
Abstract
Abstract
Purpose
The purpose of this study was to identify the correlation between the vascular development of the femoral head and avascular necrosis (AVN) in patients with developmental dysplasia of the hip (DDH) treated by closed reduction (CR).
Methods
We retrospectively reviewed 78 patients with DDH treated by CR (83 hips). The vascular maturity, number of vessels and perfusion changes of the femoral head were assessed on perfusion MRI (pMRI) before and after CR.
Results
The number of vessels (mean 4.2 sd 1.4) of the femoral head and the ratio (36.1%) of mature vessels (type III) on the dislocated side were significantly less than those at contralateral side (mean 6.0 sd 1.2; 82.2%) (p < 0.001). Of the included 83 hips, 39 hips (61.5%) showed decreased perfusion of the femoral head, including partial decreased (Class B, 47.0%) and global decreased (Class C, 14.5%), at the dislocated side, which was significantly more than those at contralateral side (0.0%) (p < 0.001). In total, 32 out of 83 hips (38.5%) developed AVN. The rate of AVN with Class A (18.8%) which perfusion of the femoral head was normal (unchanged or enhanced) was significantly less than those with Class C (66.7%) (p = 0.006).
Conclusion
The vascular development and perfusion changes of the femoral head on the dislocated side are significantly worse than those at contralateral side. Immature vascularity of the femoral head before CR and poor perfusion of the femoral head after CR may be risk factors for AVN in patients with DDH.
Level of evidence
III
Keywords
Introduction
Developmental dysplasia of the hip (DDH) is a common disorder of the hip joint characterized by an abnormal anatomical relationship between the femoral head and the acetabulum. Avascular necrosis (AVN) of the proximal femoral epiphysis is a potential complication in children with DDH managed by closed reduction (CR). The goal of treatment is to achieve early, stable reduction of the hip joint and to avoid AVN as it can lead to early degenerative arthritis and may ultimately require hip salvage surgery or hip joint replacement.1–6
The reports of AVN in children with DDH treated by CR vary between 0% and 67%. Severity of hip dislocation, 7 , age, 8 traction, 9 ossific nucleus 10 and adductor release 11 have been reported as risk factors for AVN in children with DDH treated by CR. Most authors agree that the blood supply of the femoral head was disrupted is a key factor for the occurrence of AVN. Perfusion MRI (pMRI) was used to evaluate the vascular development of the femoral head.12,13 Previous studies have shown that pMRI can predict the occurrence of AVN in children with DDH after CR.14,15 However, the number of cases included in previous studies was small, and signal changes of the femoral head only were assessed in previous studies but not vascular pattern of the femoral head.
The aim of this study was to evaluate: 1) the vascular pattern of the proximal femoral epiphysis such as vascular type, number of vessels and quality measured on pMRI before and after CR in children with DDH treated by CR and spica cast immobilization; and 2) the correlation between vascular pattern of the proximal femoral epiphysis and AVN.
Materials and methods
After obtaining approval from our institutional review board, we retrospectively reviewed the medical records of 166 patients diagnosed with DDH and treated with CR and cast immobilization at our centre between November 18, 2017 and April 26, 2019.
The inclusion criteria were as follows: 1) diagnosis of DDH; 2) complete clinical and radiographic data including MRI and anteroposterior radiographs before and after CR; 3) at least 12 months of clinical follow-up.
Exclusion criteria were as follows: 1) concomitant diagnosis of cerebral palsy, arthrogryposis multiplex congentita, myelomeningocele, tethered cord syndrome or other neuromuscular condition; 2) failed closed reduction and changed to open reduction; 3) incomplete clinical and radiographic data.
A total of 78 out of 166 (46.9%) patients (63 girls, 15 boys; 83 hips) met the inclusion criteria. The left was involved in 44 patients (56.4%) and the right hip was involved 29 patients (37.2%), respectively; five patients had bilateral involvement (6.4%). The mean age at the time of CR was 16.6 months (sd 7.3; 4.3 to 33.5), and the mean follow-up time was 21.0 months (sd 6.9; 12.0 to 34.4).
