
Abstract
Abstract
Purpose
In this study the course of unstable hips after successful treatment with Fettweis plaster of Paris (POP) is examined. Special focus will be given to age at beginning of treatment and initial hip type.
Methods
The development of 93 unstable hips treated between November 2001 and April 2015 was examined. Inclusion criteria were: 1) unstable hips with successful treatment with Fettweis POP; 2) presence of two pelvic radiographs (12 to 24 months and 24 to 48 months). We analyzed: 1) the initial ultrasound hip type according to Graf; 2) the average age at first and second radiograph; 3) the Tönnis classification: normal findings (< 1 SD), slightly (1 SD to 2 SD) and severely dysplastic hips (> 2 SD).
Results
In all, there were 14 hips type D, 41 hips type III and 38 hips type IV. Mean age of the first radiograph was 13.9 months and of the second 28.5 months. The first radiograph showed: (< 1 SD): 36, (1 SD to 2 SD): 34, (> 2 SD): 23 hips, the second radiograph: (< 1 SD): 33, (1 SD to 2 SD): 19, (> 2 SD): 30 hips. With subdivision at the start of treatment at age eight or fewer weeks 2/16 hips (12.5%) and with initiation of the treatment more than eight weeks 22/77 (26.0%) deteriorated. During the course between first and second radiograph a total of 35.7% of initial hip type D, 19.5% of type III and 23.7% of type IV deteriorated.
Conclusion
Radiograph controls after treatment with Fettweis POP show poorer outcome after delaying the start of treatment more than 8 weeks. These findings were independent of the initial ultrasound hip type. Regular radiograph controls of all hip types treated for unstable hips are justified to detect residual dysplasia.
Level of evidence
IV
Introduction
Developmental dysplasia of the hip (DDH) is the most common hip disorder in children.1–3 The incidence varies from 1 to 34/1000 births depending on different diagnostic standards and methods. Furthermore, the prevalence in Central Europe and Asia is higher in comparison with African countries.4–6 Recognized risk factors for DDH are: 1) breech position; 2) family history; 3) oligohydramnion; 4) female gender; 5) firstborn; and 6) presence of musculoskeletal diseases e.g. club foot.5,7,8 A genetic influence is currently discussed. 9
Clinical as well as ultrasound examinations are proven methods for early diagnosis.10–12 In several European countries the ultrasound examination according to Graf is part of the ‘well-baby-program’ or used as selective diagnostic tool. According to Graf, the ultrasound findings are basic for classification and allow differentiation between stable but immature and dysplastic hip types (I–II stable) and unstable hip types (D, III, IV). 13
Stable hips are regularly controlled by clinical and ultrasound examination and/or treated with various splints e.g. the Tübingen splint. 14 In the treatment of unstable hips, plaster of Paris (POP) in human position e.g. the Fettweis POP or splints e.g. the Pavlik harness, have been proven successful as treatment tools.15–18 Under certain conditions unstable hips can be successfully treated with the Tübingen splint.19,20.All therapies are based on the principle: 1) reduction; 2) retention; and 3) maturation.
The Fettweis POP – which is used in the present study – was developed in 1968. 15 The application is carried out under short anesthesia. Prior to the application of the plaster the concentric reduction and safe position, normally in 90° to 100° flexion and 40° to 50° abduction, can be checked by arthrography. In more severe cases (especially in hip type IV), previous treatment with overhead extension for about two to three weeks may become indicated. 21 After plaster application the corrected hip position is checked by various imaging procedures e.g. MRI examination.22,23 Following the treatment with the Fettweis POP, further therapy with various splints or bandages is necessary until a transfer into a clinical and ultrasound stable hip type I is achieved.
Standard anterior-posterior pelvic radiograph controls can be indicated from the age of six months. From this age on, ultrasound imaging is more difficult due to increased ossification of the cartilaginous precursors.24–26 However, in many protocols radiograph controls are not conducted under the age of 12 months in order to reduce exposure to radiation.
