
Abstract
Purpose
Excessive in-spica abduction is a risk factor for oste-onecrosis after surgical reduction for developmental dysplasia of the hip (DDH). The traditional method for radiographically measuring hip abduction using axial imaging does not reflect the true angle, which usually lies in an oblique plane. The purpose of this study was to describe a novel method for measuring true hip position using advanced imaging.
Methods
A trigonometric model was derived to define hip position based upon the femoral axis angular deviation from midline as measured on axial and coronal sequences of MRI studies. In-spica MRIs of 28 hips having undergone surgery for DDH were reviewed. On two separate occasions, the same three raters measured the femoral axis deviation from mid-line on axial and coronal imaging. Abduction was estimated using the traditional method of measurement and our novel method. Intra- and inter-rater reliability were assessed.
Results
The methods yielded different estimates (p < 0.001). Inter- and intra-rater reliability were excellent for both methods (inter-rater ICC > 0.922, intra-rater ICC > 0.919). The traditional method is accurate at 90° of flexion, but it increasingly overestimates abduction as hip flexion decreases. All cases where hip flexion was ≤ 40° exhibited ≥ 10° of error.
Conclusions
Decreasing hip flexion in spica modifies the perceived angle of abduction as measured using axial imaging. This inaccuracy can be overcome through assessment of orthogonal views using our new approach, which is accurate and reliable. It should be considered for future research investigating the effects of in-spica hip position on outcomes of DDH treatment.
Introduction
Avascular necrosis (AVN) is one of the most serious complications of open or closed reduction of the hip in the treatment of developmental dysplasia of the hip (DDH), with reported rates in the range of 6% to 48%. 1 Early studies suggested that excessive post-operative hip abduction in spica is an important risk factor for developing osteone-crosis.2–4 Further, it has been demonstrated that avoiding extremes of abduction in post-operative immobilisation significantly reduces the incidence of AVN.5,6 Based on these data, it has become well accepted that reduced hips should be immobilsed in less than 55° to 60° of abduction to prevent potential compromise of the vascular supply to the proximal femoral epiphysis and resulting osteonecrosis.
In this era of advanced imaging, axial sequences from CT or MRI are often used in the DDH literature to assess the degree of abduction in spica. At 90° of hip flexion, an axial image is orthogonal to the plane of flexion and is therefore an appropriate means of assessing the amount of abduction. However, with in-spica hip flexion < 90°, axial images are not orthogonal to the plane of flexion and therefore are inappropriate for assessing abduction. This is especially true in cases of open reduction where more modest hip flexion, typically around 30°, is recommended for post-operative immobilisation.1,7,8 Despite this shortfall in measurement technique, it has been our observation that practitioners and researchers continue to use the traditional method of radiographically estimating hip abduction—measuring the deviation of the femoral axis from midline as seen on axial imaging—even when the hip is flexed to < 90°.9,10 The purpose of this study was to develop a novel way to accurately estimate hip abduction regardless of hip flexion angle. We also sought to analyse the traditional method's accuracy and reliability compared with our novel method.
Materials and methods
Model development
Precisely defining the cardinal angles of the hip joint was a prerequisite in this study. We defined true abduction as the angular deviation of the femoral axis from a sagittal plane. More accurately, it was defined as the smallest angle between the femoral axis and any sagittal plane. This angle can be imagined to lie in the plane of flexion as shown in Figure 1. Hip flexion was defined as the angle between the plane of flexion and a coronal plane. Continuing with definitions, we recognised that the traditional measure for hip abduction taken from axial imaging is better conceptualised as a projection of the hip abduction angle in the axial plane. Similarly, the angular deviation of the femoral axis from the midline as seen on coronal imaging could be conceptualised as the hip abduction angle in a coronal projection.
