
Abstract
Purpose
Most children with cerebral palsy classification Levels IV and V in the Gross Motor Function Classification System (GMFCS) are unable to walk and, therefore, spend almost all day in a sitting position in their wheelchairs. As a result of the spastic muscle contraction, malpositions of joints or a scoliosis develop, which require a decision to be made on whether to correct the posture or simply find the best soft bedding position.
Methods
The distribution of pressure on the seat while sitting in a wheelchair was measured with a pressure distribution measuring mat. The different distribution patterns were analyzed.
Results
Pressure distribution measurement allows to find a compromise between posture correction and soft bedding. Additionally, pressure-reducing seats were examined on their effectiveness. We also focused our measurements and data analyses on recognizing the causes for pain. Sometimes, the origin of the problems and pain of children in wheelchairs is not clear.
Conclusions
Using the above-mentioned measuring equipment, the causes of these problems can be detected much more easily than just by clinical examination. The pressure measuring mat can help to optimize the seating position for the spastically handicapped children and adapt technical aids. Examples demonstrate the most frequently occurring problems of these children in their wheelchairs which are typical for neuro-orthopedic diseases.
Introduction
Cerebral palsy is a lasting damage of the yet immature brain before, during, or after birth. This damage is irreversible but not progressive. Depending on the location and extent of brain damage, different multiple handicaps arise, along with the deficiency of motor control and postural function.
Due to spastic contractions of the knees, hips, and the dorsal muscles, the latter often result in neurogenic scoliosis and many of these children are not able to walk. For these children, the wheelchair is the only chance to obtain some mobility.
Sitting in a wheelchair can result in a development of a hip extension and, therefore, a flexion of the pelvis and a tendency to sit solely on the end of the sacrum for the extremely handicapped children. As a consequence of the hypotonic dorsal muscles, a neurogenic scoliosis may develop, along with a loss of postural functions for sitting. Normally, sitting constitutes a dynamic process regulating motor reactions due to endogenic and exogenic influence.
Patients with cerebral palsy cannot continually adapt their sitting posture. However, a variety of seating aids can improve their quality of life.
Therefore, in order to avoid functional problems and pain caused by insufficient seating aids, it is necessary to examine the child very accurately, in particular with regards to the position of the pelvis, and to optimize the sitting aids [1].
The pressure exerted on the bedding of the wheelchair during sitting may lead to displacement of the upholstery material towards the side of the wheelchair. This can be detected with a special measuring mat. The data obtained with the measuring mat show the pressure distribution of the trochanter major and the os ischiaticum on the seat of the wheelchair and helps to detect where special stress on the skin may occur.
Especially so, children with neurologic diseases like spina bifida and cerebral palsy tend to have less sensibility in the lower limbs and overlook the early warning signs of too much pressure on the skin, resulting in decubital ulcer. The local hypoperfusion of the muscles can also cause pain through ischemia [2].
Materials and methods
The study included 72 children and youths aged 2–20 years diagnosed with cerebral palsy and showing symptoms of bilateral spastic cerebral palsy of varying severity. Included are three children with spina bifida and one child with myotonic dystrophia Curschmann–Steinert). They all need a wheelchair either all day (48 of 72) or just outdoors for better mobility (24 of 72).
Twelve of the children are diagnosed with neurogenic contract thoracolumbal scoliosis and windblown deformity (hip ad/abduction deformity, oblique pelvis position, in some cases with hip subluxation) (see Fig. 1). Six of them had Gross Motor Function Classification System (GMFCS) Level IV and six GMFCS Level V. In the following, we refer to these 12 children with severe malpositions of the hip and neurogenic scoliosis who are not able to walk and are equipped with a wheelchair and a seating aid. They all have individually fitted technical supports in their seats or seating aids. These seating aids are developed by a team that includes a physiotherapist, an orthopedic surgeon, and an orthopedic technician. Some of them needed a special support for sitting, in particular, those with a neurogenic collapsing spine.
