
Abstract
Abstract
Purpose
Cubitus varus deformity is one of the most common complications after displaced supracondylar humeral fractures in children. The purpose of this study was to evaluate the relationship between the fracture displacement and cubitus varus deformity in displaced supracondylar humerus fractures.
Methods
Seventeen patients (11 males/6 females; mean age 7 years) with cubitus varus deformities occurring after Gartland type III posteromedial or posterolateral displaced supracondylar humerus fractures were evaluated with clinical and serial radiographic examinations. All patients had been treated surgically by open reduction through a medial approach and percutaneous cross-pinning. All fractures were reduced anatomically. Ten of the patients were operated within the first 24 h. The time interval between the initial injury and the surgical procedure for the remaining seven patients was 5.3 days on average (range 2–10 days). The carrying angle and range of motion of the elbow were measured throughout the follow-up period. The mean follow-up time was 3.7 years (range 2–12 years).
Results
Five patients with type III-B fractures had a mean carrying angle loss of 8.8° (range 6–10°), whereas for the remaining 12 type III-A patients the mean loss was 15° (range 6–29°) (P = 0.019). None of the patients in this study demonstrated limited elbow motion. According to the Flynn criteria, the results were good in five type III-B patients. There was no statistically significant relationship between the loss of carrying angle and the delay before the surgical procedure (P = 0.615 in type III-A, P = 0.096 in type III-B).
Conclusions
The carrying angle loss was more significant in type III-A fractures compared with type III-B in this series. These results suggest that although anatomic reduction has been achieved by surgical treatment without loss of reduction, there is still a risk for cubitus varus deformity for type III-A fractures due to the initial compression of the medial column or, in other words, physeal injury.
Introduction
Displaced supracondylar fractures of the humerus in children are associated with several complications; cubitus varus deformity is the most common angular deformity after these injuries [1, 2]. Although use of percutaneous techniques has reduced the incidence of cubitus varus deformity significantly, 5–10% of children with supracondylar humerus fractures still develop this deformity irrespective of the treatment [3].
The pathogenesis of angular deformities of the elbow after supracondylar fractures of the humerus is obscure. Most of the studies in the literature conclude that the deformity can be a result of malunion, which includes medial tilting in the coronal plane, extension in the sagittal plane and internal rotation of the distal fragment in the horizontal plane [4–9]. Other studies suggest that growth disorders of the distal humeral physis induced by the fracture itself may cause cubitus varus [10–14].
The aim of this retrospective study was to investigate whether there was a correlation between the displacement of the fracture and cubitus varus deformity in displaced supracondylar humerus fractures treated surgically by medial open reduction and percutaneous fixation.
Materials and methods
Three hundred and nineteen patients with displaced supracondylar humerus fractures were treated at the Department of Orthopaedics and Traumatology of Ministry of Health Goztepe Training and Research Hospital between January 1992 and August 2003. All had complete radiographic documentation from the time of the fracture to healing. Two hundred and thirteen patients who were operated for displaced extension type of fractures by medial open reduction and percutaneous fixation were evaluated and only those patients who had cubitus varus deformity, as defined by a loss of carrying angle of more than 5° compared to the contralateral side according to Flynn's criteria [3], were included in the study. All of these fractures classified as type III (no cortical contact between proximal and distal fragments) according to Ref. [15]. Exclusion criteria were age greater than 18 years, open fracture, nondisplaced fracture, metabolic bone disease, a dysvascular extremity, and ipsilateral upper extremity fracture. The study group consisted of 17 (11 males, 6 females) patients. The average age at fracture was seven years (range 1–11 years).
