
Abstract
Abstract
Background
Selective dorsal rhizotomy (SDR) is a surgical procedure for treating spasticity in ambulant children with cerebral palsy (CP). However, controversies remain regarding indications, techniques and outcomes.
Current evidence summary
Because SDR is an irreversible procedure, careful patient selection, a multi-disciplinary approach in assessment and management and division of the appropriate proportion of dorsal rootlets are felt to be paramount for maximizing safety. Reliable evidence exists that SDR consistently reduces spasticity, in a predictable manner and to a substantial degree. However, functional improvements are small in the short-term with long-term benefits difficult to assess.
Future outlook
There is a need for high-quality studies utilizing long-term functional outcomes and well-matched control groups. Collaborative, multicentre efforts are required to further define the role of SDR as part of the management paradigm in maximizing physical function in spastic CP.
Introduction
Primary neurological factors (e.g. spasticity, weakness, balance, poor selective motor control) and secondary deformities (e.g. joint contractures, bony deformities, joint dysplasia) both compromise gait and motor function in children with cerebral palsy (CP). Correction of secondary deformities can be done via orthopaedic intervention, often in the form of single event multi-level surgery (SEMLS). 1 However, this does not address the primary neurological factors. A growing body of literature suggests that selective dorsal rhizotomy (SDR) is effective in improving one neurological factor – spasticity, which may lead to improvements in function and gait.
Spasticity is defined by increased resistance with increasing velocity of movement and/or the presence of a spastic catch. 2 A number of interventions are available for the management of spasticity. Broadly, these can be described as surgical versus non-surgical, temporary versus permanent and focal versus generalized (Fig. 1). 3 SDR is a form of surgical, permanent and relatively generalized treatment option for lower extremity spasticity that reduces tone by selective sectioning of lumbosacral afferent nerve rootlets.
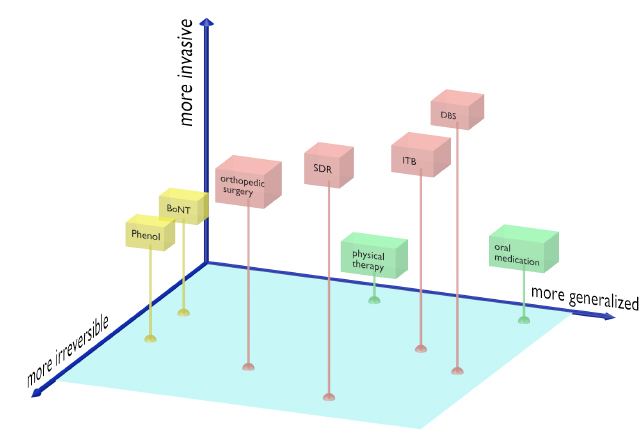
Tone management options in cerebral palsy. Tone management is only one aspect of the musculoskeletal care needs of children with spastic cerebral palsy: lever arm dysfunction and joint deformity are other important aspects and are not represented in this diagram. Within the tone management paradigm, options include non-invasive (green), injections (yellow) and surgical (red). Selective dorsal rhizotomy (SDR) is a form of surgical, irreversible and largely generalized option for tone reduction. Orthopaedic procedures for tone reduction include muscle/tendon lengthening and transfers (BoNT, botulinum toxin; ITB, intrathecal baclofen; DBS, deep brain stimulation; SDR, selective dorsal rhizotomy).
However, much controversy remains regarding the use of SDR, how patients should be selected for the procedure and what outcomes can be achieved.4–6 Quality long-term data are lacking, and much of what is done in clinical practice is not supported by strong evidence. In addition, natural history studies exist that show reduction in spasticity 7 and improvement in gross motor function 8 can occur in the absence of intervention, making results of SDR difficult to interpret without well-matched control groups. This article aims to serve two purposes: 1) to explore the boundaries of our knowledge by providing a review of the current literature; and 2) to share three decades of experience from our institution on the use of SDR in helping children with CP.
The focus of this review will be on the role of SDR in maximizing mobility and independence for ambulant children with CP, functioning at Gross Motor Function Classification System (GMFCS) 9 levels I to III. A nonselective dorsal-ventral rhizotomy may be performed in individuals with more severe impairments, functioning at GMFCS levels IV or V, in order to meet palliative care goals such as pain relief and improvement of caregiving. 10 Since this is a different procedure with different indications and expectations, it is outside the scope of this review and will not be addressed here.
History and rationale
In preterm infants, the deep periventricular white matter is metabolically susceptible to injury. Damage to this area typically leads to reduced inhibitory input into the spinal interneuron pool from descending neural pathways. This results in excessive spinal cord alpha motor neuron activity and spasticity. Afferent dorsal root input into the spinal interneuron pool has a further net excitatory effect on the on the alpha motor neurons. Dorsal rhizotomy reduces the amount of excitation of alpha motor neurons and thereby reduces spasticity (Fig. 2). 11
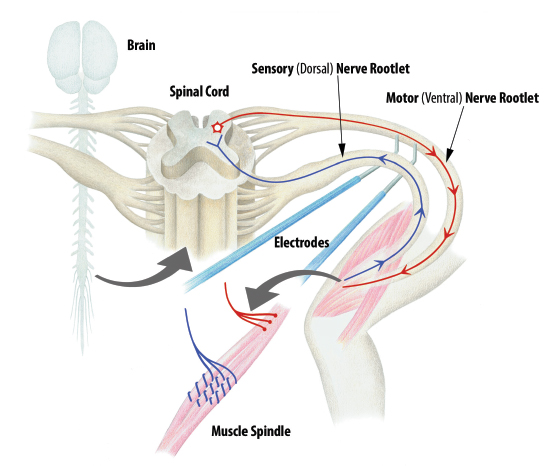
Spasticity reflex arc schematic diagram. Muscle stretch stimulates dorsal (afferent) sensory nerve rootlets, which in turn has a net excitatory effect on alpha motor neurons within the spinal cord. The spasticity arc is completed via the hyperstimulated efferent ventral motor rootlets. During SDR, individual dorsal rootlets are isolated and stimulated with a Peacock probe. Those that produce inappropriate activation are sectioned. Illustration used with permission, courtesy of Timothy T. Trost.