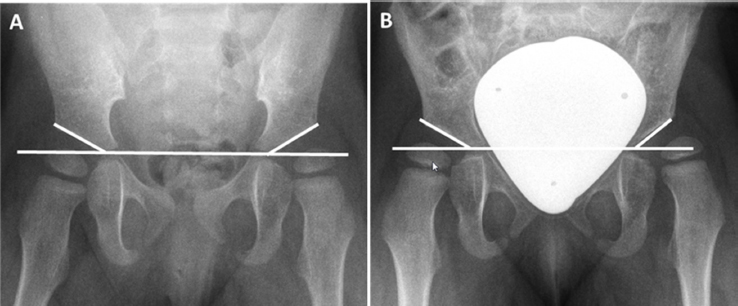
For evaluation of radiograph controls various lines and angles are used (Fig. 1). Here the acetabular (AC) angle is a parameter used to evaluate DDH. The AC angle is measured along the Hilgenreiner line and the AC roof. Based on these findings, the classification and evaluation of DDH according to Tönnis is established. With consideration of age, gender and affected side the Tönnis classification distinguishes between normal findings (< 1 sd), slightly dysplastic (1 sd to 2 sd) and severely dysplastic (> 2 sd) hips.2,27
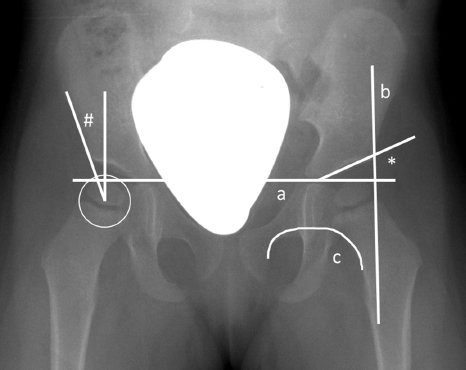
Pelvic radiograph of a two-year-old girl: (
The formerly valid thesis that a ‘normal’ hip after successful treatment does not deteriorate with growth is more and more called into question and regular radiograph controls are recommended until cessation of growth. In this study we therefore examined the course of unstable hips which were successfully treated with Fettweis POP with respect to the initial ultrasound hip type and age at diagnosis and treatment.
Patients and materials
Patients
From November 2001 to April 2015, 104 consecutive children with 132 unstable hip joints were treated with the Fettweis plaster at our institution. The treatment protocol is shown in Fig. 2.
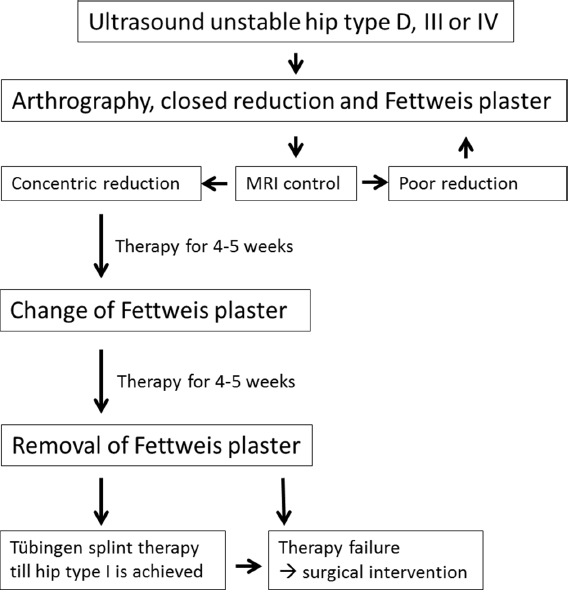
Treatment protocol of unstable hips type D, III and IV with Fettweis plaster.
Inclusion criteria for this retrospective study were 1) unstable hip according to Graf that were successfully transferred into an ultrasound stable hip type I by treatment with the Fettweis POP followed by treatment with the Tübingen splint; and 2) presence of routine pelvic radiograph controls at the age of 12 to 24 months and 24 to 48 months.
