
Abstract
Purpose
To collect and describe data on the natural history of abnormal ultrasound (US) findings in hips of infants under six months of age to serve as a reference to the design of screening programmes and treatment algorithms in the care for children with hip dysplasia.
Methods
A search in PubMed of the terms “DDH” and “ultrasound” was done to find hips with abnormal US findings that were not treated. In cases of multiple periods of follow-up, the classification of every period was evaluated separately (individual hip follow-up periods).
Results
Data of 13 561 hips with 16 991 follow-up periods were collected and analyzed. Most quantifiable classifications and follow-up periods were according to Graf (14 876) and a minor number of the hips had follow-up periods with femoral head coverage (FHC) (2115). Normal development without treatment in the first six months was for Graf 2a between 89% and 98%, for Graf 2c between 80% and 100% and for clustered data Graf 2a to 2c between 80% and 97%. For Graf 3 hips more than 50% were reported to develop into normal hips without treatment. As for Graf 4 hips this percentage was reported below 50%. For children with an FHC less than 50%, normalization was reported between 78% and 100%.
Conclusion
The natural history of developmental dysplasia of the hip (DDH) shows a benign course, especially in the well-centered hips. This outcome probably contributes to the fact that all studies on US screening of hips for detection of relevant DDH in order to improve outcomes of treatment are rated as substantially underpowered.
Keywords
Introduction
Osteoarthritis of the hip is one of the major burdens of disease, with a wide spectrum ranging from the quality of life of the individual patient to global economic costs. The incidence rate is around 16% at around the age of 45 years, rising to 25% to 40% in people over the age of 75 years.1–3 Early osteoarthritis of the hip is associated with hip dysplasia in early childhood. The consequences of hip dysplasia depend on its severity. Hip dysplasia with persistent subluxation of the femoral head has the highest risk for developing early painful hip osteoarthritis between the ages of 20 to 50 years and can already be present shortly after skeletal maturation in cases of severe subluxation. 4
The relationship between hip dysplasia in childhood and its related short-term and long-term morbidity is one of the motives for the development of screening programmes for hip dysplasia in the first weeks after birth. Well-known tests for diagnosing hip dysplasia after birth by physical examination, like Ortolani 5 and Barlow 6 , were developed in the first and second half of the last century and are still practised today.
The limitations of radiographic depiction of the hip, due to the absence of the ossific nucleus in the first months after birth, have been combatted by ultrasound (US), and this method has become popular since the first paper describing it by Graf in 1980. 7 The cartilaginous anatomy of the hip can clearly be outlined sonographically. Since then many other authors have published results in more than ten different classification systems. 8 The most frequently used classifications are the static method of Graf, the stability test by Harcke 9 and the femoral head coverage (FHC) by Morin et al 10 and Terjesen et al 11 and combinations of these methods as published by Rosendahl and Toma. 12 The alfa and beta angle by Graf and the FHC by Morin and Terjesen produced quantifiable parameters. The classifications from these methods are aiming at defining the different grades of hip dysplasia and providing a prognosis for its sequelae. Although a hip dislocation can clearly be diagnosed, classifications for hip dysplasia and subluxation vary. The borders of the categories in these classifications are made by the authors on the basis of their experience or on consensus in expert panels. Differences in image acquisition and interobserver variation can significantly influence the diagnosis in the border zones between the different categories of the classifications. Diagnosing relevant hip dysplasia in the first months of life does not meet the World Health Organization standards since seven of the 11 criteria cannot be not met. 13 Cochrane and other high-quality reviews conclude that diagnosis by US is ‘highly sensitive but poorly specific’, and that it is not clear how much unnecessary treatment is instituted today due to the lack of a benchmark for diagnosis. 14 For stable hip dysplasia it is even questionable if the current treatment alters the natural history of the development of the hip. Randomized trials of abduction treatment of dysplastic hips according to the existing classification systems have failed to show a difference between the treatment and non-treatment groups between six weeks and three months and between three months and six months.15,16 The natural history of the dysplastic hip in the first six months therefore remains one of the most intriguing subjects to study in hip dysplasia.
