
Abstract
Purpose
To determine the influence of the time from injury to surgery of Type III supracondylar fractures on operative duration and quality of reduction.
Methods
A retrospective review of Type III supracondylar fractures treated by closed reduction and percutaneous pinning over a 3-year period was performed.
Results
The subjects were divided into two groups based on the time from injury to surgery (IST): Group 1 (<8 h) 48 subjects and Group 2 (>8 h) 39 subjects. There was no difference in the mean age or gender ratio between the two groups. There were no cases of compartment syndrome or conversion to open reduction in either group. The mean IST was 669 min. The mean IST for Group 1 was 340 min and it was 1,074 min for Group 2. The operative duration for Group 1 was 32.56 min and for Group 2 it was 31.72 min (P = 0.77). There were no significant differences in the quality of reduction.
Conclusions
There was no difference in the operative duration demonstrated between IST <8 h and IST >8 h. This failure to demonstrate a difference should not be interpreted as demonstrating equivalence. This study does not conclude that all displaced supracondylar fractures should be delayed, though it does inform the surgeon that, if compelled to delay surgery, this series did not demonstrate an increased risk of complications, nor a worsened quality of reduction.
Keywords
Introduction
Supracondylar fractures of the humerus are among the most common fractures in the pediatric population, and, yet, can present significant technical challenges [1]. These fractures are subdivided based on the degree of displacement, using the Gartland classification system [2]. The focus of our study is limited to Type III fractures, representing displaced fractures with no remaining cortical contact. The commonly accepted treatment for these fractures involves a closed reduction and percutaneous pinning [3]. Much has been studied and published on the topic of techniques for operative fixation, with persistent debate related to the number, direction, and configuration of pins [3]. Several studies have explored the definition of quality of reduction, ranging from Baumann angle to more complex indices [4–6]. Traditionally, these fractures have been treated as surgical urgencies, though recent research has cast doubt on this issue [7–10]. These studies demonstrated no influence of injury to surgery time (IST) on the outcome measures investigated (rate of open reduction, rate of complications, length of hospital stay, and clinical outcome). One other study has examined the issue of quality of reduction in relation to the timing of surgical intervention and found that delaying operations did not compromise the quality of reduction [11].
Purpose
In our study, we endeavored to elaborate on this previous work to determine if delaying surgical treatment might have an adverse impact on the surgeon's ability to obtain and maintain a reduction. The purpose of our study was to determine the influence of the time from injury to surgery of Type III supracondylar fractures on operative duration and the quality of reduction. We set operative duration as our primary outcome measure and our chosen quality of reduction parameters as our secondary outcome measures.
Methods
A retrospective chart review was performed for all Type III supracondylar humeral fractures treated with closed reduction and percutaneous pinning at our center over a 3-year period (2003–2006). Subjects were excluded by the following criteria: incomplete clinical information, incomplete or inadequate imaging, open fracture, vascular injury at presentation, or ipsilateral injury. All subjects that met the inclusion criteria for the study underwent a formal chart review to obtain the following information: date of birth, date of injury, time of injury, time of hospital presentation, staff surgeon, date and time of surgery, start and end time of surgery (as defined in the operative nursing records), pin configuration, and any complications.
A radiographic analysis of all films was carried out by two independent reviewers in a blinded fashion on two occasions, separated by 6 weeks. This analysis was performed using existing software on our digital imaging system. Intra-operative post-reduction and fixation fluoroscopic images were utilized. Parameters measured on the anterior–posterior images included: Baumann Angle (Fig. 1), proximal and distal fragment width (PFW-AP and DFW-AP, respectively), and medial and lateral translation (MT-AP and LT-AP, respectively). Parameters measured on the lateral images included: lateral humero-capitellar angle (Fig. 2) [12], proximal and distal fragment width (PFW-L and DFW-L, respectively), and anterior and posterior translation (AT-L and PT-L, respectively). Using these parameters, the following indices were calculated: Gordon Index ([AT-L/DFW-L] × 100) [5], Griffet Index 1 (DFW-L/PFW-L × DFW-AP/PFW-AP), and Griffet Index 2 ([Gordon index/10] + Griffet Index 1) [6].
