
Abstract
Background
Medial hamstring fractional lengthening is commonly performed in children with cerebral palsy (CP) to decrease contracture and/or to improve gait. Percutaneous procedures are gaining more and more popularity, even in the paediatric population, with equivocal results. The purpose of this paper was to determine the efficacy and safety of percutaneous medial hamstring myofascial lengthening (PHL).
Methods
This is a prospective randomised controlled trial including 31 knees from 18 consecutive patients with CP scheduled for medial hamstring lengthening in the setting of multilevel tendon lengthening procedures in a university hospital. Other concomitant lower extremity surgeries were not exclusionary. A first paediatric orthopaedic surgeon executes the PHL at one level, as recently described in the literature. Another surgeon opens and extends the wound to explore what had been cut during the PHL and completes fractional lengthening (OHL) of both the semimembranosus (SM) and semitendinosus (ST) when possible. Popliteal angle (PA) was assessed by a third surgeon immediately before PHL, after PHL and then after OHL, using a goniometer in a standardised reproducible manner. All three surgeons were blinded to the others’ findings. Primary endpoints included ease of performing PHL, the percentage of tendon-fascia/ muscle portion sectioned percutaneously and improvement of PA. Comparison between improvement of PA after PHL and OHL was done using a paired t-test with a 95% confidence interval.
Results
The first surgeon was at ease in palpating and identifying the semimembranosus tendon before PHL in ten knees only. PHL led to an undesirable cut of the semimembranosus muscle fibres to more than 50% of the muscle section area in eight cases (<50% in 23 cases, between 50% and 75% in eight cases), and of the semitendinosus muscle fibres to more than 50% in all cases (complete rupture in six cases, more than 75% in eight cases and approximately 50% in 17 cases). Mean PA measured 52° pre-operatively and decreased to 40° after PHL. After OHL, the PA averaged 22°. There was a significant difference between the PA value after PHL (M = 40, SD = 11.8) and the PA value after OHL (M = 22, SD = 8.7), p < 0.0001. The gain in PA did not correlate with the extent of semimembranosus muscle divided (p = 0.38) nor with the extent of semitendinosus muscle divided (p = 0.35). No major iatrogenic neurovascular injury was observed.
Conclusions
To the authors’ knowledge, this is the first prospective study concerning the anatomic effects of PHL. Although it is a quick procedure, it is often associated with difficulty by the operating surgeon to identify and evaluate what should be cut percutaneously, leading to abusive injury of the muscle itself rather than the fascia alone. In addition, the gain in PA is statistically less following PHL than following OHL despite undesirable extensive muscle injury following PHL. This may be due to the multiple fascial cuts (fractional lengthening) usually performed in OHL.
Introduction
The function of the hamstring muscles during gait is complex because they flex the knee and extend the hip simultaneously or separately. Children with spastic cerebral palsy (CP) commonly acquire lower extremity musculoskeletal deformities that may, at some point, require surgical correction.1,2
In children with CP, knee-flexion deformity is common and is caused in part by spastic and contractured hamstring muscles. The common treatment option consists of surgical lengthening of the hamstrings with the goal of increasing knee extension at initial contact.
Medial hamstring tenotomy is a widely used procedure consisting of fractional lengthening of the myotendinous junction of medial hamstring muscles.3,4 Several studies have demonstrated the effectiveness of hamstring lengthening and the procedure is widely accepted for the appropriate patient.5–7 It may be carried out either open (OHL) or percutaneously (PHL).
The type of lengthening can also vary from aponeurotic lengthening to z-lengthening to complete distal tenotomy. Most studies do not specifically define which muscles were lengthened or how they were lengthened, whereas others clearly describe their open surgical technique.6,7 Damron et al 8 perform a percutaneous tenotomy of the semitendinosus, along with OHL and proximal open semimembranosus lengthening.
PHL is a minimally invasive procedure that is alleged to result in less scarring both internally and externally. It has been used, but to a lesser extent than the open release, in the treatment of knee flexion contractures in spastic CP. 9
PHL is reported as a rapid, easy and reliable procedure. Yet, despite its recent extensive use, evidence concerning its efficacy and safety is relatively poor. Moreover, and contrary to OHL, no clear description of the technique can be found in textbooks or articles. With varying techniques and no direct visual control, one may worry about accidental injury to nearby structures such as the popliteal vessels or the sciatic nerve.
There are two types of PHL procedures reported in the literature:
Distal complete tenotomy of both tendons, 10 during which we feel the immediate snapping and proximal migration of the proximal segment with a sudden improvement in knee extension.
Myofascial lengthening at the muscle–tendon junction, 11 derived from the fractional lengthening procedure and supposed to be associated with a better preservation of the hamstring function.
The main purpose of this study was to examine what is truly cut during PHL, to determine its effect on knee extension gain and to compare the latter with the gain produced by OHL.