CR was performed under general anaesthesia in all cases. Arthrogram of the hip joint was performed to evaluate the hip position and to assist reduction. Adductor tenotomy was performed if the adductor was considered an obstacle to CR. After CR, a hip spica cast was applied for three months in order to maintain reduction, and it was changed once after six to seven weeks. After cast removal, patients were placed into an abduction brace for additional six months (three months full-time and three months night-time use only).1,5
Radiographic assessment
All patients were followed up for at least 12 months. pMRI was obtained prior to and within 48 hours after CR in all patients. Anteroposterior pelvis radiographs in neutral position were obtained prior to CR, immediately after CR and at each follow-up visit. Acetabular index (AI) was measured on anteroposterior pelvis radiographs prior to CR and at last follow-up visit. 16
The severity of hip dislocation was rated according to the Tönnis grading system. 17
Anteroposterior and frog lateral radiographs taken at last follow-up visit were used to evaluate the primary outcome measure, namely, if AVN was present or not. AVN of the femoral epiphysis was graded according to method described by Kalamchi-MacEwen. 13
Two independent raters (WJ and LY) evaluated AVN. If they could not come to an agreement on the type of AVN, a discussion with at least three other senior paediatric orthopaedic surgeons (CF, XH and Liu Yuanzhong) was performed.
Vascular development of the proximal femoral epiphysis
pMRI examination was performed using a 1.5T Philips Gyroscan Achieva MRI system (Philips, Best, The Netherlands) with the standard examination including the whole pelvis and proximal femur with axial, sagittal and coronal plane sequences. The pMRI examination was carried out prior to and after CR for 48 hours under sedation or general anaesthesia with the patients placed supine and with a body array coil placed anterior and posterior to the pelvis.
The sequences included T1-weighted spin-echo images (repetition time/echo time 372/7 milliseconds, time of acquisition 4 minutes 28 seconds) in the coronal and sagittal planes and T2-weighted fast fifield-echo (repetition time 369 milliseconds; echo time 14 milliseconds, time of acquisition 3 minutes 16 seconds, flflip angle 25°) in coronal and sagittal planes. All sequences used a 22-cm fifield of view, 3-mm slice thickness, 0.4-mm slice gap, 384-384 matrix and 2 for the number of excitations. Gadolinium diamine injection (0.2 ml/kg) was used as contrast agent to conduct cross-sectional, coronal and sagittal enhanced scanning (T1WI SPIR+C). pMRI images of the pelvis and proximal femur were obtained including coronal plane, sagittal plane and cross section. The images were transmitted to the imaging diagnostic system (picture and archiving communication system (PACS), Beijing, China).
All radiographic assessments were performed using the standard PACS software.
The type of vessels in the femoral head was assessed on pMRI before CR according to the method reported by Barnewolt et al. 18 Pattern of vascular canals is initially parallel (type I) but becomes radial with progressive development of epiphyseal ossification center (types II and III). Physis enhances markedly in types I through IV. Physis of secondary centre of ossification is seen best in type III, and it was divided into type I, type II and type III, and vascular maturity gradually increased (Fig. 1a) the number of vessels of the femoral head (Fig. 1b).
