
Abstract
Purpose:
A flexed knee gait is a common gait in children with unilateral cerebral palsy. In children without knee contracture, hamstring spasticity is commonly considered a major contributor to a flexed knee gait. We hypothesized that the popliteal angle would not correlate to a flexed knee gait.
Methods:
This retrospective study included 109 children with unilateral cerebral palsy who had undergone complete 3D gait analysis. Children who had previous surgery or knee flexion contracture were excluded. Children were divided into three groups based on knee position during stance as determined by 3D gait analysis: flexion (FK, 47), hyperextension (HK, 42), and normal (NK, 20).
Results:
There were no significant correlations between popliteal angle and dynamic peak knee extension in stance or at initial contact. Similarly, peak dorsiflexion during the stance phase did not correlate with dynamic peak knee extension in stance (all p > 0.05). Significant differences were observed in foot position during stance between FK and HK groups, as well as in quick stretch dorsiflexion with the knee extended between HK and NK groups.
Conclusion:
A flexed knee gait in children with unilateral cerebral palsy does not always correlate with the popliteal angle or dynamic ankle position in gait. These factors may contribute but are insufficient to explain all observed differences. A flexed knee gait likely involves a complex interplay of motor control, strength, spasticity, and lever arm dynamics, indicating that interventions at a single level may not fully improve dynamic knee extension.
Keywords
Introduction
Cerebral palsy (CP) is a group of neuromotor disorders caused by early injury to brain regions or pathways that control movement. CP affects about 2–3 per 1000 live births and is the most common cause of physical disability in childhood 1 and is characterized by a range of motor impairments, such as spasticity, weakness, and/or dystonia and ataxia that affect the posture and movement of the affected individuals.2,3 A gait disorder in unilateral CP can present with various patterns, depending on the CNS lesion which determines the type and severity of unilateral CP, the distribution and extent of muscle involvement, and the presence of secondary deformities. 4 Spastic hemiplegic CP or unilateral cerebral palsy (UCP) accounts for about 30% of all cases of CP and is associated with unilateral brain lesions 5 which cause asymmetric gait patterns that may affect the stability, and symmetry of walking. 6
The sagittal knee position during the stance phase is often affected in children with UCP and can be divided into three categories: flexed, hyperextended, or normal. Flexed knee gait is characterized by increased knee flexion as compared to the normal range during the stance phase and is further subdivided by the ankle position into jump, apparent equinus, or crouch gait. The knee position in children with UCP may be influenced by various and interrelated factors, such as muscle strength, spasticity, contracture, balance, and coordination of muscles controlling the knee as well as by the position of the hip and foot/ankle during stance.7 –10 In our clinical practice, we have found that the prevalence of a flexed knee gait in UCP is very common, which is corroborated by the study by Wren, who found that an excessively flexed knee gait was present in 37% of children with UCP. 11 Hamstring spasticity and/or contracture has been usually assumed to be the major determinant of a flexed knee gait in UCP, 12 but in our clinical experience, we have not always seen a direct correlation between the magnitude of hamstring spasticity and the presence of a flexed knee gait, leading us to consider that other factors may play a role. When a flexed knee gait becomes limiting to the child, both operative and non-operative treatments are used. It is imperative to understand the primary cause of the flexed knee gait to have a successful outcome. While the deviation may be different for each child, we set out to determine if we could identify a relationship between how physical exam parameters at the knee and ankle, kinematic patterns, dynamic muscle lengths, or muscle velocities influence the knee position during stance. Specifically, we hypothesized that popliteal angle and dynamic hamstring length do not predict the knee position during gait in children with unilateral CP without contractures at the knee.
Materials and methods
Subjects
After an institutional review board approval, a retrospective review was conducted on all children with gait studies performed between November 1993 and September 2019. Children diagnosed with UCP were identified and included in this study. Children with a diagnosis of traumatic brain injury more than 2 years after birth were excluded.
Children were also excluded from this study if they had a history of selective dorsal rhizotomy, significant extrapyramidal involvement, any previous lower extremity surgeries, botulinum toxin-A injection within 6 months prior to the gait study, or knee flexion contracture (passive exam knee extension of less than zero degrees). Only the primarily involved limb was analyzed for this study.
