
Abstract
Abstract
Purpose
Prospective randomized controlled trials and long-term studies are essential future directions for building evidence-based practices in developmental dysplasia of the hip (DDH), however, sufficient attrition in data (> 20%) can introduce bias deteriorating research quality. Pelvic radiography is synonymous with DDH assessment and so are Gonadal Shield (GS) recommendations with pelvic radiography. Nonetheless, losses to diagnostic information and inadequate protection have been increasingly implicated to GS usage, with significantly worse implications in female patients. Understandably for DDH, a disease with 80% female prevalence, the impact of GS usage on quality of radiographs and readability of radiological data may be drastic. This study aims to objectively define the implications of GS recommendations in DDH patients.
Methods
Pelvis radiographs of all DDH patients under the hip surveillance programme at a tertiary care hospital with a written protocol for GS usage were evaluated. Images were reviewed for gender, GS presence, adequate gonadal protection and obstruction of essential anatomical landmarks for pelvic indices.
Results
In all, 131 pelvis radiographs with DDH diagnoses (age: 1.25 to 6 years; 107 female, 24 male pelvises) were reviewed. Only 42.67% (56) of pelvis radiographs used GS despite the presence of a clear protocol. Useful anatomical landmarks were obstructed in 58.9% of radiographs with GS present. Lost diagnostic information was more common in female patients than male patients (68.1% versus 11.1%, p < 0.01). GS was ineffective at gonadal protection in 73.2% (41) of the pelvises with worse protection in female patients (78.7% vs 44.4%; p = 0.03).
Conclusions
Ironically, essential anatomy was obstructed in all the adequately protected female pelvises. Routine GS usage results in substantial attrition of radiographic data in DDH patients.
Level of Evidence
III
Keywords
Introduction
High quality prospective randomized controlled trials (RCT) and long-term follow-up studies are frequently suggested future directions for building evidence-based practices in developmental dysplasia of the hip (DDH).1,2 Attrition of data, however, is a well perceived critical limiting factor for the building of high-quality evidence. And while ‘how much attrition is acceptable?’ is a relative term a loss of ≥ 20% often indicates bias.3,4 Evidence-based medicine also uses a cut-off of an 80% follow-up in when judging levels of evidence as ‘high’ or ‘low’-quality RCTs.3,5 Researchers naturally aim at identifying and then minimizing all possible sources of attrition in their studies to improve evidence quality.
DDH research in children older than six months are customarily based on certain radiographic pelvic indices (Fig. 1). Adequate visualization of essential anatomical landmarks on pelvic radiographs standardized for tilt and rotation are proven prerequisites for collecting accurate radiographic data in DDH. 6