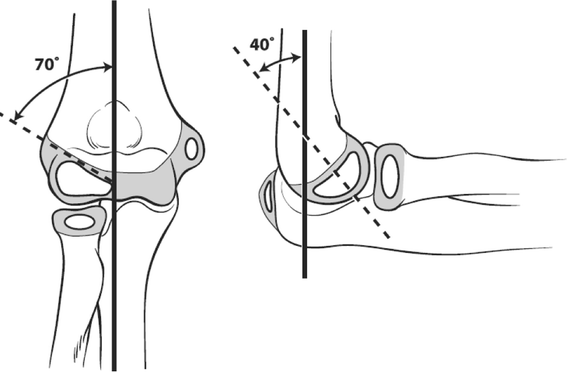
Baumann angle illustrated in both the anterior–posterior and lateral views
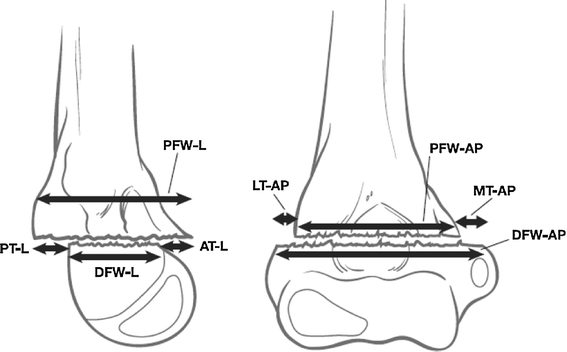
Fracture displacement measures for the humero-capitellar angle are illustrated in the lateral and anterior–posterior views. PFW-L proximal fragment width in the lateral view, PT-L posterior translation in the lateral view, AT-L anterior translation in the lateral view, DFW-L distal fragment width in the lateral view, LT-AP lateral translation in the anterior–posterior view, PFW-AP proximal fragment width in the anterior–posterior view, MT-AP medial translation in the anterior–posterior view, DFW-AP distal fragment width in the anterior–posterior view
Statistical analysis was performed using the Statistical Package for the Social Sciences (SPSS Version 17). Means and standard deviations were calculated for continuous variables. A P value of <0.05 was considered to be significant and confidence intervals were reported where appropriate.
Results
There were a total of 87 subjects after exclusion criteria were applied. These subjects were divided into two groups based on IST: Group 1 (<8 h) 48 subjects and Group 2 (>8 h) 39 subjects. The mean age for all subjects was 6 years and 1 month, with no significant difference between Group 1 and Group 2. There was no difference in the gender ratio between the two groups. Sixty subjects had been seen previously at another hospital, representing 52% of Group 1 (25 subjects) and 89% of Group 2 (35 subjects). There were no cases of compartment syndrome or conversion to open reduction in either group.
The mean IST was 669 min. The mean IST for Group 1 was 340 and it was 1,074 min for Group 2. The mean operative duration for all subjects was 32.18 min. The mean operative duration for Group 1 was 32.56 min and for Group 2, it was 31.72 min (P = 0.77) (Table 1). The mean difference between the two groups was 0.84, with a 95% confidence interval of −4.77 to 6.46.