Although the first dorsal rhizotomy was performed more than 100 year ago, 12 the procedure's evolution since then has taken several major turns. Foerster's initial method of non-selective rhizotomy fell into disuse for more than five decades because of the adverse consequences of excessive de-afferention. In the 1960s, the procedure was revised by sectioning only a fraction of the rootlets based on the patient's preoperative function, 13 and then further refined into selective dorsal rhizotomy by electrically stimulating the rootlets intraoperatively and measuring the electromyographic response before sectioning. 14 In South Africa, Peacock shifted the site of rhizotomy from the conus medullaris region to the cauda equina. 15 This makes rootlet identification easier in an effort to avoid bladder dysfunction, one of the complications noted by Fasano et al. 14 In recent years, some surgeons have adopted a more limited laminectomy at the level of the conus as advocated by Park and Johnston. 16 Although technically more challenging for identification of rootlet levels, proponents of the conus approach argue that it results in a smaller scar, reduced iatrogenic spinal instability, decreased postoperative pain and quicker recovery. 17
Following his relocation to the United States from South Africa, Peacock helped popularize SDR in North America for the treatment of children with spastic CP.18,19 Understanding that children with spastic CP are heterogenous, Peacock helped establish a set of selection criteria for SDR to maximize safety and efficacy. These criteria were adopted by the multidisciplinary team of orthopaedic surgeons, physiatrists and neurosurgeons at our institution in the 1980s. In the three decades since, our protocol for the care of children in the SDR pathway has stayed relatively constant. The original criteria were incorporated with pre- and postoperative 3D gait analysis (3DGA), a multi-disciplinary team approach, as well as intensive postoperative inpatient rehabilitation.
Patient selection for SDR
Although similarities exist between patient selection criteria of various institutions, there is no consensus. Several factors contribute to the lack of uniformity. Firstly, there are a large number of preoperative parameters that are considered, as highlighted in a recent systematic review on this topic. 20 The ‘ideal’ child that perfectly fits all preoperative categories is rare and so discretion is often necessary based on an individual's overall picture. Secondly, feedback from appropriately designed long-term outcome data is crucial for defining the optimal preoperative selection criteria. However, much like other paediatric interventions that aim to change a condition's natural history far into the future, long-term outcomes that extend into adulthood are difficult to obtain. Thirdly, most clinicians agree that a major goal of SDR in ambulant CP is to improve quality of gait and mobility. Therefore, 3DGA should form a critical component of preoperative selection and postoperative evaluation. However, 3DGA is not used by every centre that performs SDR and is rarely included in studies on indications or outcomes.
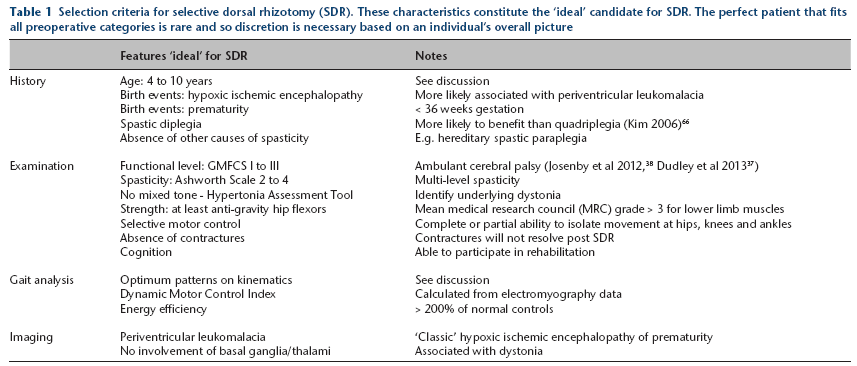
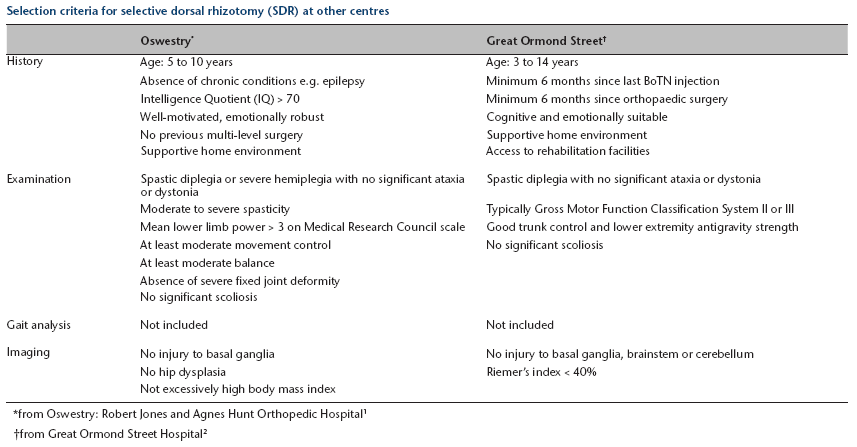
The criteria for the ‘ideal’ SDR candidate at our institution are based on Peacock's pioneering work 15 (Table 1). Short- (18 months) and long-term (13 years) results at our institution based on these criteria have been published previously.21,22 Our criteria here share similar items to those published by other institutions, such as Oswestry 23 and Great Ormond Street 24 (Appendix A). Exceptions include our use of 3DGA and standardized assessment tools of spasticity, such as the Ashworth scale 25 and the Hypertonia Assessment Tool (HAT). 26
Selection criteria for selective dorsal rhizotomy (SDR). These characteristics constitute the ‘ideal’ candidate for SDR. The perfect patient that fits all preoperative categories is rare and so discretion is necessary based on an individual's overall picture
Several items on the criteria list in Table 1 warrant further discussion.