Gait study
The gait study evaluation included a comprehensive history and physical examination, complete kinematics and kinetic analysis, and a video record of the gait. The motion analysis was performed with a 12-infrared camera VICON Motion Analysis System (Denver, CO, USA) with five AMTI Force Plates and VICON Software. The children walked at their self-selected speed, and only the barefoot condition was evaluated. The reflective markers were placed on the specified anatomical landmarks according to the Plug-In-Gait model. 13 Gait cycles were identified, and kinematics were calculated in Vicon Nexus software (Oxford Metrics, Oxford, UK). The kinematic waveforms were time-normalized, yielding a total of 101 data points for each curve. The average of three trials of each subject was used in the statistical analysis.
Musculoskeletal modeling
Kinematic angles from each child were used to calibrate a skeleton based on anatomical data derived by Delp. 14 Data (from the same source) on the origin and insertion (and for some muscles, “via-points” in between) were used to plot the muscles and calculate the length (the linear distances between the chain of points that represent the muscle). The muscle length and velocities were normalized by an individual’s muscle length at the anatomical position so that comparisons could be made among subjects of different sizes.
Statistical analysis
Analysis of Variance (ANOVA) was applied to detect differences among the three knee position groups. Pairwise comparisons were made with Bonferroni’s adjustment. Pearson correlation was utilized to examine the correlation between dynamic minimum knee flexion in stance and popliteal angle and between dynamic minimum knee flexion in stance and peak ankle dorsiflexion in stance. Statistically significant levels were set at 0.05.
Results
Demographics
One hundred nine children (54 males and 55 females) met the inclusion criteria and were included in this study. A detailed description of the children is shown in Table 1. To further evaluate what parameters caused the flexed knee, the children were divided into 3 groups based on their peak dynamic knee extension position during stance: 47/109 children walked with knee flexion (FK), 42 children walked with knee hyperextension (HK), and 20 children walked with their knee position within normal limits (NK). The NK group was defined as peak knee extension in stance within one standard deviation of typically developing children. The FK was one standard deviation greater than typically developing and the HK group was one standard deviation less than typically developing. One standard deviation was chosen because it is common to consider ranges within one standard deviation of norms as typical in gait analysis. See Figure 1 for the dynamic knee position of the three groups. There were no statistically significant age differences among the three groups (p = 0.530) at the time of the motion analysis: FK group was 10.1 ± 3.8 years, HK group was 9.5 ± 3.5 years, and NK was 10.5 ± 2.9 years (Table 1).
Gender and age of the children included in the study divided by knee position.
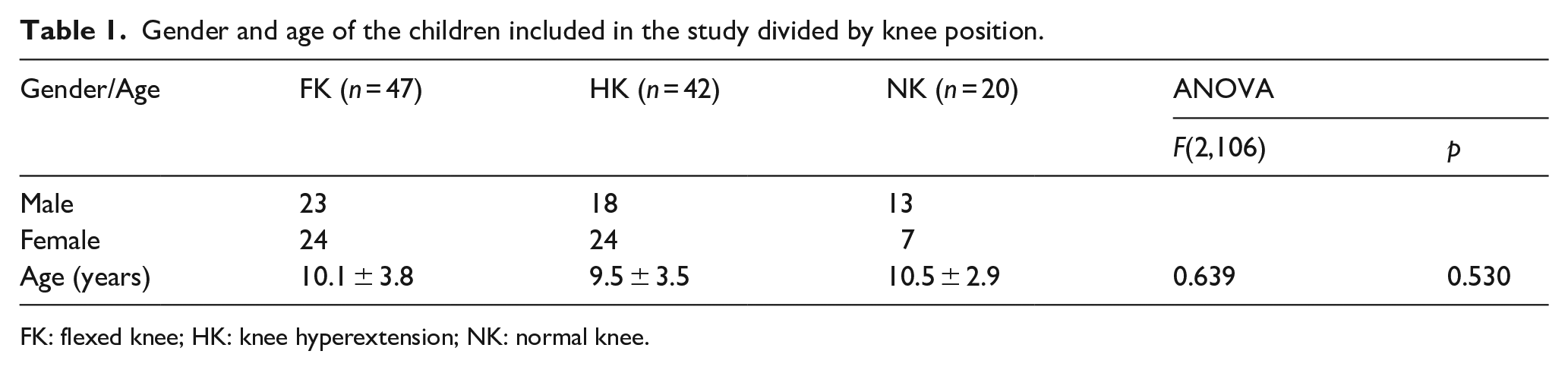
FK: flexed knee; HK: knee hyperextension; NK: normal knee.