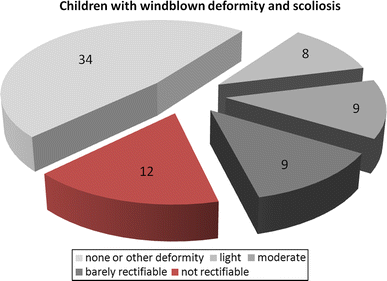
Participants of the study using a wheelchair (n = 72) and their classification of hip malformation associated with scoliosis
The remaining 60 children had GMFCS Levels II, III, or IV. Figure 2 shows the age distribution of all 72 children and youths and their GMFCS classification.
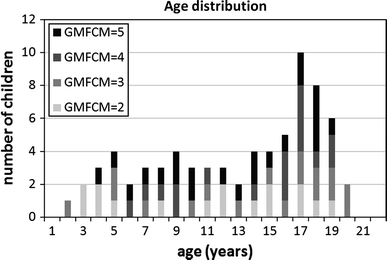
Age distribution of the participants (n = 72) and their Gross Motor Function Classification System (GMFCS) classification
The sitting posture of the children was analyzed with them sitting in the wheelchair, as well as sitting on an examination couch.
The technique used was as follows: the pressure measurement was taken with a pressure measurement mat of dimensions 38 × 40 × 0.3 cm (Novel Pliance, Novel, Munich, Germany). In this mat, 256 (16 × 16) sensors are integrated, which record the pressure data on the seat surface. The measurement rate was 100 pressure distributions per second. The pressure resolution is 0.1 N/cm2.
The measurement period was at least 3 min, during which the pressure reduction with or without the seating aid was examined and the maximum pressure points and local forces with or without the seating aid were localized.
Among healthy persons, in their normal sitting posture, the normal lordosis of the lumbar spine lessens and a lumbar spine kyphosis develops, while the pelvis rotates to a forward position. Rosemeyer showed that a regular sitting position at a 90° angle results in pronounced hip flexion and posterior pelvis position so that the lumbar spine cannot develop a lordosis. With an open angle of 110° or more, the back can position itself against the back rest, which is a more physiological sitting position [3].
Children with cerebral palsy lack the ability to adjust the position of their pelvis. They often show a deformed thorax and asymmetries of the trunk and lower limbs, along with the spastic neurogenic scoliosis. Therefore, the weight will usually rest on the trochanter and the tuber ischiaticum.
The children cannot balance these problems in their seating aids, as they do not have the motor control and ability to send the (sensory) muscle information to the brain and, therefore, cannot adjust their pelvis to a correct position. The active motor control of the pelvis and also of the trunk and the head is necessary for a well-balanced position.
Sitting can be especially difficult for children with hypotonic cerebral palsy. The postural control while sitting is problematic, expressing itself in a stereotypical, nonvariable activation of the muscles and an abnormal muscle increment and excessive antagonistic and co-activation while sitting [4].
The different distribution patterns of pressure were derived while sitting in different wheelchairs (with or without additional devices) or sitting on a normal chair.
The effects of the seat indications and aids were investigated and the effectiveness of the adapted seats and sitting positions were controlled with the Pliance pressure seat mat.
Results
Even though the degree and the peculiarities of the disablement among youths diagnosed with cerebral palsy vary exceedingly, most of the results (of the measuring) can be allocated to particular characteristics in the pressure distribution patterns.
Whereas the main focus in many patients with spina bifida or paraplegics is on preventing decubitus, patients with cerebral palsy primarily require proper adaptation of the wheelchair, respectively, of a seating aid, according to their particular physical deviations from the normal posture. In this, the various goals might be competing or even conflicting.
Our aim is a perpendicular, upright position enabling the child to participate in daily activities, especially in classrooms at school.
Frequently, we would strive also for a certain correction of the posture apart from only obtaining a relaxed and comfortable sitting position for the patient.
Particularly with abduction–adduction contractures (see examples 2 and 3) and neurogenic scoliosis (example 1), the seating aid should prevent further deterioration of the already abnormal posture. It is, therefore, necessary to apply a precisely directed force to a specific point of the skeletal structure, which, by its very nature, implies a reduction of comfortable bedding.