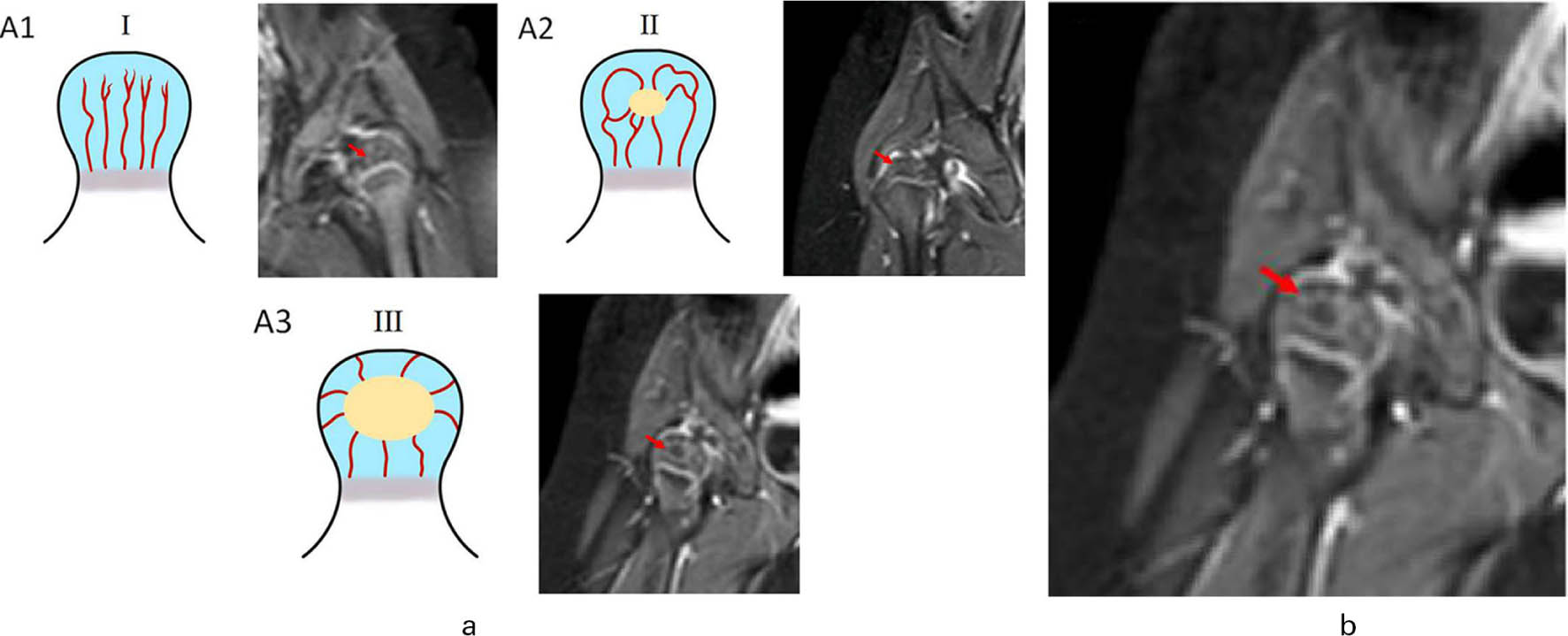
Evaluation of the vascular type and number of vessels of the femoral head on perfusion MRI before closed reduction: a) schematic diagram of the vascular type of the femoral head (A1 type I; A2 type II; A3 type III); b) schematic diagram of the measurement of the number of vessels of the femoral head. The red arrow points to the vascular shadow.
pMRI (T1WI SPIR+C) after CR was used to evaluate the perfusion changes of the femoral head after CR. According to the criteria reported by Tiderius et al, 15 there were three types of perfusion changes of the femoral head: (type A) the global perfusion of the femoral head remained unchanged or enhanced, indicating good perfusion of the femoral head (Fig. 2a; type B) perfusion of femoral head was partially decreased, indicating mild deterioration perfusion of femoral head (Fig. 2b; type C) perfusion of femoral head was globally decreased, indicating poor perfusion of the femoral head (Fig. 2c).
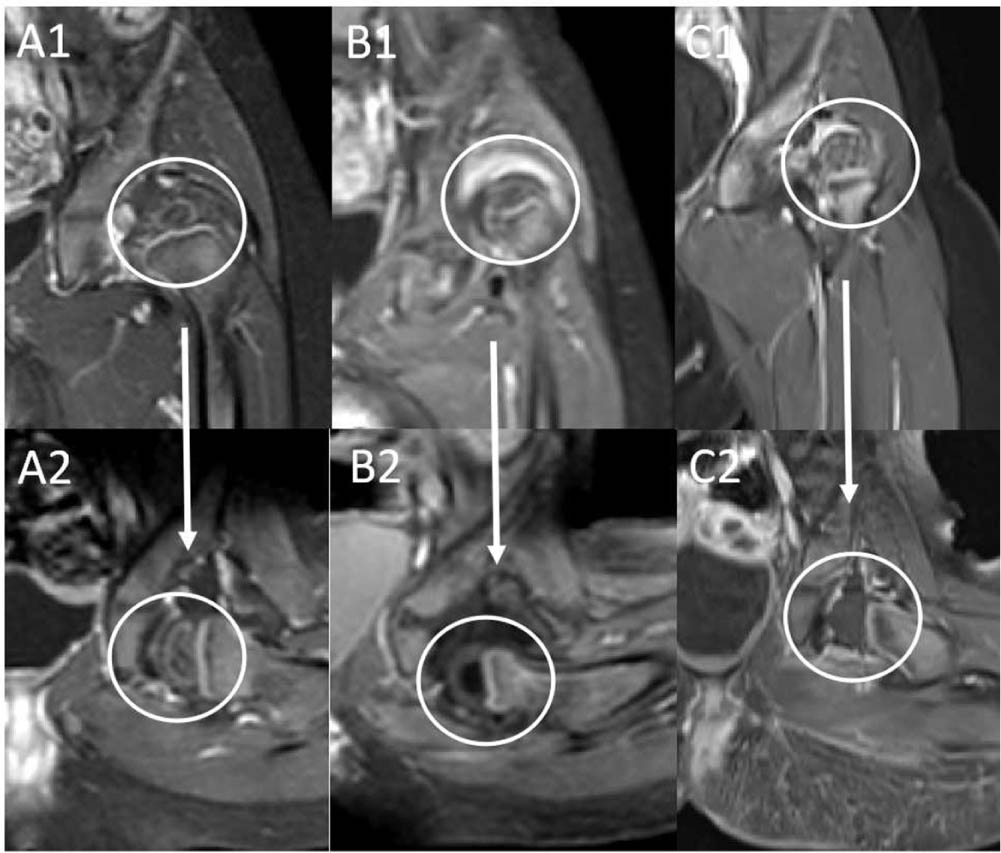
Schematic diagram of the perfusion changes of the femoral head before and after closed reduction. A1 and A2 global unchanged or enhanced by perfusion changes. B1 and B2 partial decrease of perfusion. C1 and C2 global decrease of perfusion.
Statistical analysis