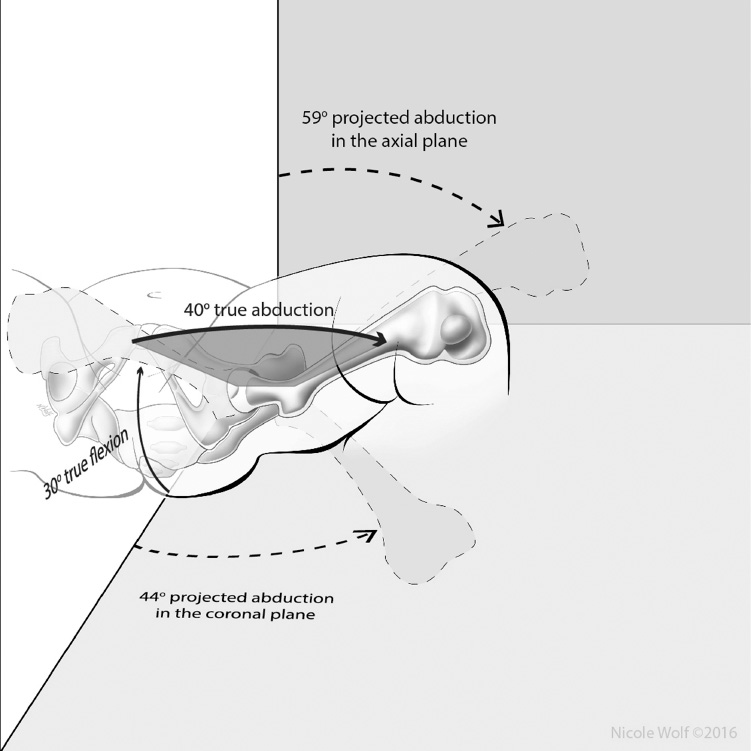
Rendering of an immobilised hip in 30° of flexion – a typical position after open reduction. Despite the leg being in only 40° of true abduction, the angular deviation of the femoral axis from midline as seen on axial imaging is 59°. For this example, the traditional method for estimating abduction therefore overshoots the true value by 19° (or 47.5%).
After having defined the four angles—true abduction, flexion, the axial projection of abduction and the coronal projection of abduction—we developed a geometric model from which we derived the relationships between the angles. These relationships are described by the equations seen in Figure 2.
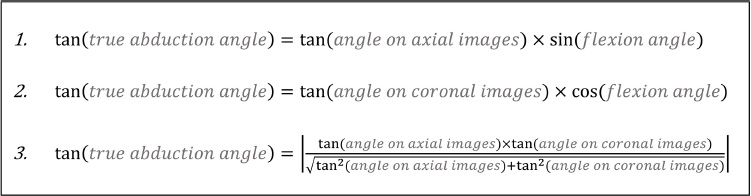
Equations describing the relationship between the angles shown in Figure 1. These were derived from a geometric model.
From these equations, one can see that the degree of hip flexion dictates the agreement between the projected angle on axial or coronal images and the true angle of abduction. Equation 1 shows that, at 90° of hip flexion, the femoral shaft angle measured on axial images does indeed represent the true angle of abduction. Equation 2 shows that, at 0° of hip flexion, the angle as measured on coronal images accurately represents abduction. However, between 0° and 90°, true abduction is not accurately represented on either axial or coronal cuts. Instead the true angle of abduction can be calculated using Equation 3, but only if the measurements from both axial and coronal imaging are known. This model also shows that, for a given angle of abduction, the traditional method of measurement will consistently overestimate abduction with error inversely related to hip flexion (Fig. 3).
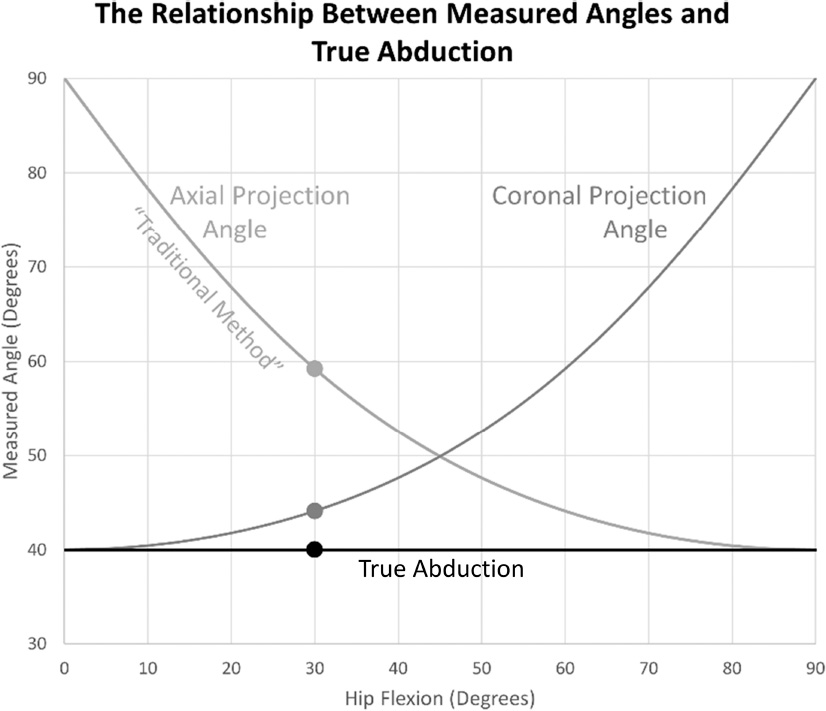
This graph illustrates how, for a given degree of true abduction (in this case 40°), the femoral axis angles seen on axial and coronal imaging vary considerably with changing hip flexion. Note that at 0° of hip flexion, the angle in the coronal plane is identical to the true abduction angle. Meanwhile at 90° of hip flexion, the angle in the axial plane agrees with the true abduction angle. The markers at 30° of hip flexion correspond to the position illustrated in Figure 1.