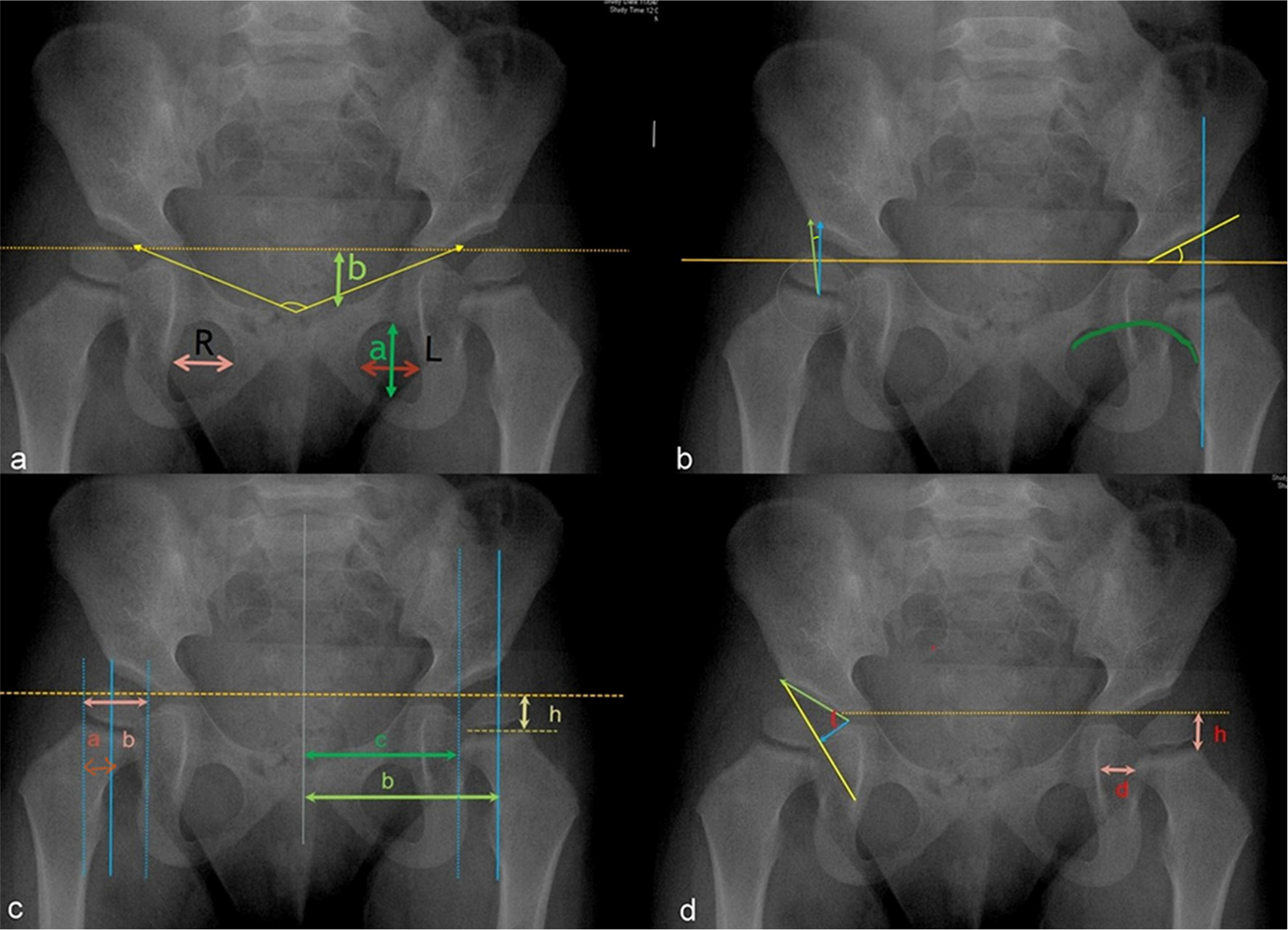
Routine radiographic pelvic indices used in assessment of a young DDH patients and the corresponding anatomical landmarks required for their measurement: (
Gonadal shields (GSs) were introduced to pelvic radiography in the 1950s with the intention of protecting young gonads from radiation. Guidelines to use GS presently exist in most hospitals. However, the effectivity of GS application in pelvis radiographs has been increasingly questioned by multiple audits.7–18 Studies have identified misplaced shields in 26% to 81% and obstructed anatomical landmarks in 13% to 82% of pelvis radiographs that applied GS. 7 GS use during pelvic radiography in female patients is especially associated with significantly lower effective protection to gonads and higher frequency of blockage to pelvic anatomy;7,8,14–17 lack of easily identifiable external landmarks for ovaries and wide variability in its location within the pelvis of a growing child contribute to the significantly higher undesirable effects of GS in female patients.14,15,19,20 It is logical to assume that DDH which has an 80% female prevalence should have a magnified negative impact of GS usage on retrieval of radiographic data and protection to gonads. 1 However, implications of GS use in DDH patients is largely unrecognized.
This study aimed to objectively define implications of GS recommendations during pelvic radiography in a consecutive series of young DDH patients. We studied the prevalence of GS application during pelvic radiography of DDH patients, and whenever it was applied, the adequacy of gonadal protection, the inadvertent obstruction of anatomical landmarks and attrition of related imaging data due to GS application were studied. We also evaluated for any differences in the effects of GS application in between male and female DDH patients.
Materials and methods
This study was conducted in our tertiary paediatric orthopaedic referral centre (Prince of Wales Hospital). We retrieved the hospital records for all the children diagnosed with DDH between the years of 2010 and 2011. The study group of DDH patients constituted of early detected DDH patients treated successfully during infancy by Pavlik harness and abduction nursing with clinical-sonographic resolution of hips. Thereafter these DDH patients were routinely followed up with pelvic radiographs starting at six months from birth and then yearly for monitoring of dysplasia, and to ensure an offer of treatment could be given if severe acetabular dysplasia persisted. The plan for discharge was made when patients showed complete resolution of the dysplasia on radiographs. The pelvic radiographs taken during their hip surveillance between 2010 and 2016 were retrospectively retrieved from the Picture Archiving and Communication System (PACS) to form the study group.