Statistical analysis was performed with SPSS software (version 20.0; SPSS, Chicago, Illinois). The chi-squares test, analysis of variance and t-test were used to analyze the vascular development of femoral head such as number of vessels, type and perfusion changes between age, Tönnis grade, AI, adductor release, abduction angle and AVN. The tests were two-sided, and a p-value of < 0.05 was found to be significant.
Results
Radiographic and pMRI showed good to excellent inter-observer reliability for AI (intra-class correlation coefficient (ICC) = 0.911), perfusion changes of the femoral head (ICC = 0.856), vascular type of the femoral head (ICC = 0.913) and number of vessels of the femoral head (ICC = 0.902).
Among the included 83 hips, 59 hips (71.1%) were Tönnis grade II, 11 (13.3%) grade III and 13 (15.7%) were grade IV.
Mean AI before CR was 39.5° (sd 4.3°; 29.1° to 48.6°). At the final follow-up, mean AI was 30.5° (sd 5.2°; 21.5° to 41.9°).
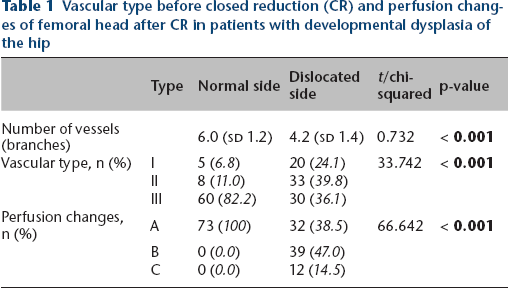
The number of vessels in the femoral head of the dislocated side was significantly less than that of the contralateral side (p < 0.001). The vascular type I and II pattern of the femoral head at the dislocated side before CR was significantly more than that at contralateral side, and type III was significantly less than that at contralateral side (p < 0.001) (Table 1). Perfusion changes of type A at dislocated side after CR was significantly less than that at contralateral side, but the ratio of perfusion changes of type B and C was significantly higher than that at contralateral side (p < 0.001) (Table 1).