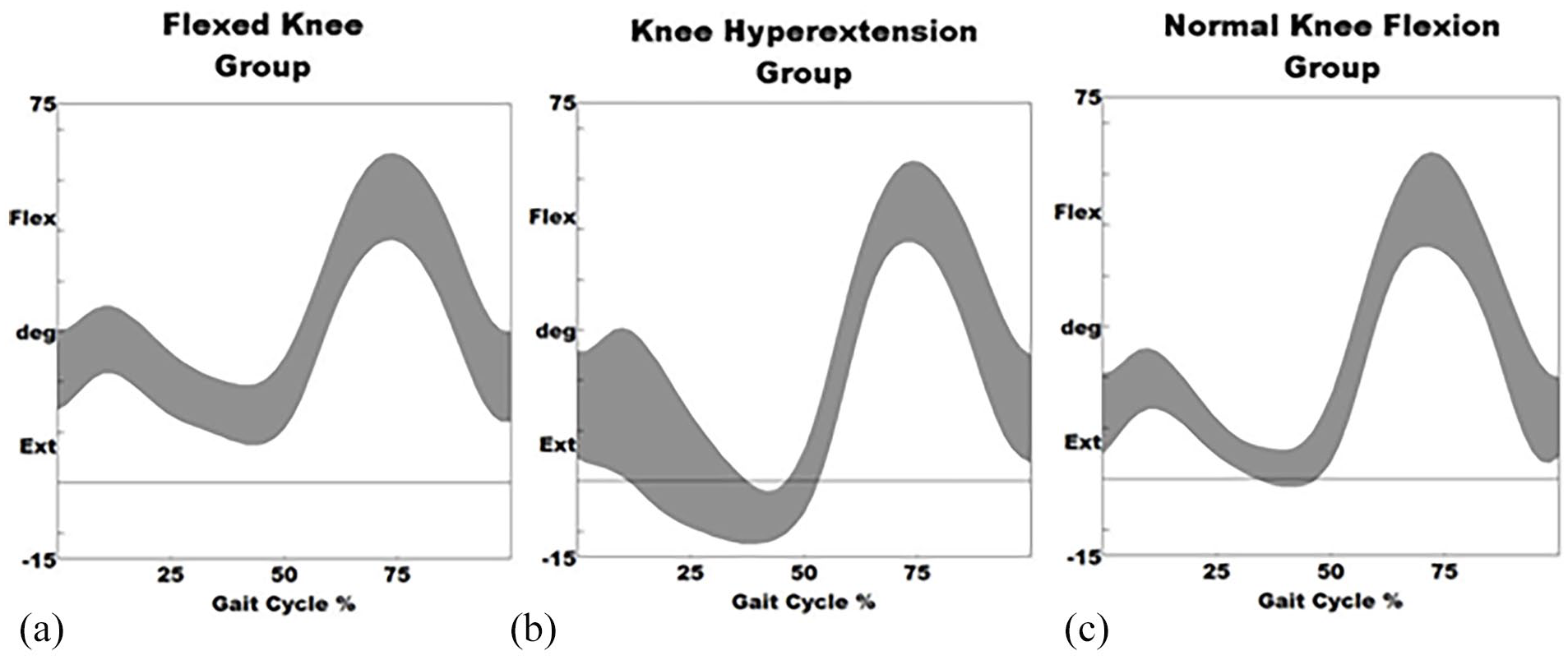
Knee flexion/extension graphs of the three groups divided by knee position, (a) FK group, (b) HK group (HK), and (c) NK flexion group.
In the FK group, there were 32 children with Gross Motor Function Classification System (GFMCS) level 1, 11 with GFMCS level 2, and 4 not recorded. In the HK group, there were 22 children with GFMCS level 1, 13 with GFMCS level 2, and 7 not recorded. The NK group had 16 children with GFMCS 1 and 4 with GFMCS 2.