Methods
After obtaining institutional review board approval, we conducted a prospective study on consecutive patients with CP scheduled for multilevel tendon releases. The group consisted of eight children with diplegia, four children with hemiplegia and six children with paraplegia. The mean age at surgery was 8.5 years (7 to 12). The indication for distal hamstring tenotomy was a primary hamstring contracture leading to a fixed knee-flexion contracture that interfered with the patient's walking ability and physical appearance and persisted even after regular and intensive physical therapy. Children with fixed knee-flexion contracture of 10° or more were excluded and scheduled for distal femoral extension osteotomy.
Each patient received both the PHL and OHL procedures and each side served as case and control at the same time. Routine clinical examination included a popliteal angle (PA) measurement that was repeated under anaesthesia to determine the extent of contracture while allowing palpation of the medial hamstring structures. The popliteal angle is evaluated with the patient supine, the tested limb in 90° of hip and knee flexion and the contralateral limb in full extension. It is represented by the angle formed by the tested leg and the vertical line in maximal possible extension of the knee. The endpoint of the knee extension is determined by the position of knee extension which initiates pelvic rotation.10,12
Three independent surgeons blinded to each other's findings participated in the study: the first surgeon with more than 19 years of experience with multilevel tenotomies in CP performs the percutaneous lengthening; the second undertakes the OHL procedure; and the third is in charge of pre-operative and post-operative PA measurements using a 1° calibrated goniometer (Fig. 1). The PHL procedure is undertaken in a standardised manner, as recently reported. 11 With the patient lying supine, the hip is flexed to 90° and the knee extended under tension with the contralateral limb in extension (PA position). Palpation of the tight medial hamstring at the presumed myofascial junction, i.e. at the level between the middle and distal thirds of the posteromedial aspect of the thigh, is undertaken (Fig. 2). The scalpel blade is inserted parallel to the presumed myofascial junction. It is then turned 90° to produce one transverse cut in the fascia of both muscles consecutively. The blade is then turned back 90° and removed from the incision; the first surgeon then leaves the operating room as the third surgeon scrubs in to measure and record the PA. He then leaves the surgical field as the second surgeon scrubs in to extend the wound, while the patient is still in the supine position, and explore what has been really cut during PHL.

Measurement of the popliteal angle: the angle that the tested limb makes with the vertical line when the knee is maximally extended.
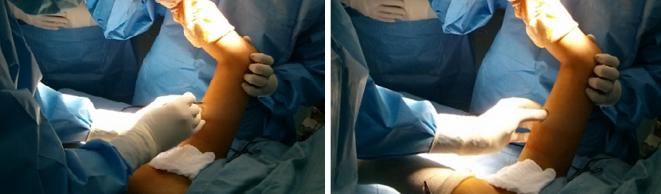
The first surgeon realising the PHL: palpation of the tight medial hamstrings followed by percutaneous transverse cut using a scalpel blade.
He reports the extent of fascial and muscular fibres cut into four categories: complete cut; more than 75% cut; between 50% and 75%; and less than 50% (Fig. 3). He looks for iatrogenic injury to the popliteal vessels, sciatic nerve and to neighbouring muscles, mainly the sartorius. He then completes the medial hamstring fractional lengthening when necessary and invites the third surgeon to come back and measure the PA following OHL, and proceeds with other planned releases.
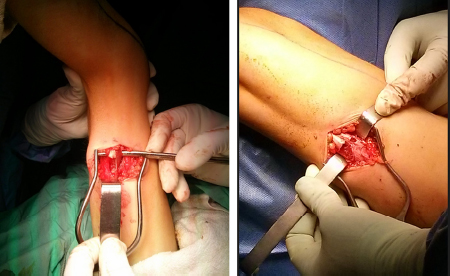
Semitendinosus (
All patients were discharged from the hospital on the day of surgery.
Statistical analysis was done using student and χ 2 tests to look for statistical significance (p < 0.005), with confidence intervals of 95%. We looked for a difference in knee extension resulting from PHL and OHL. We also searched for an association between the extent of tendinous and muscular section and the effect on knee extension. Right and left sides were compared to assess for influence of the hand dominance of the surgeon.
Results
The study included 31 knees in 18 patients (eight boys and ten girls).
Mean pre-operative popliteal angle was 52° (26° to 70° ± 14°) and decreased to 40° (20° to 60° ± 12°) after the PHL procedure (p < 0.0001), and to 22° (10° to 45° ± 9°) after the OHL procedure (p < 0.0001).
The first surgeon was at ease in palpating and identifying both medial hamstrings before PHL in ten legs only.
The tendinous and muscular fibres of the semimembranosus muscle were cut to more than 50% in eight cases (25%). There was no correlation between the degree of tendinous portion cut and the gain in knee extension (p = 0.38) (Fig. 4).
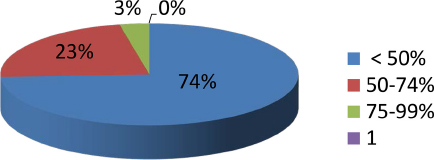
Representation of semimebranosus fascia/muscle sectioned by PHL. The pie chart shows the percentage of patients within each group. The key shows the percentage muscle sectioned for each group.
