
Abstract
Purpose
The treatment of bilaterally dislocated hips with a Pavlik harness can have deleterious effects if one hip remains dislocated. We assess the success of potentially leaving the persistently dislocated hip free and the relocated hip in a “hemi-Pavlik” harness.
Methods
In this report, we retrospectively review three cases of bilaterally dislocated hips in children who were treated with a Pavlik harness. Only one hip was effectively reduced by the harness and, in each case, half of the harness was cut away to create a “hemi-Pavlik” harness and the free side was operated on at a later date.
Results
Initial follow-up has shown that the “hemi-Pavlik” harness is effective in maintaining reduction of one hip whilst leaving the other hip untreated, thus, avoiding the complications of prolonged use of the harness in an unreduced hip or having both hips dealt with operatively.
Conclusions
We suggest, in the early stages, that if only one side of the bilaterally displaced hips can be reduced, the non-reduced side should be left free and an elective procedure carried out at a later stage. In the early stages, a “hemi-Pavlik” harness is effective in treating the reducible hip and causes no treatment obstacles for the irreducible side.
Introduction
Developmental dysplasia of the hip (DDH) denotes a wide spectrum of pathological conditions, ranging from subtle acetabular dysplasia to irreducible hip dislocation [1]. When DDH is recognised in the first 6 months of life, treatment with a Pavlik harness frequently has good results, although the success rate may be lower in children over 12 weeks of age [2–5].
Inappropriate continued use of a Pavlik harness when the hip remains unreduced can be detrimental [2]. Rates of avascular necrosis (AVN) after neglecting a dislocating hip vary from 2 to 92% [6, 7] (Pavlik himself reported a 16% risk).
Previously, a satisfactory reduction was assessed using plain radiographs and clinical evaluation. The accuracy in the assessment of reduction has been improved with the use of ultrasound [6, 8–10]. If the hip fails to reduce after a reasonable time period (usually a maximum of 3 weeks), it is generally accepted that the Pavlik harness should be removed and an alternative treatment method sought [6].
In this series, we report three cases of children born with bilateral hip dysplasia. In each case, it was only possible to obtain a satisfactory concentric reduction with a Pavlik harness in one hip and, so, the harness was modified to allow treatment to continue for the reduced hip without damage to the unreduced and “free” hip.
Methods
Three children with a diagnosis of bilateral hip dislocation are reported in this series. Patients were referred to the orthopaedic department following clinical diagnosis by the neonatologists. The patients were then examined, the diagnosis confirmed clinically and sonographically, and a Pavlik harness applied. Thereafter, the hips were assessed by clinical examination and by ultrasound scanning at weekly intervals by the Graf method.
In each case, the maintenance of a concentric reduction of one hip was possible but the other failed. In our institution, it is routine practice to abandon treatment with the Pavlik harness if the hip is not relocated within 3 weeks. After 3 weeks, in each case, the position of one hip was deemed satisfactory whilst the other hip remained dislocated. At this stage, therefore, the Pavlik harness was modified by removing the straps on the side of the irreducible hip (Figs. 1, 2, 3). The harness was left on the infants for 12, 14 and 16 weeks, by which time the relevant hip was stable and sonographically normal. During this time they were regularly monitored using ultrasound to ensure the restrained hip remained located within the joint.

Child 1 front and back photos showing the hemi-Pavlik construct

Child 2 in the hemi-Pavlik harness, –front view
The free dislocated hip was then treated at a later date by conventional methods (Table 1). Two hips were treated by closed reduction under anaesthesia at the age of 5 and 6 months, respectively, and the third child underwent an open reduction at the age of 1 year having failed an attempted closed reduction under anaesthesia. It is our practice to wait until 1 year of age before undertaking open reduction via the modified anterior approach for technical and aesthetic reasons. With regard to closed reduction, the anaesthetic facilities do not permit earlier attempted manipulative reduction under anaesthesia.
Summary of the cases and times of treatment
Results
There were three cases referred to the paediatric orthopaedic consultant (Table 1).
Two patients were born by normal delivery and the third by Caesarean section. None had any other abnormalities.
In all three cases, the diagnosis was suspected following clinical diagnosis by a paediatrician using standard tests (Ortolani's and Barlow's tests) and confirmed on ultrasound (Figs. 4, 5).
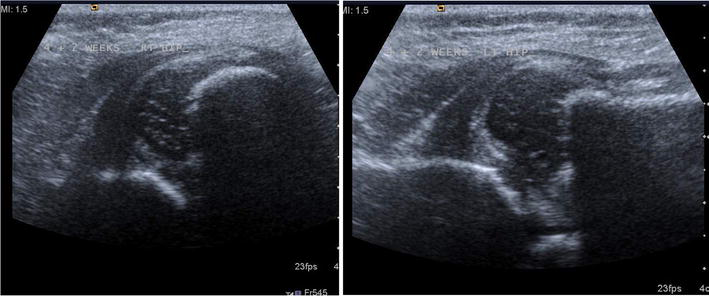
Patient 2: initial scans
The average waiting time for review by our centre was 12 days after the referral.
A Pavlik harness was applied and an ultrasound was performed to confirm the position and reduction [8].
The “untreated” hips were dealt with subsequently. Two cases underwent a successful closed reduction under general anaesthesia (children 1 and 3) and one case required open reduction at one year after an unsuccessful attempt at reducing the hip by closed means under anaesthesia when the child was aged 6 months (Figs. 6, 7 show the latest radiographs following treatment in patients 2 and 3, respectively).

Patient 2: radiograph at age 2 years 1 month, right hip treated by open reduction aged 1 year (note persistent dysplasia of the right hip)

Patient 3: radiograph at age 3 years 10 months, treated by closed reduction aged 5 months
Table 1 shows a summary of the cases.
Discussion
The use of the Pavlik harness is well established in the treatment of DDH. There are, however, recognised complications, particularly when the use of the harness is inappropriate [6]. In circumstances where a dislocated hip fails to reduce, it is recommended that the use of the harness be abandoned. However, where bilateral dislocations are present and one hip fails to reduce whilst the other hip reduces well, the clinician faces a dilemma. In some centres, it may be possible to attempt a manipulative reduction under anaesthesia, but in very young infants, adequate facilities for anaesthesia may not be available. In this situation, rather than abandon treatment altogether until the child is older, the creation of a “hemi-Pavlik” harness offers a suitable alternative. Loosening the amount of flexion and abduction on the irreducible hip may be another way, but this may be more difficult to control and some restriction may remain. The other question that is raised by this study is whether or not unilateral abduction devices are preferable for unilateral cases of hip dysplasia in order to remove the risk of AVN altogether in the normal hip, but this requires further investigation.
The three cases in this report show that, in bilateral hip dislocation, where one hip remains dislocated, the creation of a “hemi-Pavlik” harness enables continued successful treatment of the reduced hip and, at the same time, the potential complications of leaving the unreduced hip in the harness are avoided. Further treatment using conventional methods in the contralateral hip, however, is not prevented by leaving this hip free.