Physical exam
The following physical examination measures were assessed: knee extension, popliteal angle, dorsiflexion with the knee extended, dorsiflexion with the knee flexed, fast stretch popliteal reflex (R1), and the dynamic component of popliteal spasticity (R2-R1). Of the 109 children identified, popliteal angle and dynamic peak knee extension in stance did not correlate (r = 0.109, p = 0.259). Popliteal angle measured with a quick stretch and dynamic peak knee extension in stance also did not correlate (r = 0.139, p = 0.161). R2-R1 popliteal angle and dynamic peak knee extension in stance did not correlate (r = 0.086, p = 0.391). Popliteal angle and dynamic knee extension at initial contact did not correlate (r = 0.011, p = 0.906). Popliteal angle measured with a quick stretch and dynamic knee extension at initial contact did not correlate (r = 0.142, p = 0.154). R2-R1 popliteal angle and dynamic knee extension at initial contact did not correlate (r = 0.0174, p = 0.079). Peak ankle dorsiflexion in the stance phase and dynamic peak knee extension during stance also did not correlate (r = 0.185, p = 0.054).
ANOVA showed no difference among FK, HK, or NK groups for passive exam measures of knee extension, popliteal angle, popliteal quick stretch angle, and ankle dorsiflexion with the knees either flexed or extended (Table 2). However, there was a significant difference between HK and NK in ankle dorsiflexion with the knee extended quick stretch angle (p = 0.021, Table 2). Out of the 109 children, only 103 had measurements for the popliteal quick stretch angle, and 102 children had measurements for the ankle dorsiflexion with knee extended quick stretch angle.
Summary of passive exam, kinematic, and spatiotemporal parameters divided by knee position (flexed, hyperextended, normal).
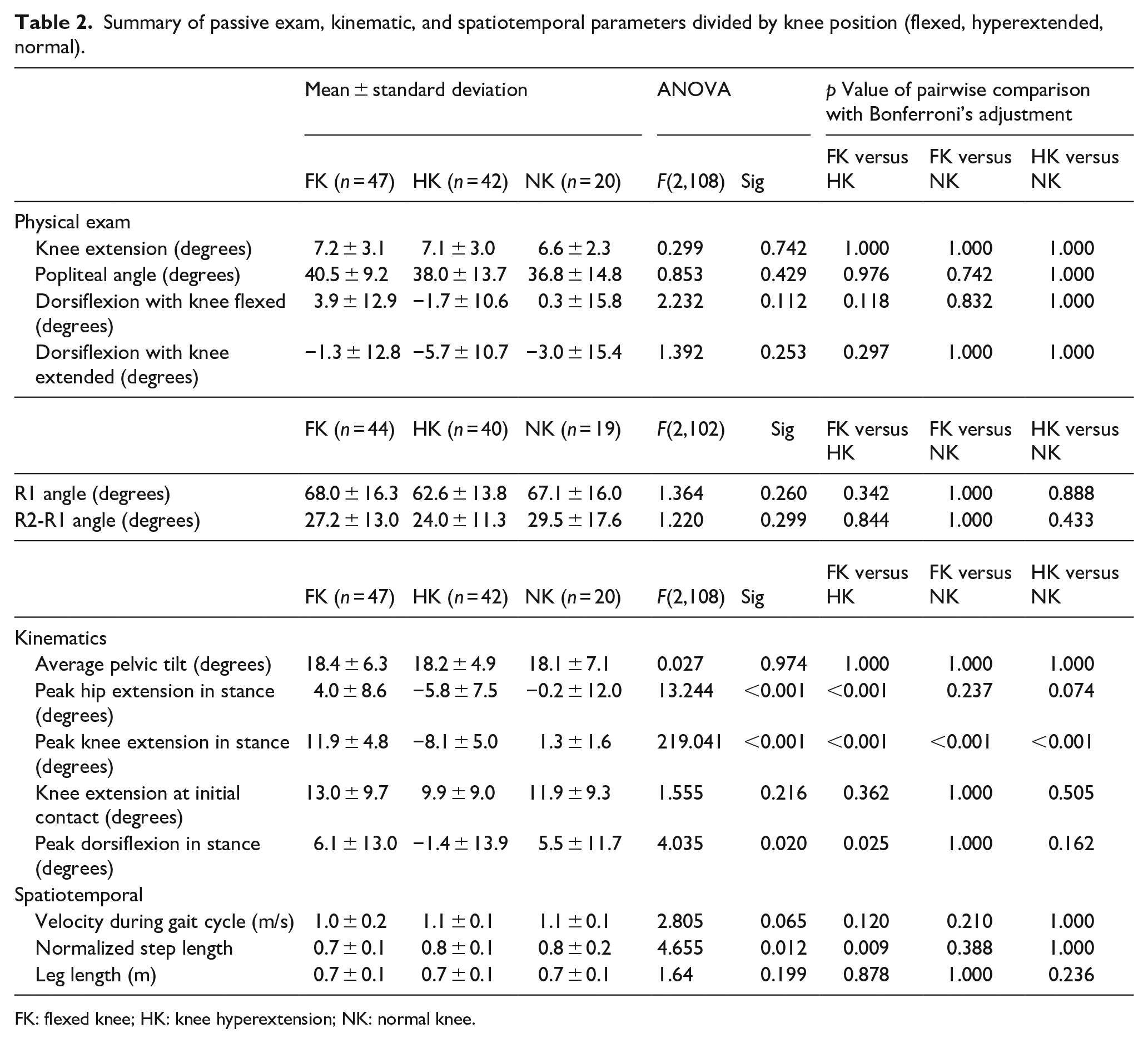
FK: flexed knee; HK: knee hyperextension; NK: normal knee.