In, for example, stabilizing an abduction–adduction contracture, corrective pressure has to be applied from the sides, showing up as typical pressure marks at the lateral pelvis and the upper thighs in the pressure distribution graph.
In scoliosis, corrective pressure is also usually applied, mostly through side pads in the backrest of the wheelchair.
Dislocations of the hip or malformations of the pelvis/sacrum require graded distribution of the padding pressure underneath the ischiae in order to not further aggravate the malposition, but, rather, use the force of gravity to achieve a certain correction.
Other frequent deviations due to cerebral palsy include contractures of the extensors and flexors of the hip joint, subluxations and luxations of the hip, and pronounced asymmetries of the muscles and the soft tissue if the paresis dominates only unilaterally only. This also shows up as characteristic change in the pressure distribution graph.
The following examples show the most frequent deviations in the pressure distribution among the above-mentioned malpositions.
Example 1: Youth, aged 18 years, diagnosed with tetraplegic cerebral palsy, more pronounced in the legs
Clinically, the patient shows a left convex lumbar scoliosis with a right convex counter swing. If the torso is in an upright position, the left pelvis is lower than the right pelvis. The padding of the wheelchair partly accommodates the malposition caused by the scoliosis by lowering the padding approximately 2 cm on the left side.
The diagram in Fig. 3 shows the equilibrium when sitting on the right ischium. The torque caused by the scoliosis and the countering torque caused by the lopsided sitting position are opposite and equal in magnitude.
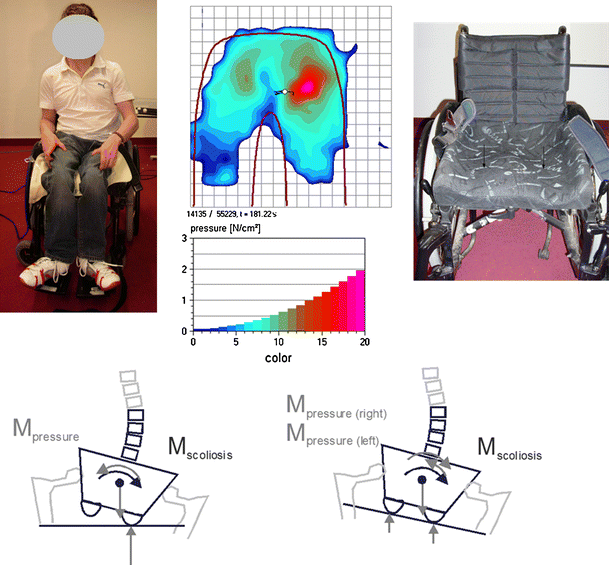
Top tetraplegic patient aged 18 years with lumbar scoliosis; pressure measurement with increased weight-bearing on the left ischium; wheelchair with adapted seat pad. Bottom diagram depicting the torques situation of different seat designs, at worst increasing the scoliosis
The diagram on the right illustrates that a complete adaption of the seat to the postural deviation of the patient and equal distribution of the pressure would, indeed, increase the inner torque of the scoliosis and, thereby, the scoliosis as such.
This can lead all the way to the painful contact of the costal arch with the iliac wing.
The extreme focusing of the pressure on the left ischium is due to the low muscle mass and needs to be considered in the design of the seat padding as well.