The tendinous and muscular fibres of the semitendinosus were completely cut in six cases (19%), to more than 75% in eight cases (25%) and to around 50% in the remaining 17 cases (55%). There was no correlation between the degree of tendinous portion cut and the gain in knee extension (p = 0.35) (Fig. 5).
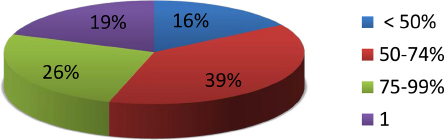
Representation of semitendinous fascia/muscle sectioned by PHL. The pie chart shows the percentage of patients within each group. The key shows the percentage muscle sectioned for each group.
We found no correlation between the side (right or left) and the extent of myofascial cut (p = 0.157 and p = 0.248 for semimembranosus and semitendinosus, respectively) or popliteal angle improvement (p = 0.151) following PHL, showing that the surgeon's dominant hand does not affect the result.
There were no accidental injuries to the surrounding muscles and no neurovascular complications.
Discussion
Hamstring lengthening remains a mainstay of surgical treatment in children with CP.
To our knowledge, no earlier study has been undertaken to evaluate the effect of PHL on knee extension despite its recent and increasing use. Medial hamstring lengthening was investigated by many studies in the literature, however, the results were inconclusive due to significant heterogeneity of the populations tested.10,11 Moreover, this procedure is rarely clearly described in textbooks and surgical atlases, and its anatomic basis has never been clearly illustrated. Our study describes the anatomic effects of PHL and its influence on the PA improvement. Evaluation of its long-term effect on knee extension and gait was beyond the scope of this paper.
By combining minimally invasive multiple soft-tissue and bony operations in children with spastic CP, some authors found immediate clinical advantages when compared with the conventional multilevel surgery. The operative time, and therefore the anaesthetic time, were significantly reduced. This is the main reason behind the increased trend towards PHL procedures in children with CP.
The effectiveness and safety of other percutaneous tendinous procedures have been evaluated.
The first in line is the one related to Achilles tendon. Few complications have been reported following this procedure.13–16 In fact, some tendinous and neurovascular structures are, on average, less than 1 cm from the nearest margin of a given hemi-section and are, therefore, at risk including the flexor hallucis longus, the tibial nerve and the sural nerve.
The main purpose of our study was to assess the effectiveness and safety of PHL in children with CP.
Several studies have demonstrated improvements similar to the present study for knee extension.2,3,7,17 DeLuca et al 4 reported a significant change in knee extension at initial contact with their ‘medial hamstring only’ group. Their procedures were well described as open intramuscular tenotomy of the semitendinosus and gracilis and a stripping of the semimembranosus.
Percutaneous lengthening at the musculo-tendinous junction has been reported to maximise preservation of muscle strength and speed of post-operative mobilisation. 18 Gordon et al 10 concluded that PHL was a useful option in ambulant children with CP undergoing a variety of concomitant operations. They reported significantly improved knee extension at initial contact, but there was no group with an OHL procedure for comparison.
In our series, palpating and identifying both medial hamstrings through the skin was very difficult in the majority of cases (70%). The increased subcutaneous fat encountered in overweight patients may render identification of the tendons almost impossible. This probably explains the high percentage of muscle belly sectioned inadvertently, leading to unnecessary injury to the muscle itself rather than the fascia alone.
Knee hyperextension or recurvatum has been observed as a potential negative effect of hamstring lengthening. 6 In our study, PHL leads to unacceptable damage to the muscular portion of both the semimembranosus and semitendinosus and this could result in persistent hamstring weakness in the long term. However, we found no correlation between the PA gain and the extent of section of semimembranosus and semitendinosus muscles.
The gain in PA is significantly less following PHL than following OHL despite undesirable extensive muscle injury following PHL. This may be due to the multiple fascial cuts (fractional lengthening) usually performed during OHL.
The main limitation of this study was its small patient population. The initial plan was to include a minimum number of 50 limbs, but owing to the negative anatomic effects recorded by the second surgeon involved in assessing what was cut during the PHL, it was decided to stop the study at its current stage.
The hamstrings are very vulnerable to persistent loss of strength after surgery. This is despite prolonged and extensive rehabilitation with an additional resistance strengthening programme to which other lower limb muscles responded well. 19 This stresses the importance of limiting lengthening to fascial portion of hamstrings with rigorous open surgical technique.
Both PHL and OHL provide significant improvements in PA in children with CP. However, the PHL technique results in unacceptable muscle damage and less gain in knee extension.
Although PHL is a fast and simple procedure, it cannot be recommended in routine surgical management of CP children with medial hamstring contracture as it is not as anatomically effective and safe as the OHL procedure.
Footnotes
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
An informed consent was obtained from all individual participants included in the study.