesized that the ossific nucleus may add mechanical strength to the femoral head and protect the epiphyseal blood supply from extrinsic compression.8,32,33 However, most studies indicated that the presence of ossific nucleus did not reduce the rate of AVN (Table 6).7,13,15,31,34 Similarly, the meta-analyses by Chen et al, 11 Niziol et al 14 and Roposch et al 15 did not find evidence to support the protective effect of the ossific nucleus on the development of AVN, which is consistent with our findings. In addition, our data suggest there is no significant association between the size of ossific nucleus and the occurrence of AVN; similar findings were reported by Sibiński et al 7 who reviewed 103 DDH hips (n = 77) and could not find any significant association between the size of the ossific nucleus and AVN. Thus, in clinical practice we do not recommend delaying treatment until the appearance of the ossific nucleus. Our current study showed that the occurrence of AVN negatively correlates with the diameter of femoral head and age at reduction. In particular, although the diameter of the femoral head negatively correlates with the severity of the dislocation according to the Tönnis grading system, subgroup analysis found that incidence of AVN negatively correlates with the size (diameter) of the femoral head in both Tönnis grades I to II and III to IV dislocations. Results of previous studies about the effect of age on AVN remain controversial. Most studies reported that the occurrence of AVN did not increase with age. Schur et al, 12 Sankar et al, 3 Gregosiewicz and Wośko, 35 Brougham et al 36 and Cha et al 37 reported that there was no significant difference in the incidence of AVN among different ages, and concluded age was not a risk factor for AVN. However, many other studies showed contradictory results. Sibiński et al, 7 Weiner et al 10 and Kruczynski 38 found that the incidence of AVN increased and the severity decreased with age. Schur et al 12 and Kalamchi and MacEwen 18 noted that the severe forms of AVN decreased with age, especially in patients older than six months when treated. Our findings indicate that the rate of AVN decreases with age, maybe due to increased number and size of vessels to the proximal femoral epiphysis in older children.39–42
Previous studies having evaluated the correlation between ossific nucleus and avascular necrosis (AVN)
It should be noted that there are still some limitations in the present study: this is a retrospective study and the follow-up time (24 to 63 months) is relatively short. However, follow-up time is enough to make sure as to whether AVN has occurred or not, as reported by previously published studies.1,5,6,16 The correlation coefficient between the size of femoral head and incidence of AVN is relatively weak (r = -0.287); therefore, further studies with larger number of patients are needed to evaluate the effects of the size of femoral head on the incidence of AVN.
Conclusion
The size of both the femoral head and the ossific nucleus increase with age although the dislocated femoral head is smaller compared with the contralateral side. The diameter of the femoral head negatively correlates with the severity of the dislocation. Similarly, the diameter of the femoral head and not the size of the ossific nucleus negatively correlates with the risk of AVN, with bigger femoral heads showing lower risk of AVN.
Footnotes
YZ: Study design, Performed measurements, Manuscript preparation.
LJ: Study design, Statistical analysis, Manuscript preparation.
ZM: Performed measurements, Manuscript preparation.
FC: Performed measurements, Manuscript preparation.
XF: Study design, Statistical analysis.
LY: Performed measurements.
XH: Study design, Manuscript modification.