During these study years, the hospital guidelines recommended routine use of GS during pelvis radiography in children with an aim to limit radiation dose to as low as reasonably achievable (the ALARA principle). First baseline pelvis radiographs and images from operating theatre or C-arm were excluded from the study as GSs were not used in these settings.
The pelvic radiographs were reviewed for the patient's gender and the presence or absence of GS. If GS was present, radiographs were additionally evaluated for: obstruction to anatomical landmarks by GS and protection to gonads by GS. The pelvic indices used for DDH patients are fundamentally based on specific anatomical landmarks (Fig. 1). 6 The obstruction to these essential landmarks 6 was objectively assessed in each radiograph and loss of related radiographic data was assessed.
For boys, protection was regarded as inadequate if part, or all, of one or both testicles, was visible beyond the limits of the shield. For girls, exposure of more than a centimetre-wide rim of pelvic contents within the pelvic basin after shielding was regarded as inadequate protection. 19
Statistical analysis
Numeric variables on the use of GS in radiographs were represented in counts and percentages (n, %). Fisher's Exact test was carried out to evaluate possible differences in the implications of GS application during pelvic radiography in between male and female DDH patients. A two-sided p-value ≤ 0.05 was considered statistically significant. All statistical analyses were performed using IBM SPSS version 24.0 (IBM Corp., Armonk, New York) was used for all statistical analysis.
Results
In all, 68 patients were diagnosed with DDH in the years 2010 and 2011 and later underwent hip surveillance. A total of 131 pelvis radiographs (107 female and 24 male pelvises) which were taken during the hip surveillance formed the study group after exclusions (Fig. 1). In all, 38 patients had complete resolution of dysplasia by walking age, and therefore had only one post-infancy pelvis radiograph. Other children with persistent acetabular dysplasia were kept under radiographic surveillance until complete resolution of dysplasia. Therefore, 11 patients had two serial radiographs, five had three serial radiographs, six had four serial radiographs, one had five serial radiographs and one had six serial radiographs post-infancy before completion of the study. Four patients in this study group showed persistent severe dysplasia and were treated with night time hip abduction brace with improvement in acetabular dysplasia.
GS use in DDH patients
Overall, 42.7% of pelvic radiographs had GS applied during radiography, 11.4% (15) had adequate protection to gonads and 25.2% (33) of the radiographs suffered from obstruction to one or more essential anatomical landmarks by GS (Table 1, Fig. 2). This, in turn, affected radiographic data retrieval in 37% of the patients undergoing hip surveillance (many children had multiple radiographs during the entire duration of hip surveillance). In radiographs with GS identified, 26.8% (15) demonstrated adequate protection to gonads (Fig. 3a) and 58.9% (33) had essential anatomy obstructed. The frequency of specific anatomical landmark blocked, and corresponding affected pelvic indices has been charted in Table 2.
Gonadal shield (GS) use in young children with developmental dysplasia of hip. Data presented as n (%)


Examples of obstruction to essential anatomical landmarks due to gonadal shield application in pelvic radiographs of developmental dysplasia of the hip patients.