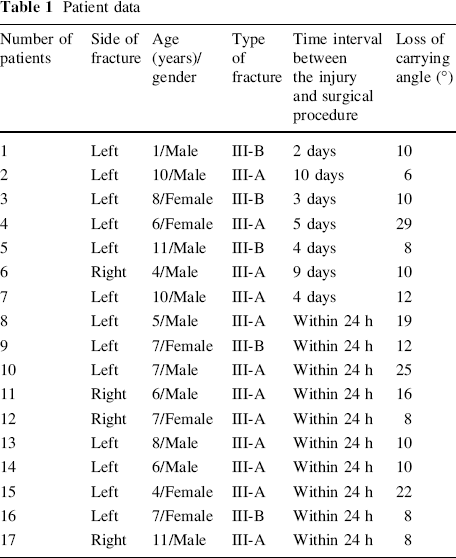
Preoperative radiographs were evaluated to determine the displacement of the fractures in the posteromedial (type III-A) or posterolateral (type III-B) direction according to Wilkins modification of the Gratland classification [2] (Fig. 1). Twelve patients (70%) had Gartland type III-A and the remaining five (30%) had Gartland type III-B fractures (Table 1). Ten of these patients (60%) were admitted to our hospital initially and operated within the first 24 h. Due to lack of a C-arm machine in the operating room, the patients received a surgical treatment consisting of manual reduction through a medial approach and percutaneous cross-pinning. The time interval between the initial injury and the surgical procedure for the remaining seven patients (40%) was 5.3 days on average (range 2–10 days) (Table 1). These patients were seen in another medical center initially and then operated in our hospital by the same surgical procedure (Fig. 2). Postoperatively, a posterior long-arm splint was applied to all children for 3–4 weeks according to the radiographic healing. In patients that had exact healing radiographically at the end of the third postoperative week, the K-wires and splint were removed and range-of-motion exercises were started. For the others both splint and the K-wires were removed at the end of fourth postoperative weeks.
Ten-year-old boy fell from a bicycle and sustained an injury of the left elbow. The plain anteroposterior and lateral radiographs showed type III-A displaced supracondylar humerus fracture at the time of injury
Patient data

He was referred to our hospital four days after the initial injury due to the failure of close reduction. He was operated by medial open reduction and percutaneous cross-K-wire fixation. Acceptable anatomic reduction can be seen on the postoperative anteroposterior and lateral radiographs
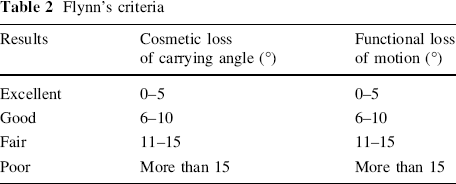
None of these patients had loss of reduction during the treatment period. Clinical evaluation at final follow-up was based on the measurements of range of motion of the elbow, all of which were compared with analogous measurements on the contralateral side. The radiographic examination included an anteroposterior and a lateral radiograph of the elbow. To determine cubitus varus deformity, the carrying angle was measured on the anteroposterior radiographs between the lines through the mid-points of the distal part of the humeral shaft and the proximal part of the ulna (Fig. 3). All clinical and radiological assessments at final follow-up were made by two independent orthopaedic surgeons (MG and BE). The long-term results were graded according to Flynn's criteria as good, moderate, or poor; taking into consideration the range of motion of the elbow and the carrying angle (Table 2).
He had full range of motion on the left elbow four years postoperatively. The anteroposterior radiograph showed carrying angle loss of 12° on the left elbow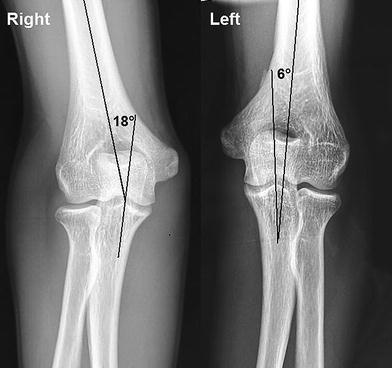
Flynn's criteria
Statistical analysis was performed by using “SPSS 14.0 for Windows Evaluation Version” software. The relationship between the carrying angle loss and fracture type was analyzed using the Student's t and Mann–Whitney U tests. A P < 0.05 was considered to be statistically significant.
Results
The average follow-up time was 3.7 years (range 2–12 years). Except for one patient (6%) with anterior interosseous nerve injury, which resolved spontaneously within three months postoperatively, none of the patients had neurological involvement before and after the operations. Pin tract infection that was resolved with oral antibiotics and pin removal after adequate osseous healing developed in another one patient in the second postoperative week. None of the patients in this study demonstrated limited elbow motion at final follow-up.