Children with secondary hip dysplasia, e.g. infantile cerebral palsy, spina bifida or other neurological diseases, were excluded.
Methods
Classification and evaluation of the hip joints was based on routine pelvic radiograph controls at the age of 12 to 24 months and 24 to 48 months of children after successful treatment with the Fettweis plaster and afterwards with the Tübingen splint until transfer into an ultrasound stable hip type I is reached. Evaluation focused on: 1) initial ultrasound hip type according to Graf; 2) average age at first and second radiograph control; and 3) determination of the AC-index according to the Tönnis classification 2 and evaluation into: normal findings (< 1 sd), slightly dysplastic findings (1 sd to 2 sd) and severely dysplastic findings (> 2 sd).
Further avascular necrosis of the femoral head (AVN) was classified according to Kalamchi and MacEwen into type I to IV. 28
All measurements were performed by two different physicians (HK and JPH) who were blinded to the patients’ diagnosis.
Statistical analysis
Results are presented as mean ± SEM using SPSS Statistics Version 23 (IBM Corp., Armonk, New York).
Results
In all, 75 children with 93 unstable hip joints (18 bilateral) were included. There were 14 (15.1%) hips with initial hip type D, 41 (44.1%) with hip type III and 38 (40.9%) with hip type IV. In all, 63/75 (84%) of the children were female.
Radiograph results of all patients
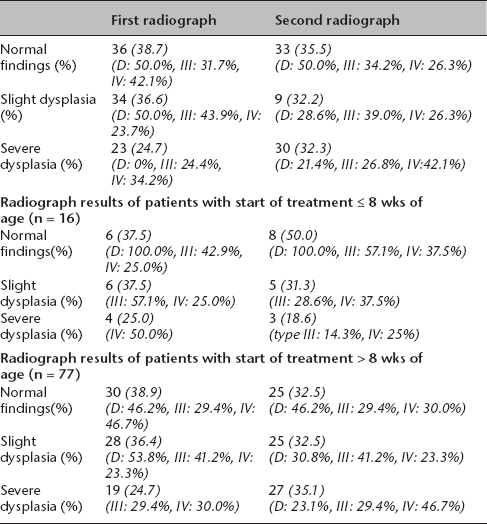
The first routine pelvic radiograph was conducted at a mean age of 13.9 months (sd 2.7, 9 to 22, n = 93) and the second radiographic control was conducted at a mean of 28.5 months (sd 6.1, 21 to 48, n = 93).
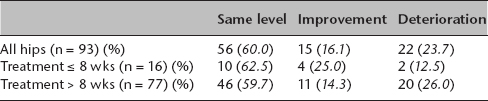
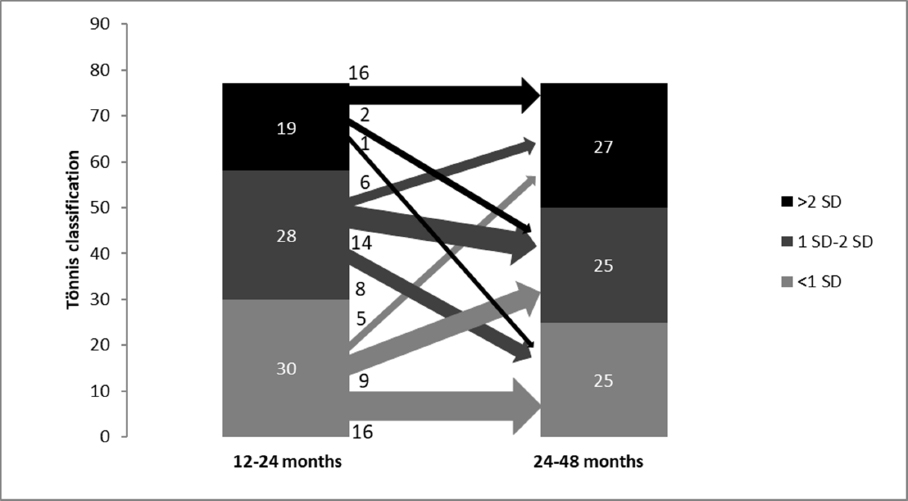
In comparison between the first and second time point, 22/36 hips (61.1%) with normal findings showed constant normal findings, 9/36 hips (25.0%) deteriorated into slightly dysplastic hips and 5/36 into severely dysplastic hips (13.9%). Overall, 9/34 of formerly slightly dysplastic hips (26.5%) improved into normal findings, 17/34 stayed slightly dysplastic (50.0%) and 8/34 deteriorated into severe dysplasia (23.5%). Overall, 17/23 of previous severely dysplastic findings (73.9%) showed constant severe dysplasia, 2/23 improved to normal findings (8.7%) and 4/23 to slight dysplasia (17.4%) (Fig. 3). A total of 15/93 hips (16.1%) improved, whereas 22/93 hips (23.7%) deteriorated (Table 1).