Vascular type before closed reduction (CR) and perfusion changes of femoral head after CR in patients with developmental dysplasia of the hip
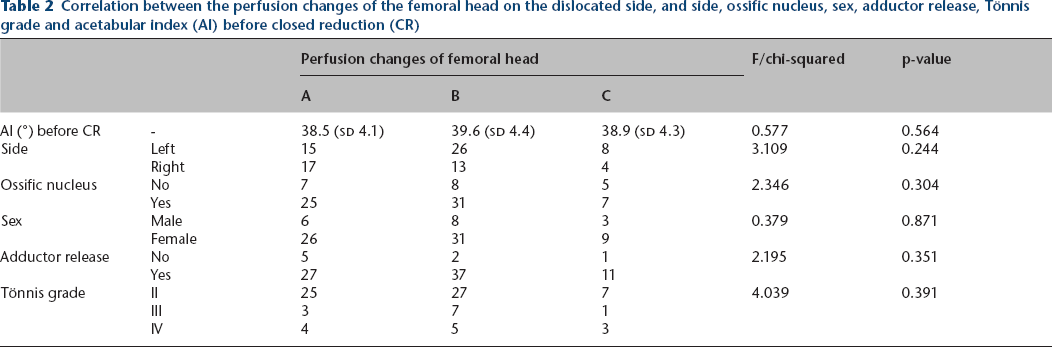
AI, ossific nucleus, sex, side, age, adductor release, abduction angle and Tönnis grade have nothing to do with perfusion changes on the dislocated side after CR, while vascular type was positively associated with perfusion changes after CR (Table 2).
Correlation between the perfusion changes of the femoral head on the dislocated side, and side, ossific nucleus, sex, adductor release, Tönnis grade and acetabular index (AI) before closed reduction (CR)
In total, 32 out of 83 hips (38.5%) developed AVN, including 22 type I AVN (68.8%), seven type II AVN (21.9%), two type III AVN (6.2%) and one type IV AVN (3.1%). The incidence of AVN above type II was 12.0%.
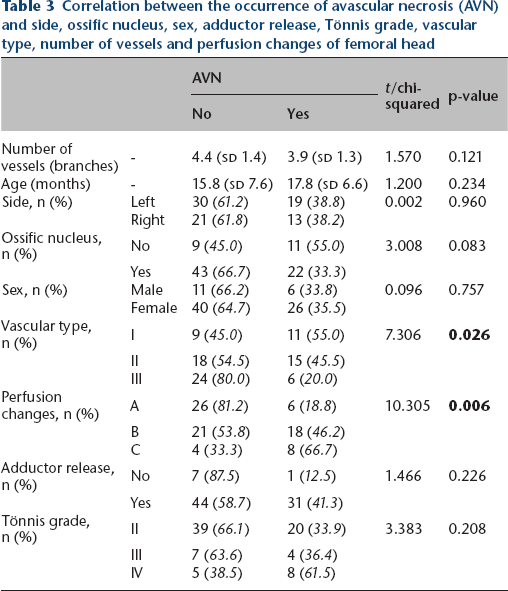
There was no significant difference in the number of vessels of the femoral head between patients with AVN and those without AVN (p = 0.121). The incidence of AVN in patients with vascular type I of femoral head (55.0%) before CR was significantly higher than that with type III (20.0%) (p = 0.026) (Fig. 3). The rate of AVN in patients with perfusion type A of femoral head (18.8%) was significantly lower than that with perfusion type C (66.7%) (p = 0.006) (Fig. 4). There was no significant difference in sex, age, side, abduction angle, number of vessels, adductor release, ossific nucleus and Tönnis grade between patients with and without AVN (Table 3).