Age
Spasticity is a major limiting factor of function in early and middle childhood. In later childhood and adolescence, surgical correction of lower extremity lever-arm deformities forms an essential aspect of management. 1 Typically, both hypertonia and secondary deformities need to be addressed for optimal results, although each may be more appropriate at different age ranges.
Since one of the concepts of SDR is to train a new gait pattern in the absence of spasticity, SDR is believed to be more effective if performed in early childhood. If performed too late, secondary contractures may develop that could limit effectiveness. Classic studies reporting benefits of SDR were performed in young children generally between four and ten years of age.27,28 MacWilliams et al 6 showed that older patients who underwent SDR between the ages of ten and 20 years experienced functional declines compared with those who did not undergo SDR. Additionally, it is difficult to clearly identify candidacy for SDR in children who are younger than four years. Gross motor function is known to be dynamic in the young child with CP, typically improving up to the ages of six or seven years, with the steepest increase occurring in the first three to four years. 8 Cooperation with physical examination and 3DGA for the very young child is also difficult. These factors contribute to reduced reliability in measuring baseline preoperative functional level and therefore difficulty in projecting long-term outcomes.
Spasticity versus dystonia
SDR only treats spasticity. Therefore ideally, spasticity should be the primary impairment in any candidate for SDR. In reality, it is common for spasticity and dystonia to be co-present in varying degrees. Even though it is critical to differentiate between the two, there is no objective measure universally agreed upon for either entity, especially dystonia. One measure of spasticity is the modified Ashworth scale, which is a scale from 1 (normal) to 5 (rigid). 25 An ‘ideal’ SDR candidate will have scores between 2 and 4 at multiple muscle levels in the lower extremities. Other options for quantifying spasticity include the Tardieu scale 29 and instrumented measures. 30 Dystonia is defined as sustained or intermittent involuntary muscle contractions that cause twisting and repetitive movements or abnormal postures. 31 The HAT is a qualitative tool shown to have moderate to substantial reliability in differentiating between spasticity and dystonia, 26 although validity is not confirmed. 32 Recent efforts to use dynamic electromyography (EMG) on physical examination and during gait have also been attempted, but differentiating between the two remains challenging. 33
Selective motor control
Individuals with CP have varying degrees of impairment in selective motor control. This can manifest as primitive movement patterns (mass flexion/extension), and ‘patterned’ activation of muscle groups when attempting to perform simple motor tasks. Compromise in motor control is not known to improve following removal of spasticity with SDR. Therefore, the ‘ideal’ candidate should have relatively good baseline selective motor control; 3DGA can help differentiate between gait abnormalities due to spasticity or poor selective motor control. 34
Motor control can be quantified statically or dynamically. Physical examination can measure static selective motor control using a scale of 0 to 2, indicating observation of only patterned movement (0), partially isolated movement (1) or complete isolated movement (2) for each muscle. 35 Motor control can be dynamically quantified from analysis of muscle synergy complexity using surface EMG during 3DGA. 36 As measured by the Walking Dynamic Motor Control Index, better motor control is associated with better functional gains following either SEMLS or SDR. 36
Baseline gross motor function
Authors have reported that children who are GMFCS I to III are more likely to benefit than those who are GMFCS IV to V.37–39 This partly forms the rationale for including GMFCS I to III as a selection criteria at our institution, as well as in most studies reported in literature. 20 However, some institutions rarely recommend SDR for children who are GMFCS I, 24 with the concern that the benefits gained may be too small to justify potential risks. In GMFCS III children, concerns regarding potential weakening effects of SDR can also limit selection. Physical examination and 3DGA are important for distinguishing between those children who rely on spasticity to maintain antigravity strength and those who are more impeded by their spasticity. Whilst we do believe that GMFCS II children often form the most ‘ideal’ candidates, the risk/benefit profile of SDR is heavily influenced by the percentage of rootlets sectioned. Around 25% to 40% of rootlets are routinely sectioned during SDR at our institution, which is low comparatively in literature. The higher the number of rootlets sectioned, the less ‘selective’ the rhizotomy procedure is, and the greater the risk of inducing weakness. Yet despite a relatively lower percentage of rootlets sectioned, we see no compromise in spasticity reduction achieved at our institution as assessed on modified Ashworth scale and long-term follow-up.21,22 Therefore, we believe that with careful selection of patients and judicial sectioning of rootlets, a proportion of children who are GMFCS level I or III can also benefit from SDR.
Kinematics on 3DGA
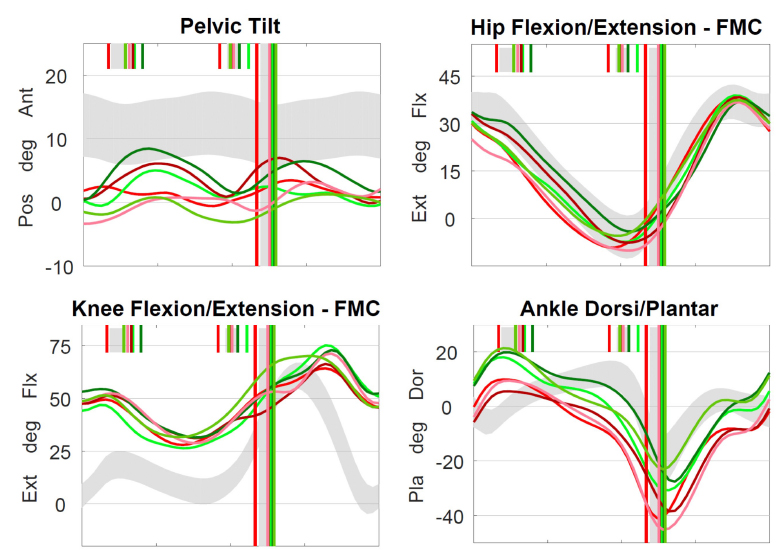
The use of 3DGA kinematics can help objectively identify factors in a child that are either favourable or non-favourable for SDR. 34 As mentioned above, a pattern of ‘mass flexion/mass extension’ movement on the sagittal plane in the hip and knee suggests reduced selective motor control (Fig. 3). Children with dystonia will also have kinematic traces that vary significantly between individual gait cycles (Fig. 4). These factors are non-favourable for SDR, for reasons stated earlier.