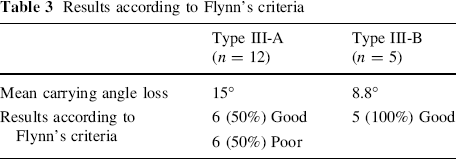
Five patients with type III-B fractures had a mean carrying angle loss of 8.8° (range 6–10°) whereas for the remaining 12 type III-A patients the mean loss was 15° (range 6–29°). There was statistical difference between the patients with type III-A and type III-B fractures with regard to carrying angle (P = 0.019). According to the Flynn criteria, the results were good for all type III-B patients. Results were good for six patients (50%) with type III-A fractures and poor for the remaining six (50%) (Table 3). There was no statistically significant relationship between loss of carrying angle and the delay before the surgical procedure (P = 0.615 in type III-A, P = 0.096 in type III-B).
Results according to Flynn's criteria
Discussion
Cubitus varus is the most common angular deformity following supracondylar humerus fractures in children [1, 2]. The incidence of this deformity in patients treated primarily by closed reduction and cast application alone ranges from 9 to 58% [2]. However, surgical treatment has had a marked effect on decreasing the incidence of this deformity. In a large comparative study by Pirone et al. [16], the incidence of cubitus varus with only cast immobilization following closed reduction was 14% versus 3% in those stabilized with percutaneous pins.
The etiology of cubitus varus deformity is still unclear. Several theories have been considered. Most of the authors believed that malreduction, rotation, or medial tilting of the distal fragment, or both, were the major causes of this deformity [4–9]. Others have reported that growth disturbances of the cartilaginous complex of the distal end of the humerus induced by the fracture itself may cause varus deformity [10–14]. Kim et al. [11] reported their long-term follow-up regarding children who developed trochlear deformities following distal humeral fractures, with radiographic and magnetic resonance imaging findings. Cubitus varus deformity developed in all of these patients with trochlear deformity, and although no progression was observed after 3–4 years it persisted until maturity.
Weiland et al. [9] reported 25% cubitus varus deformity in their series consisting of patients treated surgically by open reduction with lateral approach. They concluded that inadequate reduction with medial angulation was associated with residual cubitus varus deformity and the factors contributing to poor reduction were related to the surgical technique, in which only the lateral cortex was visualized directly. Several results of different surgical approaches to cubitus varus deformity have been reported in the literature. Smith [7] reported cubitus varus deformity in up to 57% of cases which were operated by open reduction through a medial approach. Lal and Bhan [17] reported the incidence of this deformity as 35% with posterior approach.
None of our patients had loss of reduction during the treatment and follow-up periods. Although anatomic reduction was achieved in all patients with medial open reduction, type III-A fractures with posteromedial angulation had statistically significant loss of carrying angle (P < 0.05). Devnani [18] reported results for 28 children with late presentation of displaced supracondylar humeral fractures. Seven patients with type III-A supracondylar humeral fractures had cubitus varus deformity in their series. However none of their patients with posterolateral displacement had this deformity.
Once the elbow achieved full extension and the severity of the varus deformity was appreciated, there was no evidence of any further increase in the deformity [2]. However there are isolated reports in the literature of progressive cubitus varus following a supracondylar fracture [10, 14]. Ippolito et al. [10] searched for a correlation between the angular deformity at follow-up and the adequacy of reduction. The authors presented a long-term follow-up (22 years) into young adulthood and found that the carrying angle remained the same in 18 patients, decreased in 22, and increased in 13 compared with the value present at the time of initial fracture healing several weeks after the injury. Malrotation of the distal fragment of the fracture only rarely caused medial tilting of the fragment with subsequent cubitus varus. The authors concluded that this indicated there was a potential for growth imbalance of the physis of the distal humerus. Theruvil et al. [14] published a case report of radiologically proven growth arrest due to a bony bar causing progressive cubitus varus deformity.
The reported incidence of cubitus varus deformity in some studies that included patients with delayed treatment of displaced supracondylar humerus fractures varied between 18 and 35% [17, 18]. Seven patients (40%) in our study had a mean delaying time of 5.3 days (range 2–10 days), but we were unable to identify any statistically significant relationship between the loss of carrying angle and the delay before the surgical procedure (P = 0.615 in type III-A, P = 0.096 in type III-B).
Although extension type of supracondylar humerus fractures are mostly accepted as pure hyperextension injuries [2], we think that hyperextension following an initial extension with unilateral medial compression is a more accurate description of some of these fractures. This mechanism is particularly valid for fractures with posteromedial displacement in which compression of the medial column is more likely. Our study indicates that type III-A supracondylar humeral fractures give cubitus varus deformity to a greater extent than other types of fracture, because of temporary interruption of blood supply to the medial column or physeal injury.