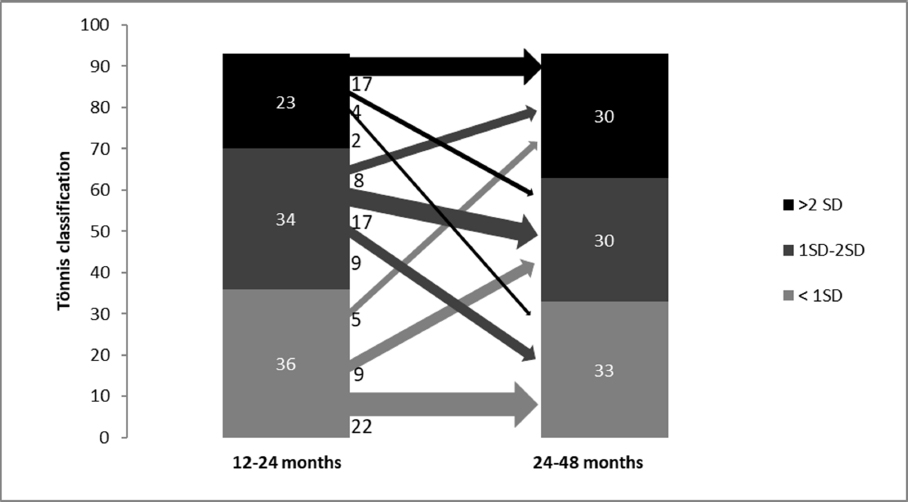
Comparison of 12 to 24 months versus 24 to 48 months, n = 93, improvement of nine slightly dysplastic hips and two severely dysplastic hips into normal findings, four severely dysplastic hips into slightly dysplastic hips, deterioration of nine normal findings into slightly dysplastic hips and five severely dysplastic hips, eight slightly dysplastic hips into severely dysplastic hips.
Comparison first versus second radiograph based on start of treatment (all hips (n = 93), treatment at eight or less weeks of age (n = 16) and more than eight weeks of age (n = 77)).
Radiograph results of patients with start of treatment at age eight or less weeks
According to IBM SPSS Statistics Version 23, the turning point from which improvement of the hips could be observed was calculated at eight weeks of age.
In 16 cases (hip type D: 1, III: 7, IV: 8) the treatment with Fettweis plaster started eight or less weeks of age. The mean age was 39.7 days (sd 9.1, 23 to 54).