Kinematic traces of ‘mass flexion (Flx)/extension (Ext)’. Mass flexion-extension is a primitive movement pattern suggesting reduced selective motor control. This can be seen typically between the sagittal hip, knee and ankle traces during swing. Flexion and extension are abnormally synchronized. Solid blue line represents onset of mass flexion (dorsiflexion in ankle) and dotted blue line represents peak flexion in swing. Red traces: left limb. Green traces: right limb. Long green/red vertical lines: ipsilateral limb foot-off. Short green/red vertical lines: contralateral limb foot-off.
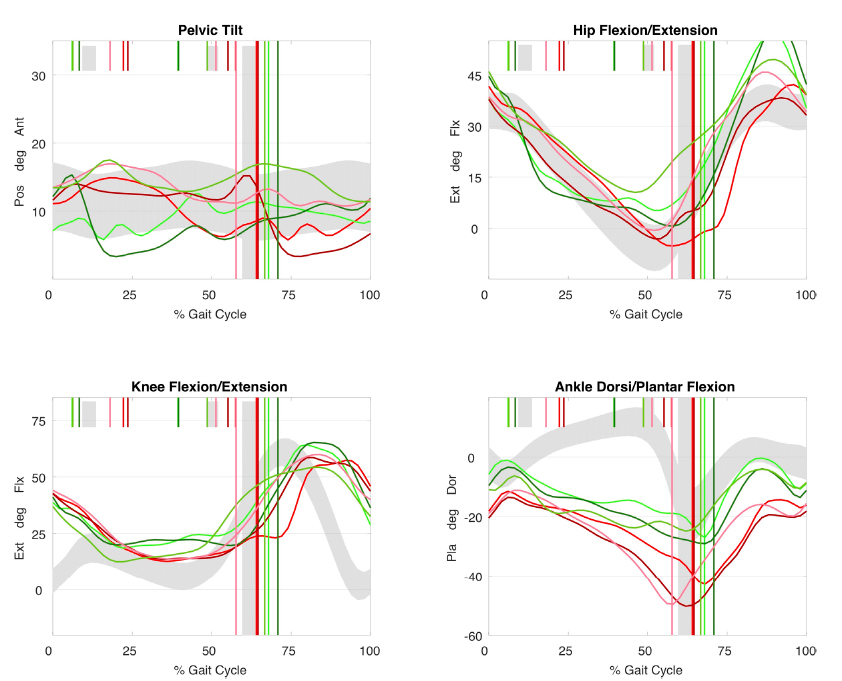
Kinematic traces in dystonia. Uncontrollable movements in dystonia results in large cycle to cycle variations between individual cycles. This individual also walks with plantarflexed gait, foot drop in swing and crouch (Pos, posterior; Ant, anterior; Ext, extension; Flx, flexion; Pla, plantarflexion; Dor, dorsiflexion).
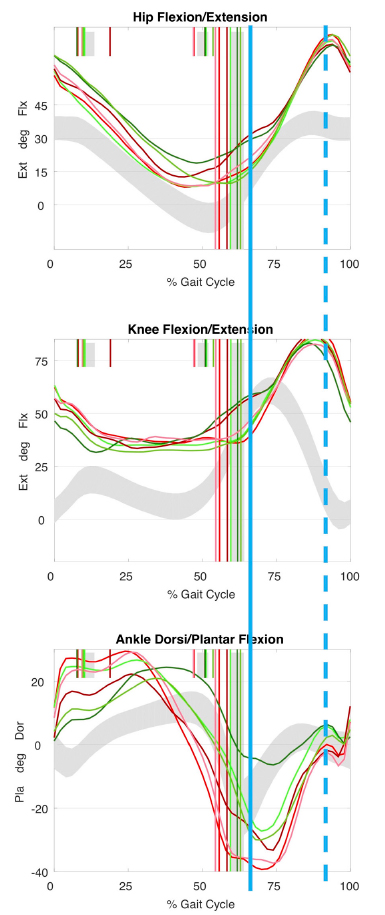
Since tone reduction is the goal of SDR, identification of kinematic patterns consistent with multi-level spasticity is critical. In the lower extremity, muscles most affected by spasticity cross more than one joint, and dynamic stiffness in the affected joints can be demonstrated objectively on 3DGA (Fig. 5). Findings include:
a ‘double bump’ pattern on sagittal pelvic kinematics suggests the presence of underlying psoas or hamstring spasticity; slowed, reduced and delayed knee flexion in early swing is consistent with rectus femoris spasticity; reduced knee extension in late swing associated with posterior pelvic tilt suggests hamstring spasticity; early ankle plantar-flexion on initial contact suggests spastic loading response in gastrocnemius muscles; muscle-tendon modelling derived from joint kinematics can also show reduced length and velocity (Fig. 6).
Kinematic pattern of predominantly underlying spasticity affecting gait. ‘Double bump’ pelvis, slow and delayed knee flexion in early swing, reduced knee extension in late swing and early ankle plantarflexion in stance all reflect spasticity in underlying muscles. The involved muscles are often those that cross more than one joint (rectus femoris, hamstrings, gastrocnemius) (Pos, posterior; Ant, anterior; Flx, flexion; Ext, extension; Pla, plantarflexion; Dor, dorsiflexion).