Kinematics
There was also no statistical difference among the three groups in the kinematic measures of mean pelvic tilt in the stance and knee extension at initial contact.
There was a statistically significant difference between FK and HK for the kinematic measure of minimal knee flexion in stance (p < 0.001), but this was to be expected since the groups were split by this criterion. There was a statistically significant difference between FK and HK for the kinematic measure of minimal hip flexion in stance (p < 0.001) and peak ankle dorsiflexion in stance phase (p = 0.020, Table 2).
Spatiotemporal parameters
Normalized step length differed significantly between FK and HK (p = 0.012, Table 2).
Muscle modeling
There was statistical significance between the FK and HK for maximum soleus length during stance phase (p = 0.002, Table 3). There was a very weak correlation between peak dynamic soleus length during stance and peak dynamic knee extension in stance (r = 0.265, p = 0.005) and there was a very weak correlation between peak dynamic soleus length in stance and knee extension at initial contact (r = 0.258, p = 0.007). There was no difference in hamstring length or hamstring velocity among the three groups (Table 3). Peak dynamic knee extension in stance did not correlate with peak medial hamstring length in stance (r = −0.038, 0.695). Peak dynamic knee extension in stance did not correlate with peak lateral hamstring length during stance (r = −0.172, 0.074). Dynamic knee extension at initial contact did not correlate with peak medial hamstring length during stance (r = −0.133, 0.166). Dynamic knee extension at initial contact did not correlate with peak lateral hamstring length in stance (r = −0.037, 0.700).
Muscle length and velocity; children were divided by knee position (flexed, hyperextended, normal).
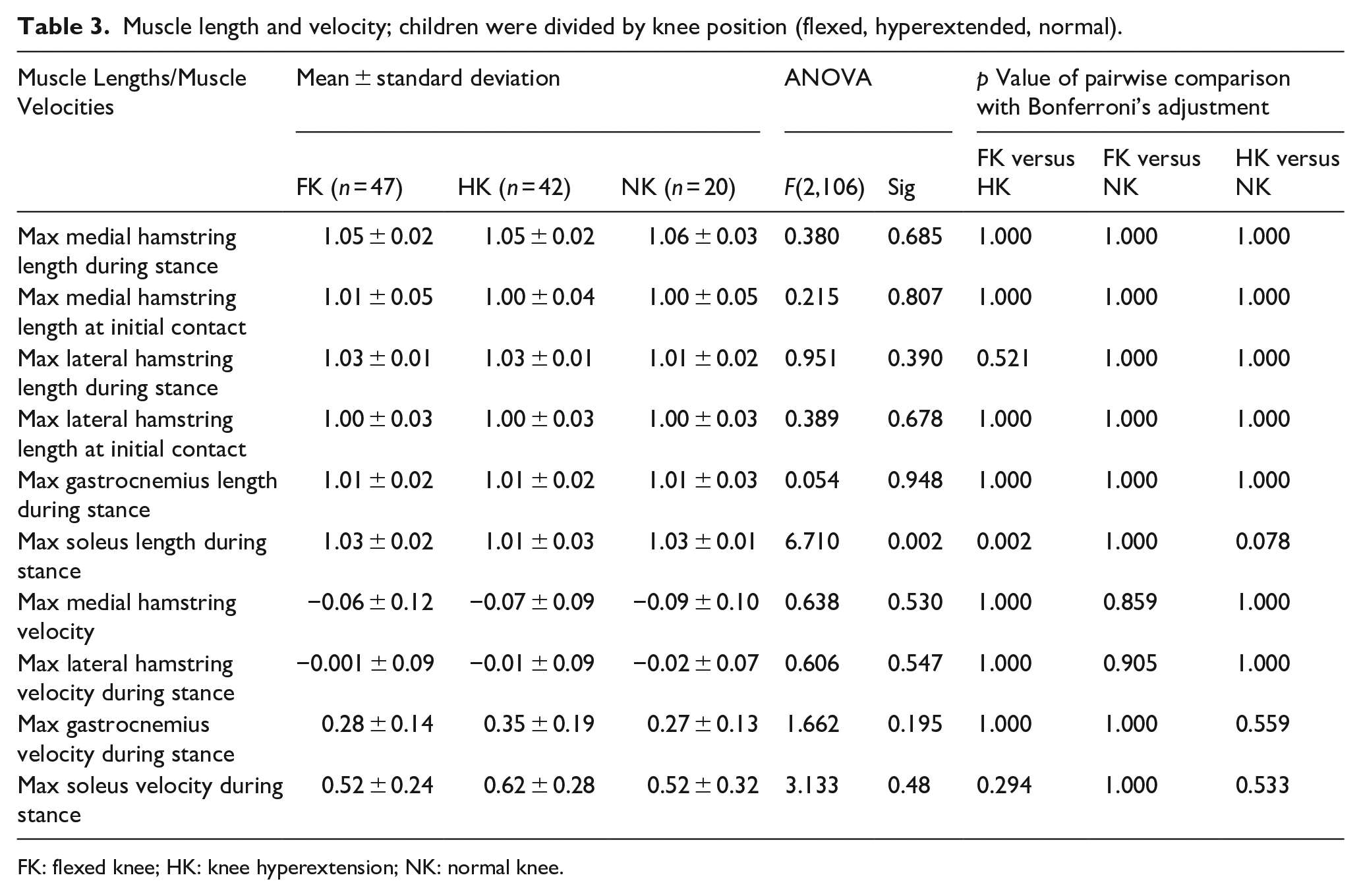
FK: flexed knee; HK: knee hyperextension; NK: normal knee.
Discussion
The purpose of this study was to investigate the primary cause of the flexed knee gait in children with UCP without contractures at the knee. The results showed that there was very weak to no correlation between most of the passive exam measures and dynamic variables examined in this study, indicating other dynamic factors that may influence the gait pattern of these children.