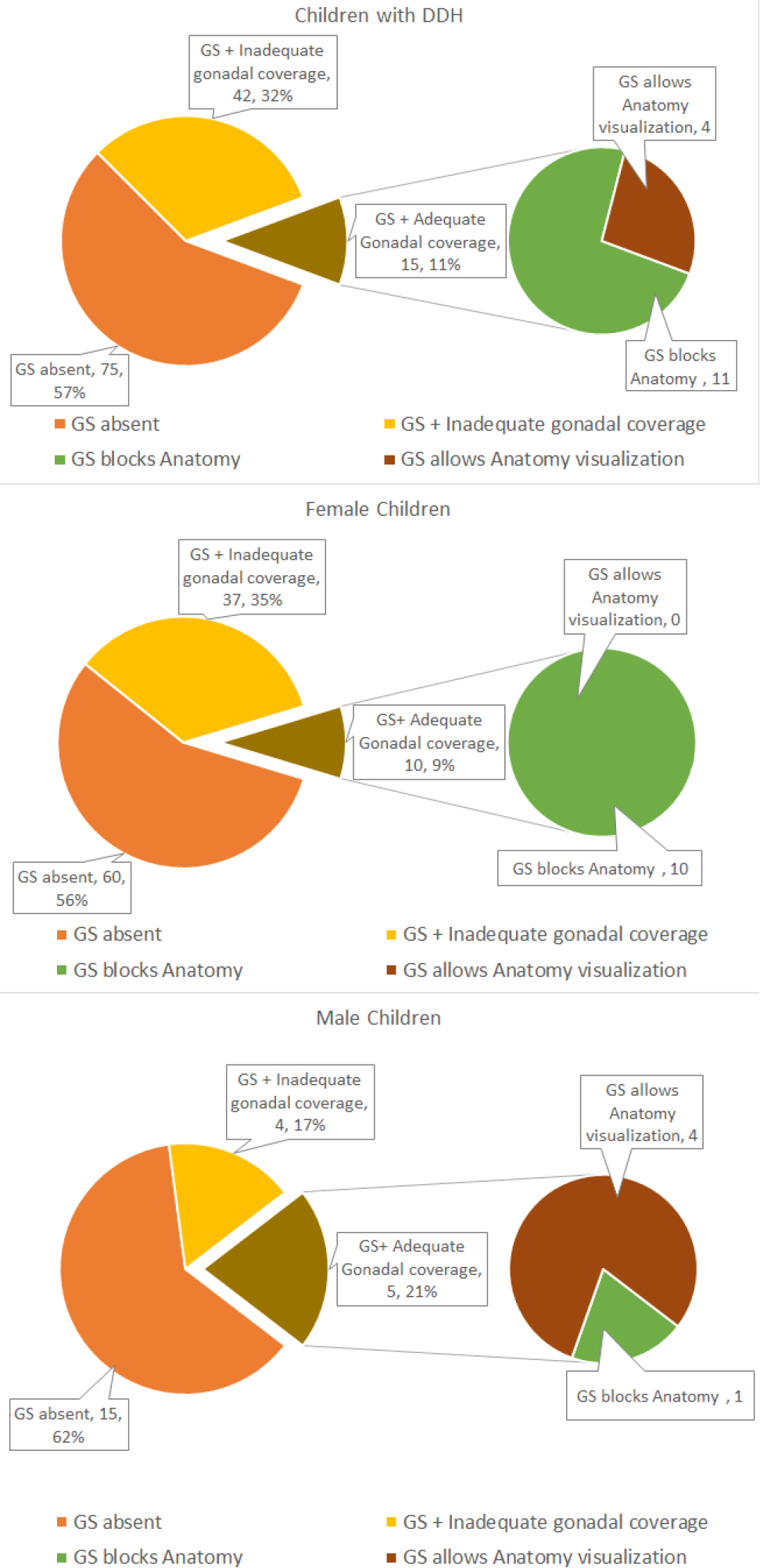
Pie charts explaining the effect of gonadal shield (GS) recommendations during pelvic radiography on visualization of essential anatomical landmarks required for pelvic indices measurement in developmental dysplasia of the hip (DDH) and the protection of the gonads in these radiographed pelvises: (
Obliteration of individual anatomical landmarks by gonadal shield (GS) and its effect on attrition of pelvic indices
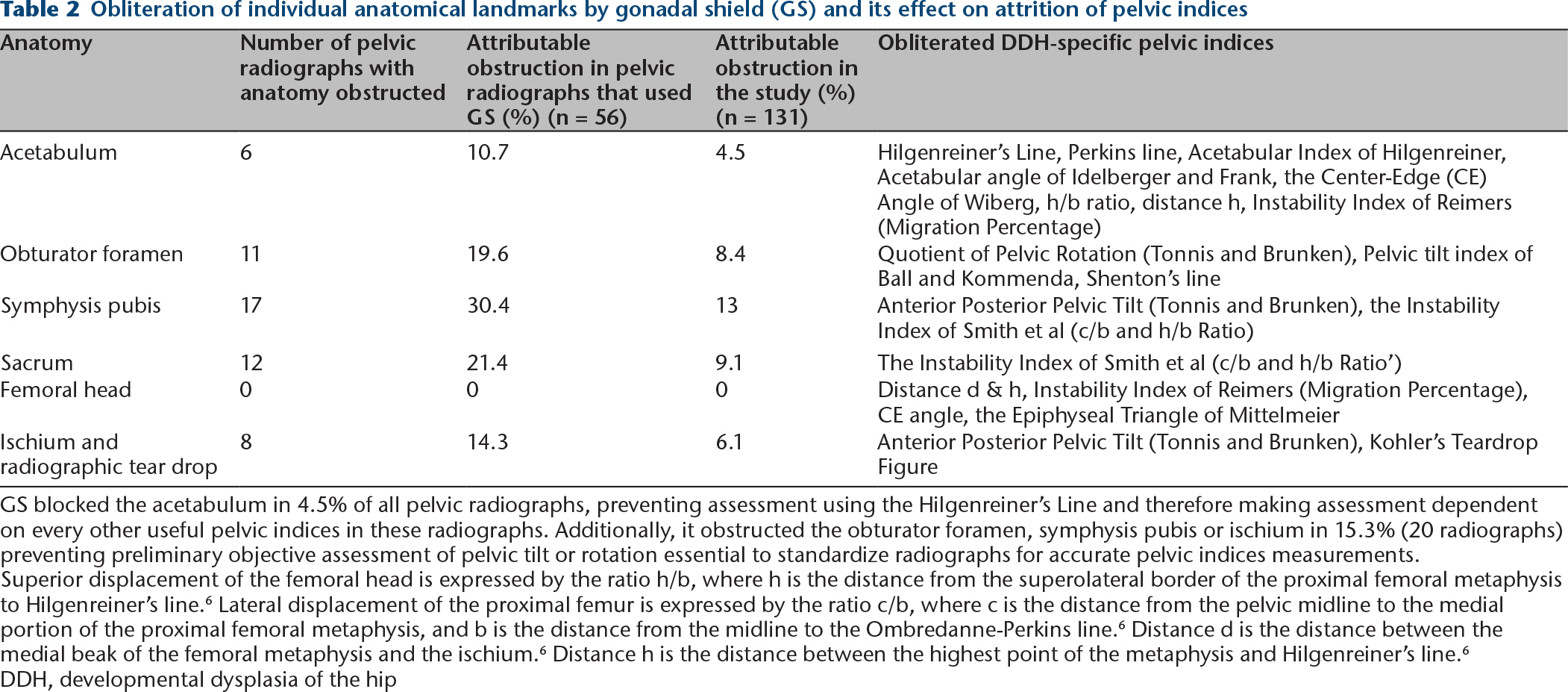
GS blocked the acetabulum in 4.5% of all pelvic radiographs, preventing assessment using the Hilgenreiner's Line and therefore making assessment dependent on every other useful pelvic indices in these radiographs. Additionally, it obstructed the obturator foramen, symphysis pubis or ischium in 15.3% (20 radiographs) preventing preliminary objective assessment of pelvic tilt or rotation essential to standardize radiographs for accurate pelvic indices measurements.
Superior displacement of the femoral head is expressed by the ratio h/b, where h is the distance from the superolateral border of the proximal femoral metaphysis to Hilgenreiner's line. 6 Lateral displacement of the proximal femur is expressed by the ratio c/b, where c is the distance from the pelvic midline to the medial portion of the proximal femoral metaphysis, and b is the distance from the midline to the Ombredanne-Perkins line. 6 Distance d is the distance between the medial beak of the femoral metaphysis and the ischium. 6 Distance h is the distance between the highest point of the metaphysis and Hilgenreiner's line. 6
DDH, developmental dysplasia of the hip
Gender-specific implications of GS use in DDH patients
GS application during pelvis radiography among girls offered significantly less protection to gonads when compared with radiography in boys (21.3% versus 55.6%, p = 0.03), and was accompanied by a significantly higher obstruction to anatomical landmarks (68.1% versus 11.1%, p < 0.01) (Table 3). In all, 97% (32) of radiographs with obliterated anatomy and 90.2% (37) of radiographs with inadequately protected gonads with GS occurred in female DDH patients (Table 1). In the radiographs with adequately protected gonads, the visibility of an essential landmark was significantly better in male patients (p < 0.01) (Figs 3b and 3c). Among the radiographs with inadequate shielding to ovaries, GS additionally obscured anatomy in 59.5% of these radiographs. Contrastingly, radiographs of male DDH patients never shared obstruction to essential anatomy when inadequately shielded by GS.