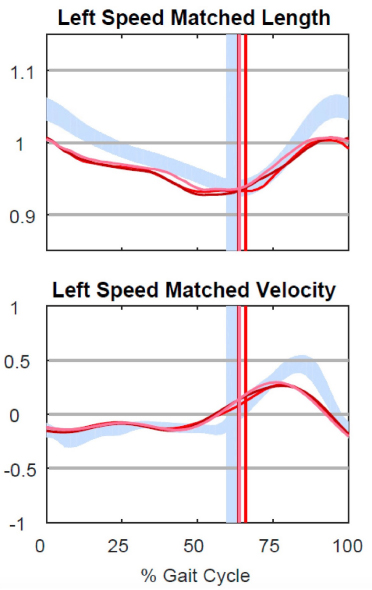
Hamstring length. Musculotendinous length modelling can be performed given known muscle insertions and joint positions. Spasticity is associated with short hamstring length and slow velocity, when matched for walking speed. These are expected to improve following selective dorsal rhizotomy (SDR).
However, restricted range of movement can also be caused by established soft-tissue contractures which would not be expected to improve with SDR. Soft-tissue lengthening procedures may be necessary to address these prior to SDR. Although it may be possible to tease out some of these findings in a detailed physical examination, spasticity is a problem of movement, and therefore a dynamic assessment of the child using 3DGA should provide the best means of quantifying pathology and assessing candidacy for SDR.
Neuroimaging
To identify the ‘ideal’ candidate, brain magnetic resonance imaging (MRI) is essential for determining the presence of periventricular leukomalacia (PVL), and the absence of injury to basal ganglia, brainstem or cerebellum (Fig. 7). 20 PVL compromises supratentorial influences to the spinal neuronal pool, resulting in loss of inhibition to the spinal reflex arcs. PVL is the most common MRI finding in CP and is seen in over 70% of children with spastic diplegia. 40 The highest risk of PVL occurs after birth prior to 32 weeks’ gestation, 41 and hence prematurity is also usually considered part of the selection criteria. Smaller lesions of PVL are limited to the trigonal regions of the ventricles and primarily affect the lower limbs. With increasing severity of injury, larger areas of periventricular white matter are affected, leading to cavitation, cyst formation and ventriculomegaly with thin corpus callosum. In children with these findings, CP is more severe and other factors become more important in limiting mobility than spasticity alone, making outcomes of SDR less predictable. Injuries to the basal ganglia, thalamus and hippocampus are characteristic of hypoxic ischemic injuries, more typical in full-term births. 40 These MRI patterns are associated with dystonia and are therefore not an ‘ideal’ feature in selection for SDR. Screening MRI of the spine are also routinely ordered prior to proceeding with SDR to rule out other anomalies of the neural axis.
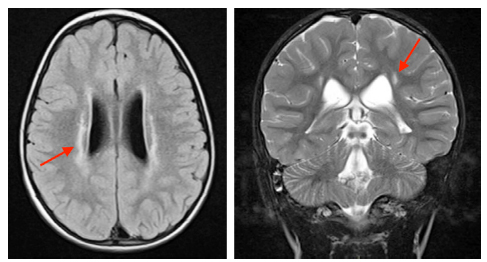
Brain MRI in periventricular leukomalacia (PVL). The ‘ideal’ candidate for selective dorsal rhizotomy will have isolated PVL (red arrows).
Surgical technique
Today, most centres perform SDR using variations of the technique described by Peacock.15,42 The patient is positioned prone and needle EMG sensors are positioned to monitor representative muscles of each myotome, which may include psoas, vastus lateralis, tibialis anterior, peroneus longus and gastrocnemius. The surgical approach is most commonly via a laminectomy or osteoplastic laminotomy from L1 or L2 to S1, which allows excellent visualization of the cauda equina and rootlets. 11 The single-level laminectomy at the level of the conus is a technically more challenging alternative but has the advantages associated with a minimally-invasive approach. 16 Following laminectomy, the plane between ventral (motor) and dorsal (sensory) roots is identified, and ventral roots are protected throughout.
Dorsal roots are then separated into individual myotome levels. Systematic stimulation of rootlets is carried out with a Peacock probe at threshold amplitude, usually with a frequency of 50Hz. Rootlets with abnormal response are sectioned. Responses that are considered abnormal include those that are incremental, clonic, multiphasic, sustained or spread to three or more adjacent levels or to the opposite leg. 21 The total proportion of rootlets resected in some institutions exceed 40%.11,24 However, at our institution, a lower percentage of between 25% and 40% is routine, and near uniform normalization of spasticity is still achieved as measured by our long-term outcomes via the modified Ashworth scale.21,22 In addition, a lower percentage of rootlet resection may reduce risks of side effects of excessive de-afferention such as weakness and sensory abnormalities. Bladder dysfunction is avoided by identifying sacral rootlets responsible for bowel and bladder control using anal sphincter sensors and preserving them.
Irrespective of the surgical approach used or the exact percentage of rootlets divided, it is well established that SDR is effective in spasticity reduction. 43 What remains controversial is whether this translates into long-term functional advantages over other management strategies in tone reduction. Current efforts are now focused on answering these questions.
Outcomes of SDR
Interpreting literature on the outcomes of SDR must take into account several factors. First, the surgical intervention carried out is a permanent one, and will affect the child into their adolescence and adulthood. Therefore, long-term findings are particularly important. Second, the natural history of CP should be considered, including changes in gross motor function and spasticity that may occur with age. Well-matched control groups are therefore critical in comparing SDR with other management modalities. Third, in ambulant children with CP functioning at GMFCS levels I to III, outcome assessment of SDR should include quantitative measurements of gait quality in the form of 3DGA. However, routine 3DGA is not yet the standard of practice. Fourth, global assessment across multiple domains of the International Classification of Function (ICF) is sparsely reported. Even when ICF is reported, the effect on outcomes that family support, income or other social factors may have are often unmeasured or underestimated.