Assessment of accuracy and reliability
Appropriate institutional review board approval was given before any patient data were analysed. Assuming a Type I error rate of 5% and a power of 80%, an a priori power analysis indicated that more than 26 participants would be needed to find a statistically significant difference between good and excellent inter-rater reliability (intraclass correlation coefficient (ICC) 0.6 vs 0.8, respectively).11,12 Accordingly, post-operative images from 28 hip reductions were retrospectively reviewed. As post-operative hip positioning often varies based upon type of reduction (open vs closed), participants’ hips were consecutively sampled to yield 14 open and 14 closed reduction cases and thus provide a larger distribution of hip positions. Raters consisted of one paediatric orthopaedic surgeon, one paediatric musculoskeletal radiologist and one paediatric orthopaedic surgery fellow. Raters were instructed to measure hip abduction using two methods: the traditional method and our novel method. The traditional measurements were made according to previously-published guidelines. 9 This process begins with an axial image through the ischial tuberosities. A transverse line is drawn connecting the posterior edges of the ischial tuberosities. Next, a sagittal line is drawn perpendicular to the transverse line. A third line defines the axis of the femoral shaft. The axial femoral shaft angle (traditional measure) is then taken as the angle between the sagittal line and the femoral axis line (Fig. 4).
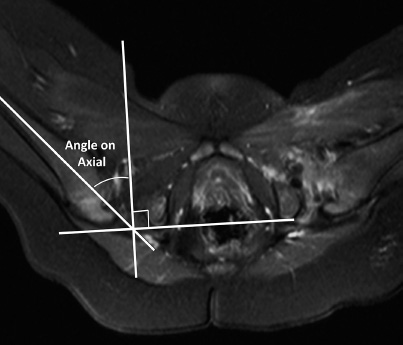
This axial image from a post-operative MRI scan illustrates the traditional method for estimating hip abduction in spica. This involves drawing a transverse line across the posterior aspects of the ischial tuberosities followed by the placement of a sagittal line perpendicular to the first. The traditional angle is measured between the femoral shaft axis and the sagittal line.
Raters were next asked to make measurements using coronal images in a similar manner. In this process, Hilgenreiner's line is first drawn through the triradiate cartilages. Next, a sagittal line is drawn perpendicular to Hilgenreiner's line. Again, a line is made along the femoral shaft axis. The coronal femoral shaft angle measurement is the angle between the sagittal line and the femoral axis line (Fig. 5). For each hip analysis, the axial femoral shaft angle (traditional measurement) and the coronal femoral shaft angle were used to calculate the true hip abduction using Equation 3. Hip flexion angles were also calculated according to the model. At a later date, all measurements were repeated by all three raters on a randomly ordered set of the same 28 images to allow for intra-observer calculations.
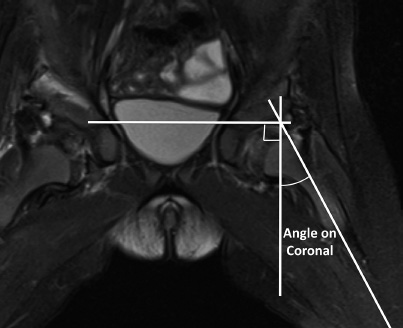
This coronal image from a post-operative MRI scan shows how femoral axis angular deviation as seen in the coronal plane was measured in this study. Hilgenreiner's line is first drawn, followed by a sagittal line perpendicular to it. The coronal projection angle is then measured between the femoral shaft axis and the sagittal line. Using this measurement along with that shown in Figure 4, one can calculate the true angle of hip abduction using Equation 3.