Operative duration

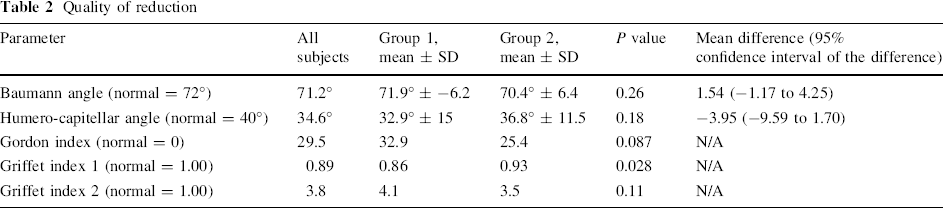
In terms of quality of reduction, a variety of parameters were measured and compared between the groups. The summary of this data can be found in Table 2. The mean Baumann angle for all subjects was 71.2°. When divided by group, Group 1 averaged 71.9° and Group 2 averaged 70.4° (P value = 0.26). The mean difference between the two groups was 1.54, with a 95% confidence interval of −1.16 to 4.25. The mean humero-capitellar angle for all subjects was 34.6°. When divided by IST, Group 1 averaged 32.9° and Group 2 averaged 36.8° (P value = 0.18). The mean difference between the two groups was −3.95, with a 95% confidence interval of −9.60 to 1.70. The mean Gordon Index for all subjects was 29.5. When divided by IST, Group 1 averaged 32.9 and Group 2 averaged 25.4 (P value = 0.087). The mean Griffet Index 1 for all subjects was 0.89. When divided by IST, Group 1 averaged 0.86 and Group 2 averaged 0.93 (P value = 0.028). The mean Griffet Index 2 for all subjects was 3.8. When separated by IST, Group 1 averaged 4.1 and Group 2 averaged 3.5 (P value = 0.11).
Quality of reduction
The intra- and inter-rater reliabilities were measured for the Baumann angle and the lateral humero-capitellar angle. The intra-rater correlation coefficient for the Baumann angle for rater 1 and rater 2 were 0.48 and 0.46, respectively. The inter-rater correlation coefficient was 0.83. The intra-rater correlation coefficient for the lateral humero-capitellar angle for rater 1 and rater 2 were 0.76 and 0.80, respectively. The inter-rater correlation coefficient was 0.46.
Table 3 demonstrates the impact of the individual surgeon on the IST and operative duration. When analyzed by individual surgeon, there were no significant differences in the mean operative duration between groups, nor the propensity to preferentially perform surgery in less than or greater than 8 h.
Operative duration by surgeon

Discussion
Building upon previous work, our study endeavored to establish that, beyond not causing harm, the quality and ease of reduction and fixation of these injuries were not being affected by surgical timing [3, 7–10].
The results demonstrate that there was no appreciable effect on the quality of reduction between our two groups. This was assessed using three separate radiographic parameters: Baumann angle, humero-capitellar angle, and Griffet index. Though there are weaknesses to any one of these individually as an assessment of the quality of reduction, we feel that, by using them as a group, we are capturing a quantitative measure of the reduction. Furthering this finding was that the operative duration did not differ between groups. Though there are many factors that are responsible for the operative duration (time of day, staff, trainee, surgeon, anesthesia, etc.), we found no difference between our two groups when stratified by time since injury. Using operative duration as a surrogate for the relative ease of reduction and fixation, we can conclude that a delay in treatment did not negatively influence this facet either.
In their series, Iyengar et al. [7] studied a consecutive series of 58 patients retrospectively. They selected 8 h as the definition of early versus delayed surgery. No difference was demonstrated in the rate of open reduction, and follow-up examination showed no clinical difference between the groups. Mehlman et al. [8] performed a retrospective, double-cohort study to evaluate the influence of early (<8 h) versus delayed (>8 h) treatment on post-operative complication rates. Their series included 151 Type III fractures. They found no significant difference between groups with respect to the need for open reduction and complications. They had no cases of compartment syndrome in either group. Leet et al. [9] performed a retrospective review of 158 Type III supracondylar fractures. They demonstrated no correlation between an increase in time to surgical intervention and longer operative time or the need to open the fracture site. They also concluded that there was no indication that the delay to surgical treatment resulted in longer hospital stay or an increase in unsatisfactory results. They found a mean IST of 21 h and 18 min. The average operative duration was 53 min. Gupta et al. [10] performed a retrospective review of supracondylar fractures. Of their series, 69 were Type III fractures. They demonstrated no significant difference in peri-operative complications or the rate of open reduction in children undergoing early (<12 h) versus delayed (>12 h) treatment. They recognized the limitations of the retrospective nature of their study and the selection bias that this could create.