Spasticity
A relatively non-controversial outcome of SDR is its effect on spasticity. 43 Several short-term randomized trials,27,28,44 as well as long-term cohort studies,22,39 have confirmed spasticity reduction following the procedure. However, this information should be understood in light of evidence shed on the natural history of spasticity in CP. Spasticity in the gastrocnemius muscle, as measured longitudinally by a dichotomized Ashworth scale, reached a peak at age four, followed by a gradual reduction up to the age of 12. 7 Since most SDR procedures are performed between the ages of four and ten years, the implication is that the natural history of spasticity at least partially accounts for the improvements seen post-SDR. However, in our long-term study comparing children who underwent SDR with those who had alternate tone management strategies, SDR resulted in uniform reduction of tone on the modified Ashworth scale in all muscle groups down to a normalized score of one, whereas those in the comparison group only showed a partial reduction in spasticity. These findings strongly suggest that SDR produced more additional reduction in spasticity than can be accounted for by natural history alone or by other tone management strategies. 22
Dystonia
One concern regarding SDR is that it may unmask dystonia once spasticity is corrected. Isolated incidents of this occurring have been reported for children with more severe impairment. 10 This concern can be minimized by the careful selection of SDR candidates who show minimal signs of dystonia or mixed tone. As suggested previously, the HAT tool can be used to identify dystonia, but at present, there is no objective and quantitative measurement. Since there is no evidence to suggest SDR reduces dystonia, alternative surgical strategies such as intrathecal baclofen, ventral rhizotomy or deep brain stimulation may be required to address refractory and disabling dystonia.
Functional outcomes
As mentioned previously, studies on long-term functional outcomes of SDR are limited by small sample size, heterogeneous outcome measures, and lack of control groups. Available evidence suggests that SDR confers a modest functional advantage. A meta-analysis of three short-term (9 to 24 months) randomized control trials (RCTs) in 2002 found that SDR combined with physical therapy improved Gross Motor Function Measure (GMFM) more than physical therapy alone. 43 However, when the included studies are looked at separately, only two supported small functional improvements.27,28 The RCT by McLaughlin et al, 44 which had the longer follow-up (24 months) did not show improvement in function, although a reduction in spasticity was still seen. Observed short-term improvements after intervention in a young child must also be placed in the context of gross motor function improvements that are naturally expected up to the age of seven years. 8
A more recent systematic analysis that included cohort studies with more than five years of follow-up found that SDR conferred a modest improvement in ICF body structure and body function domains, but had no influence on ICF activity and participation domains. 45 Of the studies that included a comparison group, Daunter et al 46 showed that SDR was associated with a lesser decline in gross motor function and reduced hours of daily assistance required. However, changes in function were self-rated and it is uncertain whether groups were matched on baseline spasticity levels. Bolster et al 47 showed that compared with reference centiles stratified by GMFCS level and based on GMFM function, no children showed deterioration of function by more than 20 centiles, and a portion showed significant improvement in GMFM scores. Munger et al 22 found that although patients with SDR were not significantly different to a well-matched control group in terms of a variety of quality of life measures at long-term follow-up, SDR did significantly decrease the number of subsequent tone-reduction interventions required, such as anti-spasticity injections and soft-tissue orthopaedic surgeries. 22
When stratified according to preoperative GMFCS level, authors have reported that children who are GMFCS I to III are more likely to benefit than those who are GMFCS IV to V.37–39 This forms the rationale for including GMFCS I to III as one of the selection criteria. It is possible that for a select few, SDR may allow a small improvement in GMFCS level itself. While GMFCS is not intended as an outcome measure, some studies have reported changes post-SDR. Josenby et al 38 found that seven out of 29 patients had an improvement of GMFCS level, and none had deteriorated, but no comparison group was available. While our long-term study had a comparison group that was matched on a variety of baseline parameters, few individuals in each group had both a baseline and follow-up GMFCS level measured. Five out of nine children who underwent SDR had an improvement in GMFCS level at long-term follow-up while only one deteriorated. 22 The control group had neither improvement nor deterioration.
Gait analysis
To our knowledge, three studies to date have investigated the effect of SDR on gait quality using pre- and postoperative quantitative gait analysis. Two of these studies used 2D gait analysis (2DGA),48,49 and only one used 3DGA. 22 Subramanian et al 49 found improvement in some 2DGA gait parameters at one and three years post-SDR, but this improvement was not maintained at ten years. In contrast, Langerak et al 48 found that improvements in range of movement, cadence and step length persisted 20 years post-SDR. At our institution, 3DGA is performed routinely pre- and postoperatively for major interventions. We reported our findings comparing matched groups of patients who underwent treatments with and without SDR. 22 At a median follow-up of 13 years, we found that both SDR and control groups improved in terms of Gait Deviation Index (GDI), mean dynamic knee range of movement and equinus in stance. However, the non-SDR group had a greater improvement in GDI compared with the SDR group at the time of long-term follow-up, likely at the cost of an increased number of orthopaedic interventions.
Pain
Although not a common manifestation of CP during childhood, the prevalence of pain in adults with CP is higher than in the general population.50,51 Some authors have hypothesized that persistent muscle spasticity could be a contributor. 39 However, multiple factors can influence pain or the perception of pain, including comorbidities, previous treatments received, mental cognition and available social support. In addition, SDR is usually done many years prior to the onset of pain, complicating any attempts at causal links. Tedroff et al 39 measured pain and pain interference in 18 adults who underwent SDR as children. While half reported presence of pain, severity and pain interference were judged to be low compared with a general adult CP population, whose SDR status was unknown. 50 Assessments of pain with CP comparison groups by Daunter et al 46 and Munger et al 22 were not able to show pain improvement attributable to SDR. Therefore, further research is needed to evaluate whether SDR can minimize or delay the development of pain in individuals with CP.
Joint and musculotendinous contractures
Although it may improve joint range of movement in the short-term, evidence exists that SDR does not reduce the occurrence of joint contractures in the long-term.5,39 These findings have been a disappointment. Joint contractures may be the result of underlying structural soft-tissue abnormalities that are independent of muscle tone. Abnormal lever-arm dysfunction that affects a child's ability to ambulate (e.g. torsional bony abnormalities, foot deformities and joint dysplasia) are also frequently encountered in CP but are neither prevented nor improved with SDR. Both joint contractures and lever-arm dysfunction usually present later in childhood and require orthopaedic surgery. Therefore, the implication is that, for the majority of children undergoing SDR, at least one or more subsequent major surgical intervention is required.