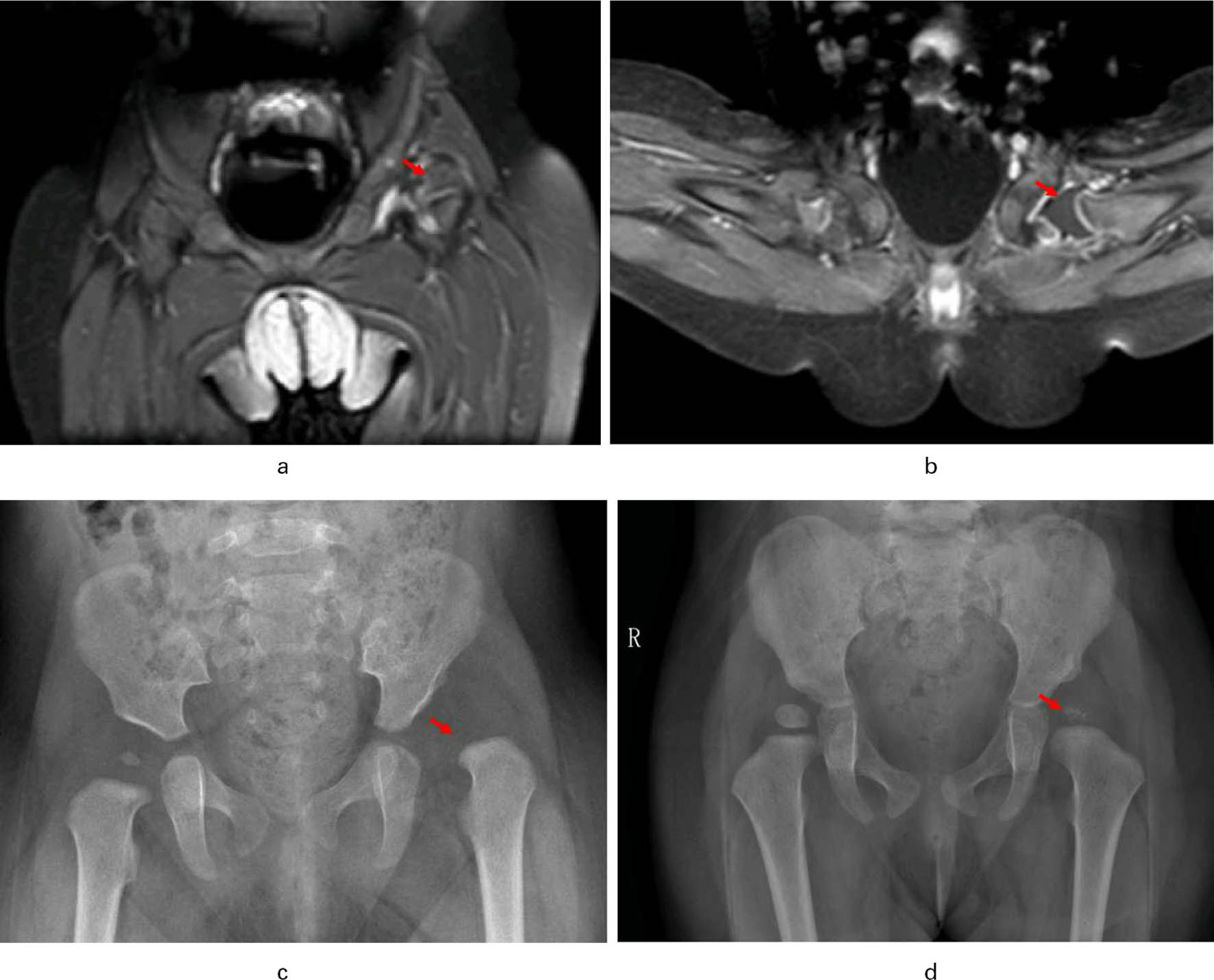
Example of vascular type I in children with left side developmental dysplasia of the hip for one year after closed reduction had developed avascular necrosis.
Example of perfusion type C in children with left side developmental dysplasia of the hip for one year after closed reduction had developed avascular necrosis.
Correlation between the occurrence of avascular necrosis (AVN) and side, ossific nucleus, sex, adductor release, Tönnis grade, vascular type, number of vessels and perfusion changes of femoral head
Discussion
This study showed that the vascular pattern of the femoral head on the dislocated side in patients with DDH was worse than that at the contralateral side. Previous studies have shown that the blood supply of the femoral head is essential to its normal growth and ossification, and the distribution and the number of blood vessels in the femoral head also continuously changes with the growth and development of the femoral head.19–21 Barnewolt et al 18 reported that the normal blood vessel of the femoral head in infants and young children on pMRI mainly showed three distribution types corresponding to epiphyseal development type I, type II and type III. The higher the vascular type, the more mature the development of the blood vessel.