Material and methods
In order to find data on the natural history of US abnormalities of the hip in children under six months of age, a search in PubMed of the terms “DDH” and “ultrasound” was done to find reports on hips with abnormal US findings that were not treated during a part of or the total course of their development. All untreated hips with abnormal US findings were counted. Groups were made according to the time of first US exam, classification of abnormal US findings, the change in classification during follow-up without treatment and time of follow-up without treatment. Data were corrected for the numbers lost to follow-up. In cases of multiple moments of follow-up, the classification of every moment in follow-up was evaluated separately (individual hip follow-up periods). Totals of every group were counted in numbers and changes in classification were calculated in percentages.
Results
The search in PubMed resulted in 568 hits. Reports on stability were combinations of clinical and US instability and very heterogeneous. Most reports that investigated instability at birth reported no correlation between instability at birth and subsequent development of the hips. Therefore, instability at birth was left out of the analysis trend in this report. From the 568 articles, 23 articles included descriptions of the history of hips with abnormal US outcomes of hips that were not treated. The natural history of a total of 13 561 hips ranging from immature hips to complete dislocation was analyzed. The reports showed a relatively large variety in age of first US, follow-up time periods, protocols, decision trees and classification systems. The classification according to Graf and the FHC according to Morin and Terjesen were used to classify the dysplasia. In this analysis, Graf IIa+ and Graf IIa- hips were merged into the group Graf IIa. In the context of the slight differences in the definition of abnormal between different authors and the different age groups in the FHC classification, the coverage of 50% was defined as the border between normal and abnormal in the articles that reported on the follow-up of FHC. 17 The time period of non-treatment in these reports varied between two weeks and eight years. The times of follow-up of different groups varied depending on the start of treatment of hips that did not develop to Graf I or a FHC of more than 50% at the different times of follow-up.
Reports on hips classified according to Graf
In 18 of the 23 articles that included descriptions of the history of hips with abnormal US outcomes of hips that were not treated, hips were classified according to Graf (Table 118–35). One of the first reports was by Gardiner and Dunn. 18 A group of 59 hips was not treated initially (21 Graf IIa, 12 Graf IIc, 20 Graf III and six Graf IV). After two weeks, 37 hips (71%) ranging from Graf IIa to IV remained untreated (19 Graf IIa = 90%, eight Graf IIc = 66%, seven Graf III = 35% and three Graf IV = 50%). All of these hips were normal at age one year.
Natural history of hips Graf IIa-IV
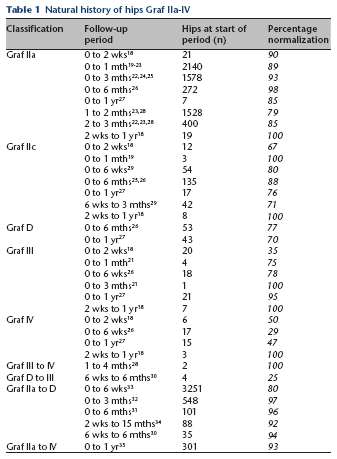
In studies with follow-up periods between 0 and one month, 89% of 2140 Graf IIa hips developed to Graf I hips without treatment.19–23 Between 0 and three months 93% of 1578 Graf IIa hips developed to Graf I hips without treatment.22,24,25 In the study by Bialik et al, 26 98% of Graf IIa hips that were not treated developed to normal by age six months. Rosenberg and Bialik 27 reported normalization of six out of seven Graf IIa hips after follow-up of one year.