Hip and spine
Concerns regarding negative effects of SDR on the hip and spine can affect a clinician's recommendation regarding the surgery. At present, there is insufficient evidence to suggest SDR produces any definitive effect. Although spontaneous improvements in hip dysplasia and subluxation have been reported following SDR,52,53 numbers are small and no conclusions can be drawn. A recent systematic review into interventions that may prevent hip dysplasia in CP did not find SDR to have either a positive or negative effect. 54 When hip surgery is required in a child who is otherwise eligible for SDR, timing of such intervention is discussed later in this review.
Reports of postoperative spinal deformity following SDR have raised concerns. However, many of these concerns were from earlier studies that included non-ambulant children and utilized a more extensive dissection.55,56 The high rate of scoliosis in the general CP population and the lack of historical controls compromise ability to interpret causality in these findings. Experience at our own institution does not support increased incidence of scoliosis after SDR. Sagittal plane instability following SDR is another concern. The conus approach advocated by Park and Johnston, 16 is preferred by some surgeons to minimize this risk compared with multi-level laminectomy, but definitive evidence is lacking.
Energy efficiency (EE)
EE during walking is one of the prerequisites of normal gait. 1 Improving EE of gait can be considered a goal of any treatment directed at gait improvement. This forms the rationale for our routine measurement of EE by oxygen consumption before and after interventions. Poor EE is a common finding in patients with CP. 57 The co-spastic and prolonged electrical activity associated with spasticity are theoretically additive. An earlier, unmatched study from our institution suggested that overall, EE improved following SDR. 21 However, these results need to be considered in light of evidence that EE spontaneously decreases with increasing age. 58 In our more recent long-term study with a matched cohort, the improvement in EE for the SDR group approached statistical significance (p = 0.06), while the non-SDR control group did not. 22 The findings are far from conclusive, as variations between patients were large and sample size was small. Unfortunately, EE is rarely evaluated and reported in other outcome studies on SDR.
SDR within a multi-disciplinary, multi-modal approach
A multidisciplinary team working together can help mitigate the effects of CP on gait and mobility. Clinicians should have a clear understanding of the pros and cons of alternate management modalities and communicate together in multi-disciplinary clinics.
SDR and orthopaedic surgery
While SDR is an important tool in tone management, hypertonia is only one aspect of the musculoskeletal challenges faced by individuals with CP. Another aspect is abnormal lever-arm dysfunction, e.g. torsional bony abnormalities, foot deformities and joint dysplasia, which can significantly impede a child's ability to ambulate. These effects are generally seen in later childhood and can only be corrected with orthopaedic surgery. Similarly, joint movement limitations due to established contractures do not improve with SDR, nor does SDR prevent the development of contractures.5,39 When present, contractures can be improved with orthopaedic intervention.
In addition to lever arm and joint contracture correction, orthopaedic surgery also plays a role in the tone management paradigm (Fig. 1). Transfers of spastic muscles, e.g. rectus femoris, can improve knee flexion in swing. 59 Lengthening of persistently spastic muscles can be performed, however, at the potential risk of loss to muscle strength. Although SDR does not reduce contractures, it may reduce the need for soft-tissue surgeries that are aimed at decreasing spasticity.22,37 Institutions that practice a multi-disciplinary, multi-modal tone management approach have the opportunity to optimize options of spasticity control.
The relative timing of orthopaedic surgery and SDR also needs to be considered. If required, orthopaedic surgery is usually indicated at an older age than SDR, when torsional abnormalities and joint contractures are less likely to remodel, and also less likely to recur following correction. In order to minimize impact on rehabilitation following SDR, orthopaedic surgery is not generally performed until at least one year later, with a few exceptions. If hip subluxation is present and progressive, this may need to be addressed prior to SDR. Currently, it is unclear what effect, if any, SDR has on neuromuscular hip dysplasia. 54 However, it is clear that once hip dislocation is established, pain is common and reconstructive options are limited, hence the relative priority this should be given over SDR. Simultaneous SDR and hip reconstruction should be avoided, as one operation will restrict the rehabilitation required by the other.
Another situation for earlier orthopaedic management is when an established equinus contracture is present at time of consideration for SDR. Persistent equinus following SDR can significantly affect rehabilitation. If appropriate conservative measures have been ineffective, a low-dose calf-lengthening procedure can be performed concurrently with SDR to allow plantigrade ambulation during rehabilitation. Tendoachilles lengthening in zone 3 should be avoided, as this can adversely weaken the calf and lead to crouch. 60
SDR and rehabilitation/physiatry
Extensive rehabilitation is required and is part of the SDR protocol in most institutions performing this procedure.24,38,55,61 Physiatrists and physical therapists should be part of the team giving input into the patient selection process as well as communicating to parents regarding postoperative expectations and rehabilitation plans. At our institution, rehabilitation following SDR differs significantly to rehabilitation following SEMLS. Following SDR, patients receive a four- to six-week intensive inpatient programme. Twice-daily physical and occupational therapy commences on day three post-surgery. After discharge, ongoing outpatient therapy continues initially at five days per week, and a tapered programme extends up to one year.
During the early postoperative period, a reduction in sensory feedback can limit the ability of the child in maintaining movement control. SDR may also temporarily unmask underlying weakness, although children with significant preoperative weakness in antigravity muscles should have been excluded from consideration of SDR (Table 1). The rate at which children recover muscle control correlates with GMFCS level, with those who are GMFCS I often rehabilitating faster than those that are GMFCS III. Rapid gains can be expected within the first three to six months following surgery. The goals of physical therapy during this time include strengthening (resistance and endurance), as well as training for a new gait pattern. New orthoses may be required to promote new walking patterns. Good motivation, family support, time and cognition are crucial throughout the process. These should form part of the preoperative considerations for SDR and should also be communicated to the child and family prior to surgery.