Variations in gonadal shield (GS) use during pelvic radiography of male and female children with developmental dysplasia of the hip
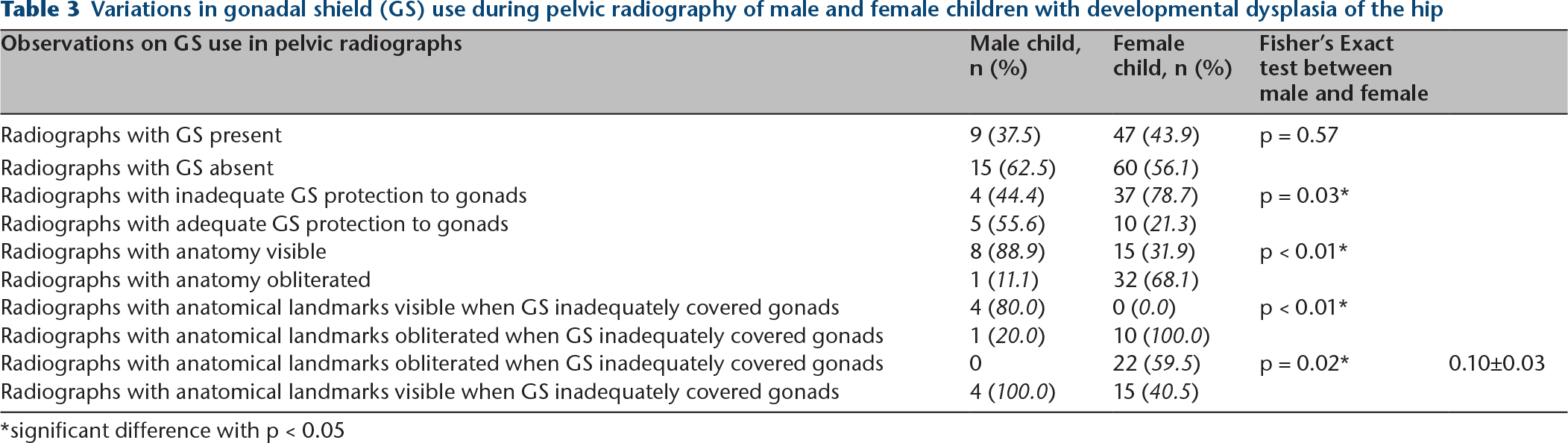
significant difference with p < 0.05
Discussion
We found GS prevalence during pelvic radiography of young DDH patients to be at 43%, a similar lower GS prevalence of 58% (95% confidence interval: 40% to 74%) has been suggested by Karami et al 9 in their recent meta-analysis on GS. The placement of GS in practice seems to be much harder than one would ideally wish for. Radiographers are likely to restrict GS application when there are difficulties in its optimal positioning – a situation relatable to radiography in anxious younger children – to prevent repeat radiations stemming from a misplaced GS that may obscure anatomy. This view does find an indirect support from our study, as inadequately placed GS additionally obscured anatomy in 53.7% of all radiographs and in 100% of all female radiographs (Table 1).
However, despite an overall lower prevalence of GS usage in our cohort, such usage adversely affected data retrieval in a quarter of radiographs by obscuring anatomy while providing adequate gonadal protection in only one tenth of the radiographs. Consequently, several routine pelvic indices needed for DDH assessment could not be obtained accurately from these radiographs (Table 2). In a longitudinal DDH study, a loss of patient information including radiographic data from a time point would cumulatively diminish the final sample size available for evaluating results. By the end of this five-year surveillance, GS accounted for a loss of one or more radiographic references in 37% of the DDH patients. A similar scale of obstruction to radiographic information may under power longitudinal cohort studies on DDH and prevent accurate assessment of their hypothesis. 3 Even a smaller attrition of 20% in the cohort,3,5 can potentially introduce non-randomized bias in long-term RCTs including those on DDH and lessen their level of evidence to low-quality RCTs. 5 Additionally, considerable attrition in data will also make the generalization of the results from such studies unreliable. 3
Our study finds its relevance as recommendations for GS application during pelvic radiography is almost universal for children (including those with DDH) backed by the belief that shields adequately protect gonads from radiation. And while reports on potential drawbacks in terms of inadequate protection offered by GS have been repeatedly published, GS as an additional source of attrition to diagnostic data in DDH is being objectively studied for the first time. We found that when shields were used, they obstructed pelvic landmarks in 58.9% of the radiographs. Our results on GS induced obstruction to pelvic anatomy compares favourably with earlier reports of obstruction to pelvic anatomy cited between 13% to 82%.7,12,14,15,17,18 These studies, however, were limited by a lack of definition for the pelvic anatomical landmarks considered obstructed or when defined, these landmarks could not represent the wide spectrum of radiographic pelvic indices used in young DDH patients.7,15
Being aware that studies on DDH may selectively use only specific pelvic indices of interest to draw results, we further dissected the results on landmarks blocked by GS to individual anatomy obstructed (Table 2). This should allow researchers to estimate the degree of attrition expected for a specific pelvic index of interest. Interestingly, each anatomical landmark suffered substantial obstruction from GS use, ranging between 11% to 30%. When applied, GS obstructed the acetabulum in 11% of the radiographs. For the whole cohort, it meant that 4.5% of the pelvic radiographs were unusable for extracting any DDH specific pelvic indices. This importantly made clinical decision-making impossible for these patients and required repetition of radiographs in the next early follow-up. Our findings are in line with Liakos et al's