In several studies the first US investigation was not within the first week of birth but at a later age dependent on the structure of the screening programme in that particular study. Of 1528 Graf IIa hips at age one month, 79% developed to Graf I at age two months.23,28 Of 400 hips that had Graf IIa hips at two months, 85% developed into Graf I by age three months.22,23,28
Reports on Graf IIc hips also showed a wide variety in natural history prior to treatment. Three hips Graf IIc had become Graf I by age four weeks. 19 In all, 80% of 54 Graf IIc hips followed up from birth to age six weeks developed into normal hips as well as 88% of 135 Graf IIc hips at age six months.25,26,29 One study reported follow-up of Graf IIc hips to the age of one year: 76% of 17 hips became normal without treatment. 27 Of 42 Graf IIc hips diagnosed at six weeks, 71% became Graf I by age three months. 29
Two studies were found with separate reports on Graf D hips. One study reported 77% spontaneous normalization of Graf D hips at age six months 26 , and another study showed 70% normalization of 43 hips at age one year. 27
Sampath et al 30 defined major dysplasia as an alpha angle below 43° or subluxation. The number of hips with developmental dysplasia of the hip (DDH) in the children was not described. Of four children diagnosed with major dysplasia at age three months, one developed normal hips at the age of one year without treatment. Of the children with minor dysplasia detected at the age of six weeks, 94% had no DDH at age six months.
Reports on the natural history of hips with Graf III and Graf IV were rare. Chen et al 21 had four Graf III hips untreated of which three (75%) developed to Graf I in one month. The fourth hip was left untreated and was normal at follow-up at three months. Bialik et al 26 followed 18 Graf III hips and 17 Graf IV hips until the age of six weeks. Around 78% of the Graf III hips developed spontaneously to normal versus only 29% of the Graf IV hips. Rosenberg and Bialik 27 reported a natural history of hips until the age of one year: 95% of the hips with Graf III became normal versus 47% of the hips with Graf IV. Roovers et al 28 had two hips with dislocation at age one month that were not treated and were normal at age four months.
In many studies the classifications were clustered in the outcomes in groups Graf IIa to D, Graf IIa to IV. For the groups Graf IIa to D (4023 individual hip follow-up periods), the outcomes of normalization without treatment were, respectively, 80%, 97% and 96% at ages six weeks, three months and six months.31–33 Two smaller reports with follow-up times between two weeks and 15 months and six weeks and six months had similar results of 92% and 94%,30,34 In one report Graf IIa to IV was not reported separately in 301 abnormal hips in week one and 93% of the hips had normalized at age one month. All these hips were still normal at follow-up at age one year. 35
In eight studies data were found of Graf IIa hips that deteriorated in time (Table 2).
Graf IIa hips with deterioration in time
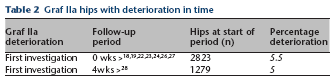
The amount of Graf IIa hips that received treatment at some time during follow-up was 155 out of 2823 (5.5%).18,19,22,23,24,26,27. In the study by Roovers et al 28 the first US measurement for Graf IIa hips was at age one month: 64 (5%) out of 1279 Graf IIa hips developed to abnormal by the age of three months.
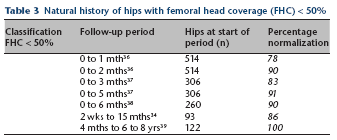
Reports on hips classified with FHC
In five of the 23 articles that included descriptions of the history of hips with abnormal US outcomes of hips that were not treated, hips were classified with the FHC (Table 334,36–39). For reports on FHC less than 50%, 2115 individual hip follow-up periods were counted. Marks et al 36 described a group of 514 hips with a FHC less than 50% at zero weeks. At the next follow-up, a few weeks later with a mean around the age of one month and two months, respectively, 78% and 90% of the hips were spontaneously normalized. Terjesen et al 37 followed 306 abnormal hips and reported spontaneous normalization of 83% and 91% at, respectively, three and five months. The same results were found by Holen et al 38 who reported spontaneous normalization at follow-up at six months in 90% of 260 hips. In the study of Lorente Molto et al, 34 86% of hips that had a FHC less than 50% had spontaneously normalized at age 15 months. Tegnander et al 39 had 170 children with normal clinical examination and FHC's less than 50% at birth. At five months ten children were treated (94%/160 not treated). From this group (90% of 170 patients), 87 children with 122 abnormal hips that were not treated could be retrieved at a follow-up of six to eight years. All untreated hips were normal.