SDR and pharmacological tone management
Intrathecal baclofen, oral medication, phenol and botulinum toxin (BoNT) injections have all been used to alleviate spasticity in CP. A detailed discussion on the pros and cons of each modality is outside the scope of this review; however, evidence in recent years has renewed concerns about the efficacy and safety of BoNT injections. Studies from Korea 62 and Australia 63 have shown that repeated injections resulted in reduced improvements in gait and functions. A recent systematic analysis also suggests that the use of BoNT may cause skeletal muscle atrophy. 64
Since SDR eliminates spasticity, the need for anti-spastic injections such as BoNT should be reduced following the procedure. Evidence for this exists. 22 In addition, compared with those children receiving alternative tone management with BoNT and phenol, SDR appears more effective in achieving lasting reduction in tone as measured on the modified Ashworth scale. 22 In light of this evidence and concerns regarding muscle atrophy with repeated BoNT injections, SDR for tone reduction is favoured. Our current preference is to use BoNT as a ‘bridging’ treatment for very young children, followed by SDR at an appropriate age when gross motor function profile matures and ability to participate in rehabilitation improves.
Cause of suboptimal outcomes following SDR
Suboptimal outcomes following SDR can be divided into two broad categories. Those that arise directly as a result of complications from the operation and those that do not.
Complications
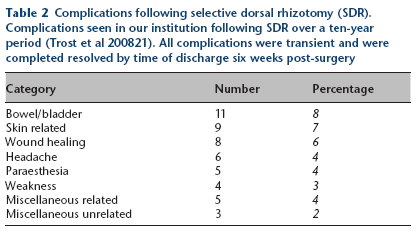
When rootlet sectioning is not excessive (< 50%) and directed by intraoperative electrical stimulation, results from multiple centres have shown that sensation loss, weakness and other neurological compromises are rare.22,48,53 Thus, fears of these neurological complications following SDR may be unwarranted and can be mitigated. Any neurological problems encountered are usually transient. In the earlier years of dorsal rhizotomy where sectioned rootlets exceeded 50%, and when intraoperative decisions were not assisted by electrical stimulation, greater neurological complications were seen.13,14 At our institution, between 25% and 40% of rootlets are sectioned, as a balance between achieving optimal spasticity control while minimizing neurological risks. The spasticity reduction seen with this range is similar to those seen in higher percentage rhizotomies, so we see no additional benefit in increasing this percentage. A comprehensive review of complications from SDR conducted at our own institution over a ten-year period revealed that all complications encountered were transient and resolved by the time of discharge at six weeks post-surgery (Table 2). 21
Complications following selective dorsal rhizotomy (SDR). Complications seen in our institution following SDR over a ten-year period (Trost et al 200821). All complications were transient and were completed resolved by time of discharge six weeks post-surgery
Other causes
Poor outcomes not directly caused by surgical complications of SDR can be avoided by adhering to the multidisciplinary team approach. This will minimize the risk of:
Poor patient selection. SDR only reduces spasticity, and therefore functionally disabling dystonia may be unmasked by the procedure in children with mixed tone. It is also important to identify children with excessive underlying muscle weakness who are dependent on high muscle tone for antigravity joint stabilization. Poor management of lever arm dysfunction. Foot deformity, torsional abnormalities of long bones and joint subluxations are very common and adversely affect joint moment-generating capacity, leading to biomechanically inefficient gait. After SDR, close follow-up with 3DGA is important to monitor for the development of contractures, abnormal torsion and crouch gait. Orthoses and orthopaedic surgery are frequently required to address these. If intervention is too late, the child may suffer severe deformities and irreversible reduction in function. Routine radiographic surveillance for hip dysplasia is required to identify subluxation that can lead to pain and difficulty walking.
Summary and future directions
Modern SDR has now been used in our institution as well as others for several decades. With careful patient selection guided by 3DGA and a multi-disciplinary approach, SDR has been shown to be safe and effective. In the longer term, spasticity reduction is evident and modest improvement or maintenance of function can be expected. The role of SDR may further increase in the future as an alternative to other tone management methods.
However, caution should still be exercised as strength of evidence in this field remains limited, and some recommendations made here rely on institutional experience. Future improvements in evidence to guide practice can be anticipated through:
collaborative, multi-institutional efforts, such as those from the Cerebral Palsy Research Network;
65
the development of improved, quantitative measures of spasticity and dystonia; long-term studies with well-matched control groups.
The advent of the above advancements will be welcomed and will help us further define the role of SDR in maximizing gait and physical function in children with spastic CP.
Footnotes
Acknowledgements
All other authors have no declarations to make.
Appendix A
Selection criteria for selective dorsal rhizotomy (SDR) at other centres
| Oswestry* | Great Ormond Street † | |
|---|---|---|
| History | Age: 5 to 10 years | Age: 3 to 14 years |
| Absence of chronic conditions e.g. epilepsy | Minimum 6 months since last BoTN injection | |
| Intelligence Quotient (IQ) > 70 | Minimum 6 months since orthopaedic surgery | |
| Well-motivated, emotionally robust | Cognitive and emotionally suitable | |
| No previous multi-level surgery | Supportive home environment | |
| Supportive home environment | Access to rehabilitation facilities | |
| Examination | Spastic diplegia or severe hemiplegia with no significant ataxia or dystonia | Spastic diplegia with no significant ataxia or dystonia |
| Moderate to severe spasticity | Typically Gross Motor Function Classification System II or III | |
| Mean lower limb power > 3 on Medical Research Council scale | Good trunk control and lower extremity antigravity strength | |
| At least moderate movement control | No significant scoliosis | |
| At least moderate balance | ||
| Absence of severe fixed joint deformity | ||
| No significant scoliosis | ||
| Gait analysis | Not included | Not included |
| Imaging | No injury to basal ganglia | No injury to basal ganglia, brainstem or cerebellum |
| No hip dysplasia | Riemer's index < 40% | |
| Not excessively high body mass index |
from Oswestry: Robert Jones and Agnes Hunt Orthopedic Hospital 1
from Great Ormond Street Hospital 2