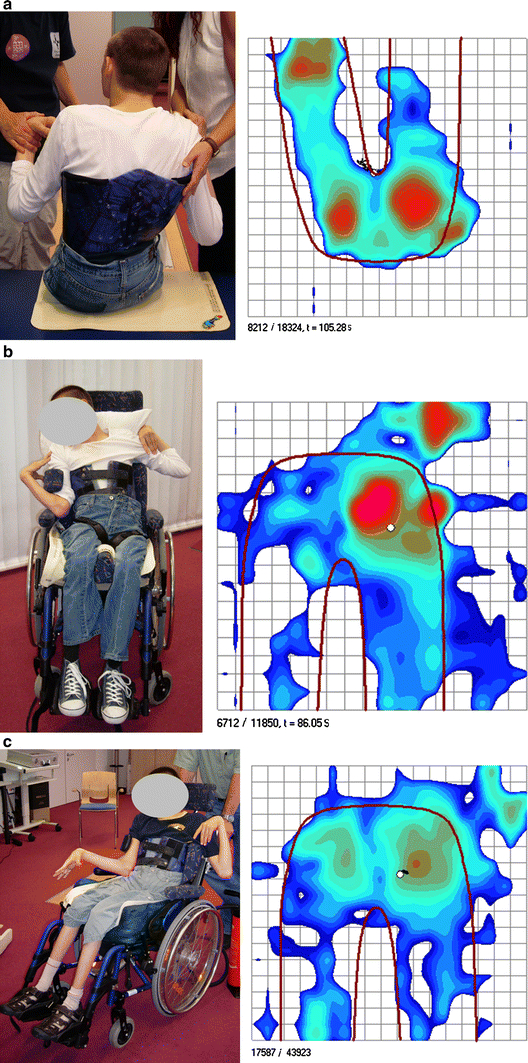
Example 2: Youth, aged 14 years, diagnosed with bilateral spastic cerebral palsy and spastic tetraplegia
The left hip of the patient is dislocated and there is a contracture of the hip adductors and flexors and of the iliopsoas. The range of motion in the hip is reduced to maximal 80° in flexion. The muscle tone, especially in the lower limbs and hip, increases dramatically during speech or other activities. This leads to more hip extension on his right side and to a rotation on the left. He compensates this hip flexion deficit by bending the upper part of the trunk forward to an upright position as far as possible.
The photograph and seat pressure results in Fig. 4a demonstrate the extreme malposition of the hip and pelvis of this patient, which does not allow a perfect and even seat position.
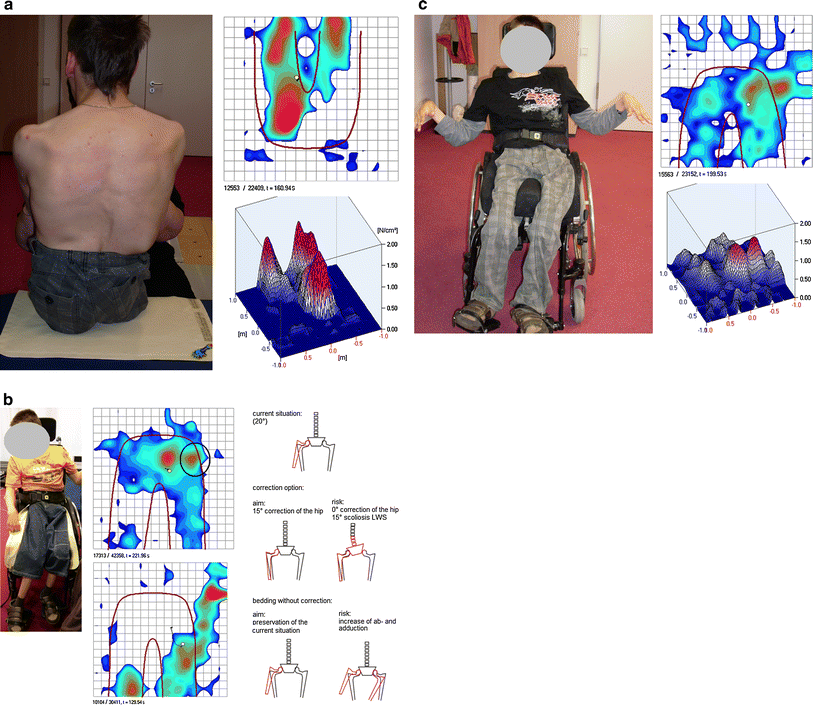
There are two different possible strategies to handle the abduction–adduction position if the child's legs. One is to try and correct the malposition by applying lateral pressure, especially to his left hip. The other strategy would be to accept the malposition and only bed the child in this position. Both treatments may result in adverse long-term effects. Correcting the malposition may lead to pressure marks in the location where the correcting force is applied. The pressure distribution in Fig. 4b already shows a beginning pressure mark located at the left trochanter major. The diagram on the right side of Fig. 4b shows that this attempt of correction might fail because it affects not the hips, but, rather, leads to a faulty posture of the lumbar spine, increasing the scoliosis.