One possible factor that may affect the knee position during the stance phase is the dynamic ankle position. Increased plantarflexion may lead to knee hyperextension due to pathological increased plantar flexion–knee extension couple,15,16 and conversely, increased ankle dorsiflexion and/or calf weakness may lead to a flexed knee position and crouch gait. We observed a significant difference between FK and HK in dynamic soleus length during the stance phase (Table 3). This finding is plausible, as the soleus muscle is a key component of the plantarflexion couple, meaning it is one of the primary muscles responsible for producing plantar flexion movement at the ankle joint, along with the gastrocnemius muscle. The soleus is particularly active when the knee is flexed, making it crucial for plantarflexion during activities such as walking or standing on toes with bent knees. 17
Our data showed a statistically significant difference in peak ankle dorsiflexion during the stance phase between FK and HK (p = 0.020, Table 2), which suggests that increased ankle dorsiflexion with decreased ground reaction force due to decreased plantar flexion–knee extension couple may lead to a flexed knee and crouch gait. Treatment strategies may include using a more rigid AFO to improve knee extension in stance. 18
Our results also showed a difference in quick stretch ankle dorsiflexion with knee extended angle between the HK group and NK group. This suggests that gastrocnemius spasticity may play a role in determining the dynamic knee hyperextension in this cohort.
Another possible cause of a flexed knee gait is dynamic hamstring length, which was not different among the three groups in this study. This suggests that hamstring length was not a determinant of knee position for this cohort. We found no difference among the three groups in the variable popliteal quick stretch angle, which suggests that hamstring spasticity was not the cause of the dynamic knee position in this cohort. While other factors such as subtle differences in muscle strength, balance, and coordination deficits may play an important role in determining the gait pattern of these children, these factors were not evaluated in this study. The literature reports that the dynamic knee position may be influenced by either spasticity or weakness of the hamstrings,8 –10 but children with contractures at the knee were included in these studies.