The issue of quality of reduction was investigated in a more recent paper [11]. In this study, 42 patients were retrospectively divided into <8 h and >8 h from injury to surgery. This study found no difference in Baumann angle between the acute and delayed intervention. This study included both Type II (21 patients) and Type III (21 patients) supracondylar fractures. Unfortunately, the acute management group was biased towards Type III supracondylar fractures (64%), and the delayed group towards Type II fractures (71%). This bias alone could have explained the lack of differences in the quality of reduction. The only parameter for the quality of reduction was the Baumann angle. The findings from our study strengthen the conclusions of this important earlier work.
Ramachandran et al. [13] reported on the occurrence of compartment syndrome over a 10-year period. This study surveyed 50 pediatric orthopedic surgeons and reported in detail on the 11 cases of compartment syndrome that occurred in eight hospitals in three countries. The study was unable to determine the true incidence of compartment syndrome, as no denominator could be matched with the numerator. The study did find that ‘severe swelling’ and delay from injury to surgical treatment were consistent findings in their cases. This study highlights that the absence of a case of compartment syndrome in any series, including this one, might simply be due to an inadequate number of patients studied.
The limitations of this study must also be considered. The study is retrospective in nature, and creates inherent bias in the early versus delayed groups. There are many variables that cannot be controlled for in a retrospective study that would influence whether a patient was brought to the operating room urgently or in a delayed fashion. The imaging utilized to determine the quality of reduction was drawn from the intra-operative fluoroscopic images. Though these are clearly of lesser resolution and standardized technique than other imaging modalities, these are the images that are being used by the operating surgeon to judge and accept the reduction, and are, therefore, perhaps the most appropriate. The quality of reduction of supracondylar fractures has been demonstrated to not correlate directly with clinical outcome. In our study, we chose to interpret the quality of reduction as a surrogate of the ease of surgery when combined with the data of operative duration. The accepted effect of rotation on the Baumann angle has been well documented [14]. It is for this reason that we chose to utilize multiple parameters to minimize this confounding influence.
There was no difference in operative duration demonstrated between IST <8 h and IST >8 h. In addition, there was no difference in the quality of reduction demonstrated between the two groups. Previous findings of the rates of open reduction and major complications were replicated in this study. Correct interpretation of these results must consider the study design and the limits to the conclusions that can be drawn. Failure to show a difference between the two groups should not be interpreted as demonstrating equivalence. This study was powered for the primary outcome (operative duration) only, and the secondary outcomes (quality of reduction) are simply hypothesis generating.
The conclusions of this study may present a paradox to the surgeon when faced with the treatment of this fracture type in his or her practice. These findings add further data to the growing number of studies finding that delayed treatment of previously considered orthopedic urgencies may not result in worse outcome. It should be noted that, no matter what the time situation is regarding the initial presentation, each patient that presents with a Type III displaced supracondylar fracture needs to be assessed clinically upon presentation to be sure that those specific conditions requiring immediate emergency treatment are not present. It is important to clarify that this study does not conclude that the fixation of all displaced supracondylar fractures should be delayed. The data from this study does demonstrate that, if the surgeon is compelled to delay surgery, for whatever reason, there is no evidence to demonstrate harm. These findings are not meant to replace surgeon judgment in an individual clinical scenario.
Footnotes
Acknowledgments
The authors wish to acknowledge Mr. Stuart Almond for his assistance with the illustrations, Ms. Beverlie Ting for her assistance with the data collection, and Ms. Angeliki Kennedy for her support in preparing the final manuscript.