The strategy of purely bedding the limbs, completely dispensing with a correction, on the other hand could result in a further decline of the adduction–abduction contracture.
Figure 4c demonstrates the compromise between both treatment strategies. The patient sits in a slightly corrected position but without trying to fully correct the deformity. The pressure mark in the pressure distribution measurement at the trochanter results from the attempt to correct the windblown deformity (adduction–abduction contracture), but the pressure value is still lower than on the ischiae.
The lower part of Fig. 4b shows the pressure distribution while the patient is intending to speak. The hips then extend and lift the pelvis and pressure is shifted to the distal femurs. The hip abduction of the right leg presses the left hip against the wheelchair.
On account of this unstable situation, further monitoring of the sitting position is necessary in order to react promptly to a change for the worse in either posture or pressure marks.
Example 3: 14-year-old youth with bilateral spastic cerebral palsy
This example in Fig. 5a–c repeats the results of example 2. According to the child's mother, the child showed some discomfort after a longer period of sitting in his wheelchair, which she identified as hip problems caused by the wheelchair. The 14-year-old boy is diagnosed with bilateral spastic cerebral palsy and is not able to walk. As he is unable to speak due to anarthria, he can only point with his finger to the hip to indicate trouble or pain anywhere in this region. The hip was operated on 2 years ago. The musculus iliopsoas and the adductors were extended because of a hip flexion contracture. The hips are 20% dislocated. The pressure distribution measurement in Fig. 5b indicates, just as in the previous example, that his problem very likely originates from the trochanter major. In this case, the pressure values at the trochanter and also under the ischiae are significantly higher than in example 2 and might already result in the long-term risk of skin damage (decubitus). The bone presses against the side of the wheelchair. Therefore, a much better bedding of the trochanter major is needed. The soft cushioned seat in Fig. 5b beds the patient well, but in a position without correction.
Example 4: Boy, aged 12 years, diagnosed with bilateral spastic cerebral palsy
This boy suffers from a permanently increasing spasticity of the extensors in both hip joints. The pressure distribution when sitting unaided (Fig. 6 left and pressure distribution, top) shows that, as a consequence of the pronounced extension of the hip, the pelvis rotates backwards to the extreme, resulting in intensified weight on the sacrum. The highest pressure values are, therefore, to be found at the sacrum. In order to still be able to orient forwards, the patient bends the torso into an upright position. This resulted in a round-back, which is also due to the cerebral palsy and the neurogenic action and has, meanwhile, solidified into a fixated kyphosis.
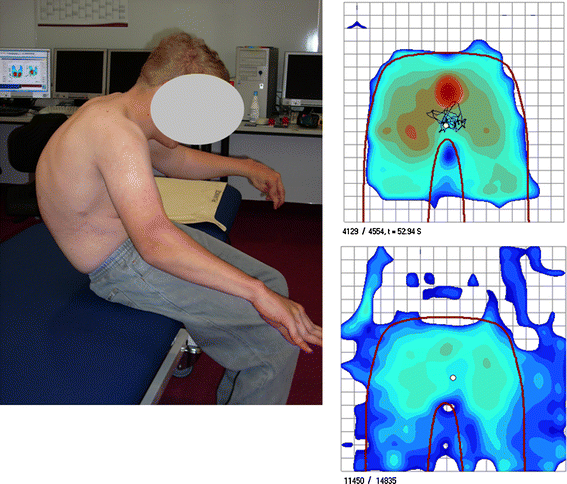
Youth aged 12 years, diagnosed with bilateral spastic cerebral palsy: fixed extended position of the hips, thoracic kyphosis. The upper pressure measurement shows a pressure mark on the sacrum when sitting unaided, as shown in the photograph. The sitting device of the wheelchair distributes this pressure (lower measurement)
A seating aid incorporated into the wheelchair can distribute the pressure evenly and, thereby, release pressure from the sacrum.