observation 15 of a 13% loss in data for acetabular index or Shenton's line due to GS use during pelvic radiography in four- to six-year-old girls. In 2017, Lee et al 17 found GS obscured the femoral head and acetabulum in 2% of the radiographs. The older age of their cohort (eight to 12 years) may be a contributory factor to their slightly deflated results. Understandably older children may be more amenable to a radiographer's instructions and may have better shield placement compared with the younger one- to five-year-old children in our study. In all, 15.3% of all radiographs in our study could not be objectively standardized for tilt or rotation due to the obstruction to symphysis pubis, ischium or obturator foramina which inhibited determination of accuracy of acetabular index and the clinical decisions made upon these values. 6 (Table 2).
Gender-specific evaluation of GS use in radiographs confirmed that most drawbacks associated with GS application were concentrated to its use in female DDH patients. The prevalence of GS was similar in both genders but radiographs of female DDH patients had anatomy obstructed in a significantly higher number of radiographs compared with those of male patients (68.8 versus 11.1%, p < 0.01). Other studies evaluating the gender-specific use of GS too state a higher obstruction to anatomy by GS in girls compared with boys.7,14,18 Additionally, adequate protection to gonads by GS during pelvic radiography in female DDH patients was rare compared with male DDH patients (20.8% versus 62.5, p = 0.03). Our observations are in line with Karami et al's 9 recent metanalysis of 18 studies on GS use in pelvis radiographs who found a significantly worse protection to gonads in female compared with male patients (15% versus 48%; p < 0.01). Worryingly, when GS did adequately protect ovaries in our study, it unequivocally ended up obliterating essential anatomical landmarks in those radiographs. Stark contrasts were radiographs of male DDH patients, where adequately positioned GS seldom obstructed essential anatomy (100% versus 20%, p < 0.01). Reasonably, malpositioned shields during radiography that inadequately protects gonads can be expected to additionally cause obstruction to important anatomy in radiographs. However, again only the female DDH patients suffered this ‘double whammy’ from GS use, with 60.5% of their radiographs with inadequate protection to gonads showing a coexistent obstruction to essential anatomical landmarks (Fig. 3). In 2014, Warlow et al 18 too suggested similar findings: 63% of images of female pelvises in their study exhibited a combined error of inadequate protection, obstruction to anatomical landmark and a too small GS but only 24% of radiographs from male patients had all the three errors. Female DDH patients are hence at risk of getting twice the radiation dose if such inadequate radiographs require repetition. We conclude that ambiguity of external landmarks for GS placement, widely variable location of ovaries within the pelvic inlet and the unrealistic precision required for adequate protection to ovaries does adversely impact GS application in female DDH patients. While boys, with external gonads placed out of pelvis inlet are more amenable to optimal GS use.
Presence of a naturally skewed female to male (80:20) gender ratio among DDH patients and significantly worse undesirable effects of GS observed in pelvic radiographs of female patients may suggest that the maleffects of GS in them can easily reflect on the whole cohort of DDH patients. In all, 92.7% of the radiographs with inadequately protected gonads despite GS and 96.9% of the radiographs with landmarks obstructed by GS in this study belonged to female patients even when radiographs from female patients represented only 81.7% of all radiographs; in 2012, Frantzen et al 7 also observed in their mixed-gender cohort of one- to five-year-olds 7 that 100% of the radiographs with obstructed anatomy belonged to female patients.