The first pelvic radiograph was taken at a mean age of 14.0 months (sd 2.3, 12 to 22), the second radiograph was conducted at a mean of 29.1 months (sd 6.8, 24 to 48). In comparison with pelvic radiograph controls in the second year of life versus 24 to 48 months, there was total increase of normal findings of 33.3%. Overall, 6/6 hips (100%) with normal findings showed constant normal findings, 1/6 slightly (16.7%) and 1/4 severely dysplastic hip (25.0%) improved into normal findings. A decrease of 16.7% of slight dysplasia was seen. Here 3/6 were still slightly dysplastic (50.0%). Overall, 1/6 hips (16.7%) improved into normal findings and 2/6 hips (33.3%) deteriorated into severe dysplasia (hip type III and IV). Overall 1/4 hips (25.0%) with severe dysplasia showed constant severely dysplastic findings. Overall, 2/4 (50.0%) improved into slightly dysplastic findings and 1/4 (25.0%) into normal findings (total decrease of severe dysplasia of 25%) (Fig. 4). Here, a total of 4/16 hips (25.0%) improved, whereas 2/16 hips (12.5%) deteriorated (Table 1).
Comparison of 12 to 24 months versus 24 to 48 months, n = 16, improvement of one slightly dysplastic hip and one severely dysplastic hip into normal findings, two severely dysplastic hips into slightly dysplastic hips, deterioration of two slightly dysplastic hips into severely dysplastic hips.
Radiograph results of patients with start of treatment at more than eight weeks of age
There were 77 unstable hips (hip type D: 13, III: 34, IV: 30) which were treated with Fettweis POP after the eighth week of life. Mean age was 115.7 days (sd 58.4, 57 to 331).
The first radiograph control was conducted at a mean age of 13.8 months (sd 2.8, 9 to 20) and the second control was at a mean age of 28.3 months (sd 5.9, 21 to 48).
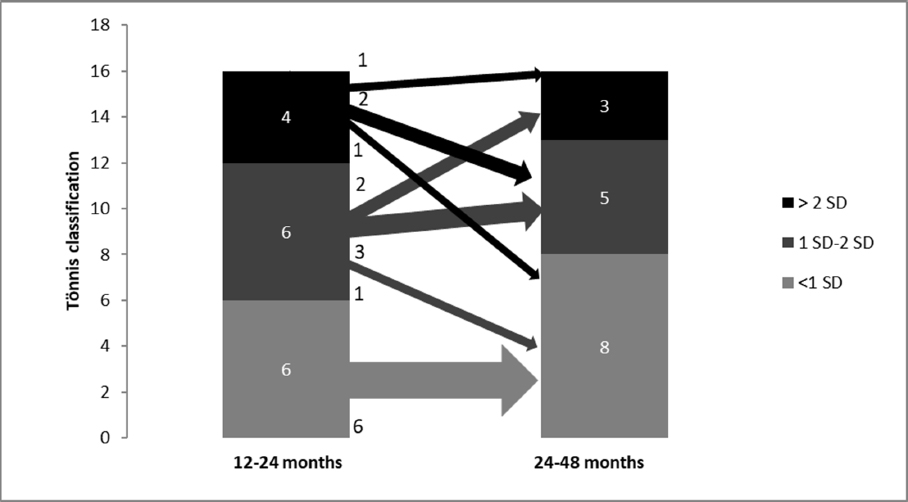
In comparison of the two time points a decrease of normal findings of 16.7% were seen. Here 16/30 hips (53.3%) with normal findings in the first control showed constant normal findings, 9/30 (30.0%) deteriorated into slight dysplasia and 5/30 (16.7%) into severe dysplasia. The number of slightly dysplastic hips was decreased by 10.7%. Overall, 8/28 hips (28.6%) improved into normal findings, 14/28 (50.0%) showed constant slight dysplasia and 6/28 (21.4%) deteriorated into severely dysplastic hips. A total increase of 42.1% of severely dysplastic hips was seen. Here 16/19 hips (84.2%) were constantly severely dysplastic, 2/19 (10.5%) improved into slight dysplasia and 1/19 into normal findings (5.3%) (Fig. 5). A total of 11/77 hips (14.3%) improved, whereas 20/77 hips (26.0%) deteriorated (Table 1).