Example 5: 16-year-old girl diagnosed with bilateral spastic cerebral palsy
The patient (Fig. 7) permanently needs her wheelchair. Clinically, a severe neurogenic thoracal scoliose appears. A seat pad with back pad and a lateral support for the trunk (mark A in Fig. 7) are required. In this case, both the seat pressure distribution and the pressure distribution on the back were recorded (pressure distribution diagrams in Fig. 7 right). The high location of the thoracal scoliosis does not reflect in the seat pressure measurement, unlike the deep lumbale scoliosis in examples 1 and 2. The lateral support of the seat is intended to stabilize the trunk in an upright position. By integration of the pressure in the area of the support in the pressure distribution measurement (mark A in Fig. 7 right), the correction power can be calculated and controlled (chart in Fig. 7 bottom right).
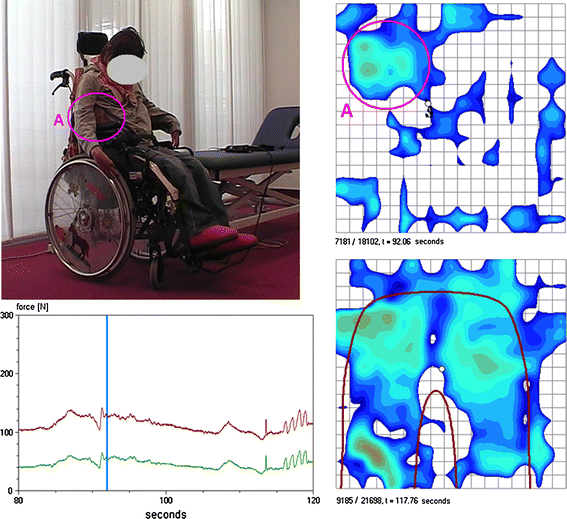
A 16-year-old girl with bilateral spastic cerebral palsy and neurogenic thoracal scoliosis. Upper and middle right pressure distribution of the back and seat, mark A pressure induced by the lateral support. Bottom force diagram, pressing force of the whole back and fraction at the support; vertical mark time corresponding to the back pressure distribution image
Example 6: 19-year-old patient with spina bifida
Patients with spina bifida have a higher risk of developing a decubitus ulcer located around the ischium. Patients supplied with a wheelchair always use special anti-decubitus seat cushions.
In this case, the patient expressed pain at the sacrum and was not able to walk. The examination of the back and sacrum showed no ulcus but a little inflammation of the skin.
The anti-decubitus seat cushion is filled with a silicon gel (Fig. 8). In this case, the silicon gel was too fluid and was squeezed to the sides of the cushion after a longer period of sitting, which means that the patient is then sitting completely uncushioned on the seat of the wheelchair. The comparison of the two pressure distribution measurements in Fig. 7, recorded at a time interval of 2 min, shows the increase of the weight-bearing at the sacrum. Eventually, this is likely to lead to an ulcus.
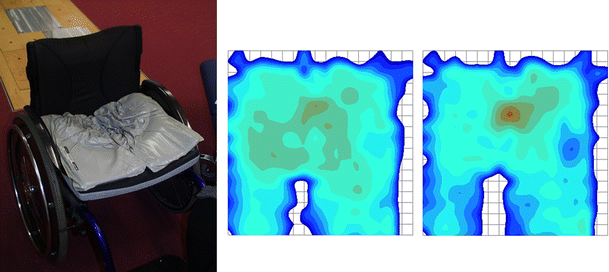
Top anti-decubitus seat cushion filled with silicon gel (thin pillow case stripped off). Bottom left and right pressure distribution measurements immediately after sitting down and 2 min later. The pressure under the sacrum increases with the time of sitting
Discussion
Wheelchairs for children with cerebral palsy should stabilize the patient and slightly correct deformities. Also, with very infaust contractures, we sometimes only have the possibility to cushion the contractures. We look out for influences of the orthopedic devices mounted in the wheelchairs and try to find a better sitting position when we measure the pressure using the pressure measuring mat. Body posture directly influences seating load. Regulating the seating load under the control of a pressure measurement device can also potentially diminish the risk to develop pressure ulcers [5].