Statistical analyses were performed using a commercially available spreadsheet program and Stata (Version 14.1; StataCorp.; College Station, TX, USA). ICCs were used to quantify inter-rater and intra-rater reliability for each method. As described in the literature, an ICC of 0 describes no agreement while a value of one describes perfect agreement between observations. ICC values > 0.6 are considered ‘good’ while those > 0.8 are ‘excellent’.11–13
Results
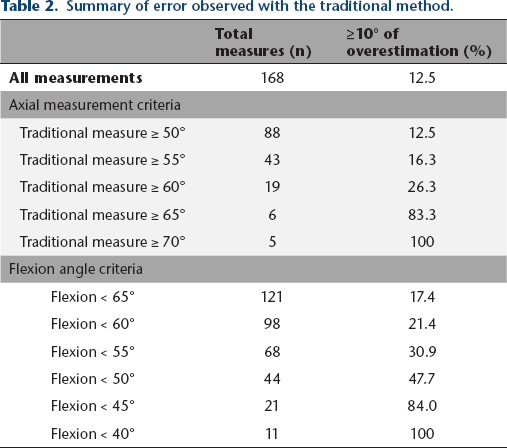
There was a significant difference between the traditional and novel measurements for hip abduction (paired t-test, p < 0.001). This was confirmed when comparing the repeated sets of measurements (p < 0.001). There was also a significant difference in true abduction measurements between the open and closed reduction groups as seen in Table 1 (Kruskal-Wallis test, p = 0.001). The theory that error would increase with decreasing hip flexion, as demonstrated by our model, was supported by findings shown in Table 2. When the calculated hip flexion angle was < 40°, there was a 100% incidence of measurement error ≥ 10° with the traditional method (11/11). Error also varied with the traditional measurement itself. Notably, 83.3% (5/6) of traditional measurements ≥ 65° were at least 10° overestimated, while only 9.9% (16/162) of traditional measurements < 65° exhibited this level of error. It is important to once again note that each traditional measure can mathematically only be greater than the corresponding novel measure, meaning that any error represents overestimation of hip abduction using the traditional measure. As an example of the error exposed via our model, we found that a hip flexed to 30° in spica will measure 59° using the traditional method when the true abduction is only 40°.
Description of hips and differences in measurements
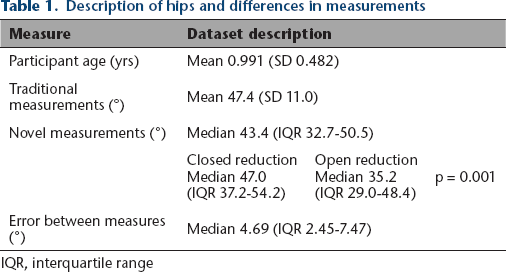
IQR, interquartile range
Summary of error observed with the traditional method.
Inter-rater reliability was assessed via two-way random effects models for consistency between individual observations, revealing excellent reliability for both the traditional (ICC 0.922-0.942) and the novel methods (ICC 0.976-0.978). 13 Intra-rater reliability, assessed with two-way mixed effects models for absolute agreement between individual observations, was also excellent for both methods (ICC 0.919-0.936 for traditional, 0.975-0.974 for novel).12,13 The mean standard deviation among angle measures was lower for the novel method compared with the traditional method (1.46 vs 2.12 on initial ratings, 1.62 vs 2.16 on repeat ratings).
Discussion
AVN is well recognised as the most devastating complication of DDH treatment. Although the exact aetiology remains poorly defined, previous studies have suggested a relationship between extremes of post-operative abduction in spica, epiphyseal vascular compromise and the risk of developing osteonecrosis.2,6,14–17 Other studies have shown that limiting the degree of abduction after hip reduction can reduce the incidence of AVN.5,6,18 As a result, it has become dogma within the paediatric orthopaedic community to immobilise hips in no more than 55° to 60° of abduction post-operatively to prevent compromising the vascular supply of the proximal femoral epiphysis and causing AVN.
With the advent of advanced imaging (CT and MRI), investigators have traditionally measured hip abduction using selected axial images through the hip joint.9,10 However, traditional methods that use only axial imaging may be misguided because axial measurements actually describe a projection of the abduction angle rather than the true angle. When a hip is flexed to 90° in spica, axial CT or MRI images can be appropriately used to measure the true angle of abduction. However, because hips are immobilised in varying degrees of hip flexion, it is critical to understand that reliance on axial imaging alone commonly fails to produce an accurate assessment of in-spica hip abduction.