Comparison of 12 to 24 months versus 24 to 48 months, n = 77, improvement of eight slightly dysplastic hips and one severely dysplastic hip into normal findings, two severely dysplastic hips into slightly dysplastic hips, deterioration of nine normal findings into slightly dysplastic hips and five severely dysplastic hips, six slightly dysplastic hips into severely dysplastic hips.
Radiograph results in relation to initial ultrasound hip type
Our data show that the radiological development of all hips is independent of the initial ultrasound hip type at diagnosis and despite a successful transfer into an ultrasound hip type I.
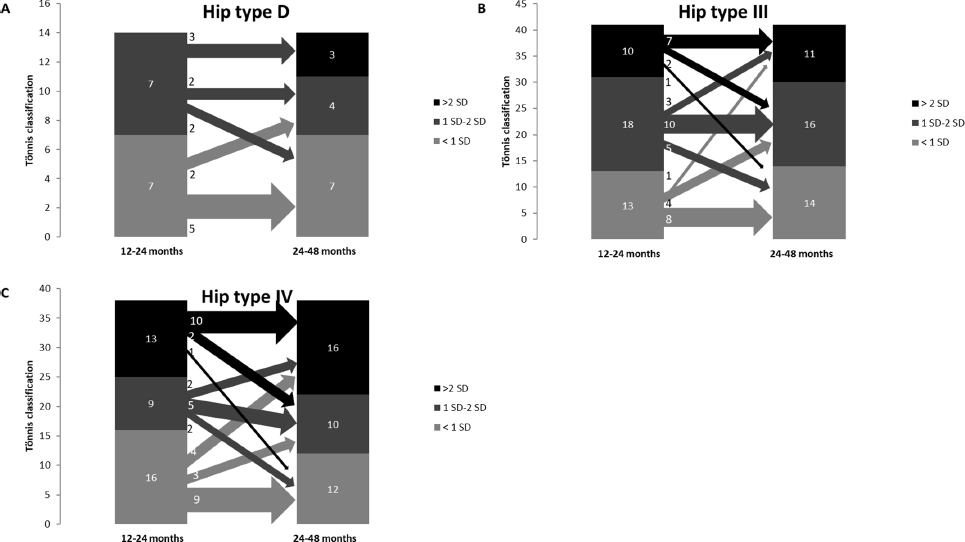
Initial hip type D (n = 14): 5/7 normal findings (71.4%), show constant normal findings, but 2/7 deteriorated into slight dysplasia (28.6%). Overall, 2/7 slightly dysplastic hips improved into normal findings (28.6%), 2/7 were constantly slightly dysplastic (28.6%) and 3/7 slightly deteriorated into severe dysplasia (42.9%) (Figs 6a and 7, Table 2).
Comparison of 12 to 24 months versus 24 to 48 months: (
(
Comparison first versus second radiograph based on initial hip type (type D (n = 14), type III (n = 41), type IV (n = 38))
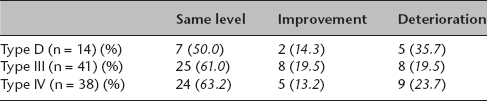
Initial hip type III (n = 41): 8/13 of normal findings were constant normal (61.5%), 4/13 deteriorated into slight dysplasia (23.1%) and 1/13 into severe dysplasia (7.7%), 5/18 of slightly dysplastic hips improved into normal findings (27.8%), 10/18 were constantly slightly dysplastic (55.6%) and 3/18 deteriorated into severely dysplastic hips (16.7%). Overall, 1/10 initial severely dysplastic hips improved into normal findings (10.0%), 2/10 into slight dysplasia (20.0%) and 7/10 showed constant severe dysplasia (70.0%) (Fig. 6b, Table 2).