There are a number of studies that investigate the effect of seats in handicapped children. They focus on, e.g., seat inclination, giving an improved function in patients with reduced activity [6]. Nielsen et al. [7] studied the, up to now, unknown amount of correction from spine deformity surgery that is required to avoid asymmetric and unbalanced sitting.
Out of a total of 72 patients examined, those with a spastic tetraparesis with distinctly increased muscle tone in the lower extremities and windblown deformity associated with scoliosis (12 children of this study) and unable to walk (like example 1) had the largest problems in the wheelchair. In these cases, the increased tonus led to a diminished ability of hip flexion and was compensated over an increased kyphosis. The abduction–adduction contraction of the hips is connected always with a scoliosis (examples 2 and 3). Only in a few cases (examples 4 and 6) did real risk for rising decubitus problems exist. This problem is commonly more typical for children with spina bifida (three cases in this study, example 6).
In medical care, a permanently applied pressure of 32 mmHg (=0.43 N/cm2) or more is supposed to induce the risk of a decubitus ulcer [8]. If higher values are found in the pressure distribution measurement, a fine-meshed clinical control of the patient is carried out subsequently. With patients who have additional risks such as severe limited motor function or sensory disturbances like spina bifida, pressure-spreading soft materials are used and the seat will be anatomically shaped.
The predominant number of the children with cerebral palsy had no health problems in the actual sense regarding the wheelchair. With them, it was enough to solve ergonomic demands on the wheelchair in order to relieve the use of the wheelchair in everyday life (example 5). Also, no problems with the wheelchair were experienced by those children who are able to walk with crutches, at least for a short distance, and have the diagnosis of a spastic diparesis.
The seat inclination influences the sitting position. In particular, the legs are in a totally different position when changing the backrest of the chair. Nwaobi shows in his study that the orientation of the body effects functional difference in the upper extremities [9].
Our investigation showed that the quality of posture for the child is clearly better when using a bedded seat for patients with a contract hip. The level of pain is reduced.
It is also shown that this kind of pressure measurement is a valid method to check up on the causes of pain and abnormal pressure distribution. It also helps to determine how the pressure distribution can be improved and the pressure on small areas can be avoided by choosing adequate materials for bedding or a different seat position. Throughout all of the children, we find that the data gathered is quite individual, not lending itself to generalization. Nevertheless, we find typical pressure distributions associated with frequent patterns of disability. The symptoms in cerebral palsy vary widely, resulting in quite differently affected muscles and their motions, co-contractions, hip positions, and, therefore, the sitting positions, as such [10].
The figures in the previous samples give sufficient data to reduce pressure under the pelvis. Also, they can be used for optimizing the sitting position and detecting pain.
Through the control and correction of the seating position, if necessary, the intensification of a scoliosis as a result of cerebral palsy via exterior faulty weights can be avoided. The given imbalances of the muscle with consecutive faulty growth caused by cerebral damage can only slightly be detained through adaption of the seating position.
The data were obtained in individual examinations of a larger group of children. The examination itself takes only a small amount of time, meaning that it is a very fast method, while, at the same time, the gathered data is quite useful. The study itself was done at the Integration Center for Cerebral Palsy in Munich in order to supply the patients with improved seating and stabilization of the body in the wheelchair.
From the findings, the following diagnosis and therapy algorithm was derived:
Clinical examination under special consideration of windblown deformity, oblique pelvis position, and scoliosis Assignment of the patients to a risk group Location of pain, e.g., tuber ischiaticum, sacrum, trochanter major Consideration of sensory deficits, e.g., spina bifida Analysis of the wheelchair seat Seat pressure distribution measurement Checkup of the pressure values on exceeding critical thresholds Lateral asymmetry of the pressure load: adequate for the correction of skeletal malpositions or risk of aggravation of the malposition or induction of yet another deformity If necessary, remodeling the seat shell Seat pressure measurement to control of the corrections Followup measurements of the pressure distribution