Understanding the gait patterns in children with UCP is crucial for effective communication among healthcare providers and for guiding appropriate treatment strategies. The initial gait classification system for UCP by Winters identified four primary gait patterns (groups 1–4). 6 This classification was based on observations of 46 children with hemiplegia, of which only 38 had UCP. Later, Rodda and Graham expanded this classification to include four types of gait, with the original Winters and Gauge Group 2 being subdivided into types 2A and 2B. 12 These two foundational classifications, along with subsequent ones, have predominantly focused on sagittal plane gait deviations. The classifications are as follows: Type 1 is characterized by drop foot gait, type 2A by true equinus, type 2B by equinus and recurvatum, type 3 by jump gait, and type 4 by jump gait accompanied by pelvic rotation, hip flexion, adduction, and internal rotation. 12 It is noteworthy that none of these current classification systems include a crouch gait classification. However, several studies have found that the existing gait classification systems are not always able to successfully classify the gait pattern in a child with UCP.19 –21 Because of the inability to reliably classify all children’s gait patterns, treatment recommendations cannot be made based on their gait pattern alone. The results from this study also showed that there was a high prevalence of unilateral crouch gait in UCP, which was not previously described in gait classification systems. In 18 of the 109 (16.5%) children, a crouch gait (excessive knee flexion in midstance and ankle hyperdorsiflexion, greater than one standard deviation of typically developed children) was shown on the involved side. Crouch gait can have negative implications on functional mobility and quality of life for children with UCP, such as reduced walking speed and endurance,22,23 increased energy consumption and fatigue,22 –24 increased risk of falls and injuries, 25 decreased participation in social and recreational activities,23,24 increased joint pain and degeneration,22,23 and decreased self-esteem and body. Therefore, the finding of the high prevalence of unilateral crouch gait in UCP in this study raises awareness and may lead to better classification and treatment planning in the future.
This study had some limitations and biases. First, since this study was retrospective, there was a selection bias due to the inclusion of only participants who underwent gait analysis as part of their pre-operative evaluation. Another potential source of bias was that the measurements of strength range of motion and gait parameters, which were reliant on the investigator’s clinical assessment and may have been compromised by the child’s body habitus. However, all physical exams were carried out by experienced physical therapists with extensive experience in motion analysis. Further, the collected data during gait analysis provided only a snapshot of disease progression rather than any trends over time. Another limitation is the lack of control over walking speed, which has been shown to affect peak hamstring length and peak lengthening velocity. 26 Further research should employ a 3D gait analysis incorporating a foot model to distinguish true ankle dorsiflexion from dorsiflexion resulting from a mid-foot break. Future studies should also explore the longitudinal changes in gait patterns and the effects of interventions such as orthoses, surgery, or physiotherapy on the knee position and function of children with UCP. We are currently exploring the use of a machine learning algorithm to help further classify gait in UCP.
In conclusion, caution should be used when identifying and treating the cause of a flexed knee gait in children with UCP. Flexed knee gait pattern is not solely determined by passive range of motion measures, muscle lengths, muscle weakness, or muscle spasticity, but likely by a complex interaction of multiple factors that affect dynamic joint position during gait. Understanding these factors can help clinicians provide more effective and individualized treatment options for these children.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521251325037 – Supplemental material for Factors associated with flexed knee gait in unilateral cerebral palsy
Supplemental material, sj-pdf-1-cho-10.1177_18632521251325037 for Factors associated with flexed knee gait in unilateral cerebral palsy by K. Patrick Do, Jing Feng and Jeremy P Bauer in Journal of Children’s Orthopaedics
Footnotes
Author contributions
K. Patrick Do: study design, performed measurements, statistical analysis, and manuscript preparation.
Jing Feng: study design, performed measurements, statistical analysis, and manuscript preparation.
Jeremy P Bauer: study design, manuscript preparation.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Board – AACPDM Consultant – Orthopediatrics.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
This study received Institutional Review Board approval from the Western Institutional Review Board (WIRB®), IRB Study No.: 1282868
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.