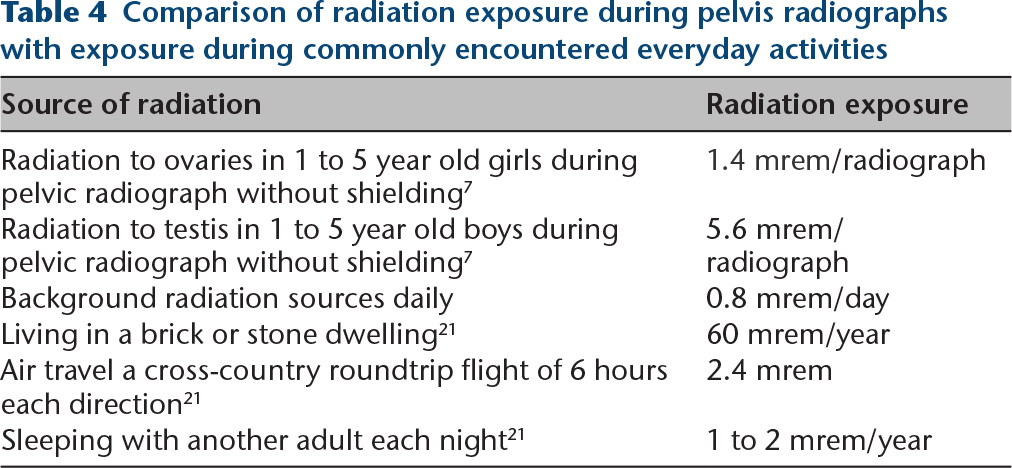
Studies have demonstrated that modern radiography techniques have a much lower radiation and the absolute radiation dose reduction to gonads by GS may not be substantial enough.7,15,21 Radiation dose especially to ovaries is low enough to compare favourably with radiation exposure during casual daily activities7,21 (Table 4). Frantzen et al7 reported on the detrimental adjusted risk for heritable disease in children aged one to five years old without shielding to be within the allowable limits of risk as per the International Commission on Radiological Protection guidelines; 22 this risk was also three times less in girls compared with boys (0.3 x 10-6 for boys and 0.1 x 10-6 for girls). They also found that in considering the need of retakes, shielding did not reduce the risk of radiation exposure in boys but potentially increased the risk of radiation exposure in girls. 7
Comparison of radiation exposure during pelvis radiographs with exposure during commonly encountered everyday activities
Our study did have some limitations. The retrospective nature of the study restricted our review to only those images that were uploaded to the PACS but it did not account for radiographs discarded and redone by radiographers including those due to malpositioned GSs obscuring anatomy. Also, it did not allow us to compare the number of retakes needed for radiographs that used or did not use GS. The unaccounted deleted images if commonplace may increase the total radiation exposure for each radiographic appointment in those children and requires further evaluation in a prospective study. The effect of GS on obscuring landmarks may also get inflated when those deleted images are considered. Also, DDH researchers might not always use all the above-mentioned pelvis indices but rely on fewer selected indices to calculate results, which will accordingly decrease the degree of attrition when lesser anatomical landmarks are deemed essential. However, visualization of acetabulum and landmarks for assessing standardization of pelvis radiographs are the minimum basic requirement in all DDH researchers and important for the accuracy of clinical decisions made upon radiological indices. 6
Conclusion
Overall GS recommendations during pelvic radiography of young DDH patients offers adequate radiation protection in a meagre percentage of radiographs but can cause substantial losses to diagnostic information, especially in the female DDH patients. From a research perspective, GS recommendations can cause substantial attrition to the data on Pelvic indices and may affect the quality of evidence from researches based on young DDH patients. Importantly, the same losses can easily translate to difficulty in clinical decision-making. At centres where modern lower dose radiography facilities are available, parental education on the lowered radiation risks to ovaries during modern radiography 7 and on the small percentage of ovaries that actually receive adequate protection from GS without losing diagnostic information may help formulate a consensual agreement at avoiding GS during pelvic radiography among young female DDH patients. While the cumulative risk from multiple serial radiographs required in some DDH patients is not as clear, a shift in focus from GS to other alternatives for reducing radiation exposure appear as better future directions. Focus on judiciary use of radiographs in DDH patients, stress on the use of modern radiograph techniques with lower ionizing radiation dosage in paediatric pelvis radiographs, use of MRI for evaluation of post-surgical femoral head reduction in spica22,23 (if not for routine screening due to risk of sedation and resource intensive needs) and continued research to further diminish the radiation dosage from radiographs, may help reduce the potential risks from multiple radiographs. However, if GS recommendations are continued by institutions, researchers are cautioned to seek larger sample sizes in anticipation of data attrition on pelvic indices.