Natural history of hips with femoral head coverage (FHC) < 50%
Discussion
To describe the natural history of abnormal US findings of hips in infants under six months, the literature was searched for hips that were not treated for a shorter or longer time since the first US examination. The vast amount of 13 561 hips was found through PubMed. Although there will be some reports that have been missed or that are out the regular field of language, the studies that were found can be considered to be representative in outlining general trends. Most studies had the first US examination within the first few days after birth; however, in some studies, the first US examination was a few weeks later or at different times within the same study population. For the follow-up, the outcome of every single follow-up period was quantified. Many studies had more follow-up times resulting in more follow-up periods than hips (16 991 versus 13 561). The majority of follow-up periods before starting treatment of hips with US abnormalities did not go beyond the age of three months. However, especially in reports from the 1990s, some authors did not treat for a longer time, even for periods to up to the age of one year or older. There seems to be a tendency in the last decade to treat earlier, despite the good outcomes of the wait-and-see policy in hips with US abnormalities. This trend should have a negative effect on the rise in the amount of data on the outcome of wait-and-see policies, especially with regard to the more serious US abnormalities found in the first weeks after birth.
Most quantifiable classifications were according to Graf (14 876), and a lesser proportion of the studies classified according to the FHC (2115). Furthermore, there was a rather large variation in follow-up moments. In several reports the data switched from the number of hips found with US abnormalities to the number of patients treated in the follow-up or to percentages without reporting the actual numbers. This made reconstruction of the raw data difficult. Therefore, only data that could be traced back to the number of hips or that could be calculated from percentages from the original number of hips were used. Various percentages of hips dropped out of the follow-up at the different follow-up moments in time. Only the hips per follow-up period that remained in the follow-up were calculated. In the studies that clustered the different types of US abnormalities, the outcome of the clustered groups was calculated separately. Given all the recalculations, one can discuss the accuracy of the absolute numbers. However, the discussion on this accuracy should not affect the general trends that can be deduced from the outcomes of these calculations.
The majority of the quantified follow-up periods of hips were Graf IIa hips. As expected, a high percentage of Graf IIa hips showed a natural course to development of a normal hip in the 5965 follow-up periods calculated, with mean percentages of 89% to 98% at different follow-up times between two weeks and six months. These data suggest that Graf IIa can safely be followed for a longer time without treatment in order to detect the relatively few hips that will show a deterioration in time. Deterioration of Graf IIa hips appeared rarely in the data but treatment at some moment in time was still around 5%.
Although there were only between 200 and 300 Graf IIc reported hips, a vast majority also showed a benign course when untreated with percentages between 80% and 100% at the different follow-up periods up to six months. The very small number of hips that were followed until the age of one year all developed into normal hips. These data, combined with favourable outcomes of the clustered data of Graf IIa to IIc between follow-up times of six weeks to six months of between 80% and 97%, also brings up the question of whether Graf IIc hips should be treated early or just followed for a few months. The data also raise questions with regard to power calculations on the effect of treatment when the treatment should be investigated in randomized trials, and which effect of treatment of stable well-centered hips at which age in the first six months of life is clinically relevant. One of the problems is that clinical information such as limited abduction of the hip or instability is often absent in the data reported and in those reports that report instability, the correlation between initial instability, US classification and outcome after longer follow-up cannot be made.
The number of follow-up data of the natural history of Graf III and Graf IV hips was relatively small (n = 87) because these hips were immediately treated in most studies. The outcomes, especially of Graf III hips at birth that were not treated was still surprisingly good, which still leaves room for discussion as to when to start treatment. The clinical information in the reports was insufficient to understand which of these dislocated hips at birth were not treated and on which grounds. The outcome of the clinical investigation still seems the most important factor in the process of decision-making for treatment. 40 This suggests a bias in the outcomes of the dislocated hips that were not treated. It is even more difficult to assess treatment based on US given the reported poor consistency in diagnostic criteria using US in DDH and the fact that there is no consensus on which degree of acetabular dysplasia, as defined by US, to treat or not.41,42
Conclusion
The natural history of DDH seems to show a benign course, especially in stable, well-centered hips. The fact that even the unstable and dislocated hips do relatively well without treatment in a substantial percentage probably contributes to the fact that all studies on US screening of hips for detection of relevant DDH in order to improve outcomes of treatment are rated as substantially underpowered. 43
Footnotes
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
None declared.