In our study, Barnewolt et al's method was used to classify the vascular type of femoral head. The results suggested that the ratio of type III (mature type) of femoral head vessels on the dislocated side of DDH (36.1%) were significantly less than that on the contralateral side (82.2%). At the same time, the number of vessels on the dislocated side were also significantly worse than that on the contralateral side. In addition, 61.5% of the femoral head on the dislocated side showed a partial or global decrease after CR, but there was no perfusion decrease at contralateral side. It can be seen that the vascular development on the dislocated femoral head in patients with DDH is worse than on the contralateral side. Our previous study has also shown that the development of the femoral head on the dislocated side in patients with DDH is significantly poorer than that at the contralateral side. 22 This may be related to the lack of mutual stress stimulation between the dislocated femoral head and acetabulum, the poor development of the femoral head and the poor development of the vascular.
Our studies have also showed that the incidence of poor perfusion of the femoral head on the dislocated side was significantly higher than that at contralateral side. 22 In all, 61.5% of vascular perfusion of the femoral head was partially or globally decreased on the dislocated side in patients with DDH after CR, but not decreased at the contralateral side. Tiderius et al 15 reported that pMRI was used to evaluate the perfusion changes of the femoral head after CR in 27 children (28 hips) with DDH, and the results showed that 20 hips (71.4%) showed focal, asymmetric and global decreased of perfusion of the femoral head after CR on the dislocated side. Gornitzky et al 14 also reported similar results. In this group of cases, the authors classified both focal and asymmetric decrease as partial decreased and compared with the contralateral side. The results showed that the incidence of perfusion decrease of the femoral head on the dislocated side was significantly higher than that at the contralateral side.
This study also found that poor vascular development of the femoral head before CR would increase the risk of AVN in patients with DDH. Vascular development of the femoral head included the development of vascular quantity and vascular quality. In this group, there was no significant difference in the number of vessels of the femoral head between patients with AVN and patients without AVN after CR, but there was significant difference in the vascular type. Type I (immature type) was the dominant vascular type in patients with AVN, while type III (mature type) was the dominant vascular type in patients without AVN. Our previous studies have also shown that poor development of the femoral head is a risk factor of AVN in patients with DDH after CR.22,23 Thus, vascular immaturity of the femoral head before CR is an intrinsic factor in the occurence of AVN after CR. This may also explain why the occurrence of AVN after DDH surgery is difficult to avoid completely regardless of the therapeutic measures taken.
This study indicated that poor perfusion of the femoral head in patients with DDH after CR would increase the risk of AVN. In this group of cases, the incidence of AVN was 66.7% and 46.2%, respectively, in patients with global and partial perfusion decrease of the femoral head, which was significantly higher than in patients with unchanged or enhanced perfusion of the femoral head (18.8%), and the poorer the perfusion, the higher the risk of AVN. The results of our study are similar to previous reports. Tiderius et al 15 used pMRI to evaluate the perfusion changes of femoral head in 27 children (28 hips) with DDH after CR, and the results showed that AVN appeared in 30% of patients with perfusion decreased of the femoral head, and in 60% of patients with global perfusion decreased of the femoral head, while AVN did not occur in those with no significant perfusion decreased of the femoral head. In addition, the studies of Gornitzky et al 14 and Jaramillo et al 12 also showed that the perfusion decrease of the femoral head in patients with DDH after CR would significantly increase the risk of AVN. Poor perfusion of the femoral head often indicates poor blood supply of the femoral head.24,25 Previous studies have confirmed that blood disorder of the femoral head was an important factor of the occurrence of AVN.12,24,25
It should be noted that there are still some limitations in the present study: 1) this is a retrospective study; 2) the follow-up time (12.0 to 34.4 months) is relatively short. However, follow-up time is enough to make sure if AVN has occurred or not, as reported by previously published studies; 3) the samples were small, therefore, further studies with larger number of patients are needed to evaluate the effects of vascular development of the femoral head assessed by pMRI on the incidence of AVN.
Conclusion
The vascular development and perfusion changes of the femoral head on the dislocated side are significantly worse than those at the contralateral side. Immature vascularity of the femoral head before CR and poor perfusion of the femoral head after CR may be risk factors for AVN in patients with DDH.
Footnotes
YZ: Study design, Performed measurements, Manuscript preparation.
LJ: Study design, Statistical analysis, Manuscript preparation.
ZM: Performed measurements, Manuscript preparation.
FC: Performed measurements, Manuscript preparation.
LY: Study design, Statistical analysis.
LY: Performed measurements.
XH: Study design, Manuscript modification.