Orthopaedic surgeons generally recognise the need for orthogonal views to fully assess a fracture, and they appreciate that the maximum deformity often lies in its own unique plane. 19 Although the concept of the plane of maximal deformity is well recognised in orthopaedic fracture care, this tenet has not yet been applied to measuring the true position of a hip in spica. However, relying on only axial images for abduction measurements is analogous to estimating the angulation of a long bone fracture using only one radiographic view. We have shown that, just as in evaluating a fracture, two orthogonal views of the hip should be used to appreciate the true position of the hip joint.
In this study, we identified a fundamental inaccuracy in the traditional method of measuring hip abduction using axial imaging from post-reduction CT or MRI studies. We then sought to describe an accurate method for measuring this angle. To this end, we first precisely defined the true angle of hip abduction as the smallest angle between the femoral axis and a sagittal plane. We then derived an equation that uses measurements from both coronal and axial imaging to calculate the true abduction angle when hip flexion is between 0° and 90°. When we applied both the traditional and our novel hip abduction measurement methods to the study cohort, we found that an alarming proportion of measurements using the traditional method exhibited ≥ 10° of error. With hip flexion below 40° and decreasing, the risk of significant error (≥ 10°) with this method trended toward 100%.
Understanding the traditional method's tendency for error is important because it affects the classification of hips as over or under the generally accepted 55° to 60° safe upper limit of post-operative abduction in spica. With the cutoff set at 55° for this study's participants, 62.2% of hips measured at 55° to 65° using the traditional method (23/37) actually fell under that limit when our novel method was applied. With a cutoff of 60°, 100% of traditional measurements that fell between 60° and 70° (14/14) fell under the cutoff when the novel method was used. Thus, hips immobilised with axial projection angles slightly above the accepted abduction cutoff of 55° to 60° are likely casted with true abduction angles under this threshold. The presence of such uncertainty around this limit casts doubt upon its validity. If the threshold for safe abduction is 55° to 60° of true abduction, then we must recognise that a hip in a safe position may actually show a femoral shaft angle of > 60° on axial imaging. On the other hand, perhaps the accepted limit of 55° to 60° was itself overestimated due to inaccuracy in measurements during earlier research, and therefore the safe limit for true abduction is less than what has been described. More likely, there is a reasonable limit for safe abduction for each degree of hip flexion. As further work is necessary to establish these flexion-specific limits, it behoves future researchers to use accurate and consistent definitions for the true position of the hip in spica.
It is important to note that studies demonstrating a correlation between excessive abduction in spica and an increased risk of osteonecrosis have mostly involved patients undergoing closed reductions rather than open reductions. 20 In these cases, hip flexion often approximates 90° and radiographically measured abduction using traditional methods is relatively reliable. To our knowledge, however, the correlation between abduction and AVN has not been convincingly demonstrated following open reductions, in which the hip is typically immobilised in a relatively extended position. 21 Based on the findings of the present study, one potential reason for this may be that, in a more extended position, the hip is actually less abducted than axial images suggest and therefore at a lower risk for epiphyseal vascular compromise.
Our study has several limitations. While conceptually accurate, the novel method would benefit from validation by independent investigators. In addition, the method requires more time and the use of formulas. Although true abduction angles can be quickly calculated with commonly available software, such as spreadsheet programs, we recognise that adding complexity to measuring may be cumbersome in standard clinical practice. Even if our exact technique is not used in an everyday setting, it is worthwhile for those that treat DDH to have an appreciation for the general effect of decreasing hip flexion on the perceived angle of abduction in spica. Additionally, use of our novel method is reasonably justified in future clinical research as it is a more accurate measure of hip position.
In conclusion, we have described the development and testing of a novel method for measuring in-spica hip abduction using axial and coronal sequences on advanced imaging. Empiric and quantitative comparison of our new method with the traditional method of measuring abduction allowed us to describe systematic error embedded in the traditional method, especially for those hips that are immobilised in less than 90° of flexion. Given the improved accuracy and reliability of our novel method, we believe that it should be considered for any future work investigating the relationship between in-spica hip positioning after surgical reduction for DDH and the risk of developing osteonecrosis.
Footnotes
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
This retrospective study qualified as human subject research. It was IRB-approved. No funding was received for this study.