Initial hip type IV (n = 38): 9/16 show constant normal findings (56.3%), 3/16 deteriorated into slight (18.8%) and 4/16 into severe dysplasia (25.0%). Overall, 2/9 slightly dysplastic findings improved into normal findings (22.2%), 5/9 were constantly slightly dysplastic (55.6%), 2/9 deteriorated into severe dysplasia (22.2%). Overall, 1/13 severely dysplastic findings improved into normal findings (7.7%) and 2/13 into slight dysplasia (15.4%). Overall, 10/13 were constant severely dysplastic (76.9%) (Fig. 6c, Table 2).
AVN of the femoral head
AVN type I and II according to the Kalamchi and MacEwen types were seen in five cases (5.4%) (hip type III: 2, IV: 3).
Operative interventions
In eight hips (8.6%) an operative correction (Salter osteotomy) was conducted after the second radiograph control (hip type III: 4, IV: 4) and in another 13 cases (14.0%) a surgical intervention was recommended (hip type D: 1, III: 7, IV: 5).
The exact information on the results can be found in Table 3.
Radiograph results of all patients (n = 93)
Discussion
For early detection and classification of DDH general screening methods including ultrasound examinations are accepted and well established in European countries 11,29. However, in some Anglo-American countries an ultrasound examination is only performed in children with risk factors such as breech position or family history. Here the opponents of general ultrasound screening discuss exaggerated diagnostics.30–32 However, both – Anglo-Americans and Europeans – have consensus that early diagnosis and treatment are crucial to prevent progression of the dysplasia and lead to beneficial outcome for the children. Our data confirm this hypothesis. To the best of our knowledge, this is the first study that examined in detail the development of initially unstable hips treated with Fettweis POP with respect to initial ultrasound hip type and age. Our results clearly show that start of treatment with reduction of the hip and retention in the Fettweis POP at age eight weeks or less show better outcome with increase of normal findings and decrease of slightly respectively severely dysplastic findings in comparison with the results with start of treatment at more than eight weeks of age. Here, the radiological results deteriorate after the first radiograph control in all classifications according to Tönnis although an ultrasound hip type I has been achieved after treatment with Fettweis plaster and afterwards with the Tübingen splint. Our results confirm other studies, which show deteriorating findings after treatment with other treatment modalities, e.g. Pavlik harness.33–35 We support the conclusion that regular controls are recommended until cessation of growth.
Interestingly, the radiograph results show that the unpredictable development with, on one hand improvement and on the other hand, deterioration of hips, is independent of the initial ultrasound hip type at diagnosis and independent of successful transfer into an ultrasound hip type I. Even hips with initial hip type D deteriorated into severely dysplastic hips. This further indicates that regular radiograph controls seem to be mandatory to detect deterioration over time and need to be early enough to indicate and perform operative improvement of AC orientation. These findings support those of other studies which use other treatment modalities e.g. Pavlik harness or Tübingen Splint and recommend further radiograph controls as well.25,36–39 However, so far, there is no standard algorithm for control examinations after successfully treated DDH. 6 Some authors also recommend other control examinations such as ultrasound and CT.40,41
Our examinations show a total of 5.4% AVN after the second radiograph control. These findings are confirmed by other studies that have also a low rate of AVN after treatment with Fettweis POP.42,43 In contrast, other treatment modalities, e.g. Pavlik harness, show a slightly higher rate of AVN.35,44,45 Comparisons between the different studies are known to be limited because of diagnostic criterias, e.g. study groups with different age at diagnosis, age at beginning of treatment, different classification and different control time points.
Limitations of our study include the fact that it was a non-randomized trial and the small number of the group with treatment starting at eight or less weeks of age (n = 16).
We demonstrate for the first time, that radiograph controls after successful treatment of unstable hips with Fettweis plaster with transfer into an ultrasound stable hip show poorer outcome after delayed start of treatment at more than eight weeks of age compared with a start at eight or less weeks of age. Interestingly, the development of the hips seems to be independent of the initial ultrasound hip type. Regular radiograph controls of all hip types seem to be justified to detect residual dysplasia.