
Abstract
Abstract
Purpose
This study aimed to compare the efficacy of decreasing leg-length discrepancy (LLD) and postoperative complications between tension band plates (TBP) and percutaneous transphyseal screws (PETS).
Methods
This retrospective study reviewed LLD patients who underwent temporary epiphysiodesis at the distal femur and/or proximal tibia from 2010 to 2017 (minimum two years follow-up). Efficacy of decreasing LLD was assessed one and two years postoperatively. Complications were classified with the modified Clavien-Dindo-Sink complication classification system. Knee deformities were assessed by percentile and zone of mechanical axis across the tibial plateau.
Results
In total, 53 patients (25 boys, 28 girls) underwent temporary epiphysiodesis (mean age, 11.4 years). The efficacy of decreasing LLD at two years between the TBP (n = 38) and PETS (n = 15) groups was comparable. Seven grade III complications were recorded in six TBP patients and in one PETS patient who underwent revision surgeries for knee deformities and physis impingement. Four grade I and two grade II complications occurred in the TBP group. The mechanical axis of the leg shifted laterally in the PETS group and medially in the TBP groups (+7.1 percentile versus -4.2 percentile; p < 0.05). Shifting of the mechanical axis by two zones was noted medially in four TBP patients and laterally in two PETS patients.
Conclusion
More implant-related complications and revision surgeries for angular deformities were associated with TBP. A tendency of varus and valgus deformity after epiphysiodesis using TBP and PETS was observed, respectively. Patients and families should be informed of the risks and regular postoperative follow-up is recommended.
Level of evidence
Level III
Keywords
Introduction
Epiphysiodesis, either permanent or temporary, is a common treatment for leg-length discrepancy (LLD). Patients with LLD > 2 cm neither tolerate well nor are successfully treated with conservative methods. The indication for epiphysiodesis is predicted LLD at maturity of 2 cm to 5 cm with enough growth remaining to correct the discrepancy.1–3 Permanent epiphysiodesis refers to the ablation of the epiphyseal plate to stop bone growth. Phemister 4 first described physeal osteotomy in 1933 to arrest the growth. A satisfactory result depends on the accurate estimation of the timing of permanent epiphysiodesis because the procedure is irreversible.5–7 Temporary epiphysiodesis suppresses bone growth through implants but preserves the physis. The growth suppression can be adjusted by removing the implants once the treatment goal has been achieved. Several implants have been developed to suppress bone growth temporarily, including the use of staples, tension band plates (TBP), and percutaneous transphyseal screws (PETS).8–10 The aforementioned implants and techniques were widely accepted in treating LLD and were advocated for their reversible and mini-invasive advantages.
The efficacy between different implants after epiphysiodesis in LLD varied. Lee et al 11 found that TBP had significantly lower efficacy than staples. Lykissas et al 12 compared three different implants and reported that the postoperative outcomes of TBP, staples and PETS were comparable. However, there was a decreased annual rate of correction with PETS compared with using staples, but not with the TBP. Moreover, clinical research comparing the efficacy of TBP and PETS remained inconclusive.
Complications following temporary epiphysiodesis are not uncommon. Surgical wound complications included hemarthrosis, knee effusion, persistent knee pain and wound infection. 10 Implant-related complications such as loosening, malposition and broken screws have been reported. 13 Physis-related complications included permanent damage, rebounding after implant removal and angular deformity. 12 After temporary epiphysiodesis, the angular deformity was reported to occur in as many as 50% of cases after epiphysiodesis using staples and 20% using screws.14,15
With the increasing use of TBP and PETS in epiphysiodesis, this study aims to answer two clinical questions. Firstly, do TBP and PETS have similar efficacy of decreasing LLD? Secondly, which implant is associated with greater risks of surgical complications? Thus, this study aimed to compare the efficacy of decreasing LLD and postoperative complications between TBP and PETS.
Materials and methods
This retrospective comparative study included patients with LLD of 2 cm to 5 cm with adequate growth remaining, who underwent temporary epiphysiodesis using TBP or PETS at the distal femur or proximal tibia in the Chang Gung Memorial Hosptial, Taoyuan, Taiwan. Patients who had concurrent osteotomy/epiphysiodesis at the ipsilateral proximal femur and had incomplete radiographic data were excluded.
Patient's demographic data, including sex, age, underlying diseases and other clinical conditions, were collected. Leg lengths were measured from the top of the femoral head to the midpoint of the distal tibia on the split scanogram of the lower extremities using the built-in software of the electronic picture archiving and communications system. The lengths of the femur and tibia were also measured separately. The efficacy of epiphysiodesis was evaluated based on the LLD improvement at one and two years postoperatively.
Temporary epiphysiodesis was performed at the distal femur, proximal tibia or combined. The selection of implants for epiphysiodesis was dependent on the surgeon's preferences. In the PETS group, guide pins were inserted into the distal femur and/or proximal tibia after small incisions under the fluoroscope. The optimal guide wire position aimed to cross the physis at the junction of the middle third of the physis with its medial and lateral thirds on the coronal plane and within the middle third of the physis on the sagittal plane. After drilling, two 7.0mm stainless steel cannulated screws, partially threaded, were inserted, followed by the guide pin, and stopped just short of the articular surface (Fig. 1). In the TBP group, the eight plates were placed at the medial and lateral sides of a physis without opening the periosteum. The guide pin was first inserted, followed by drilling the cortex. Two screws were then fixed at a divergent position (Fig. 2). Anteroposterior and lateral views were checked using fluoroscopy C-arm image intensifier for proper implant position either in the PETS or TBP group.
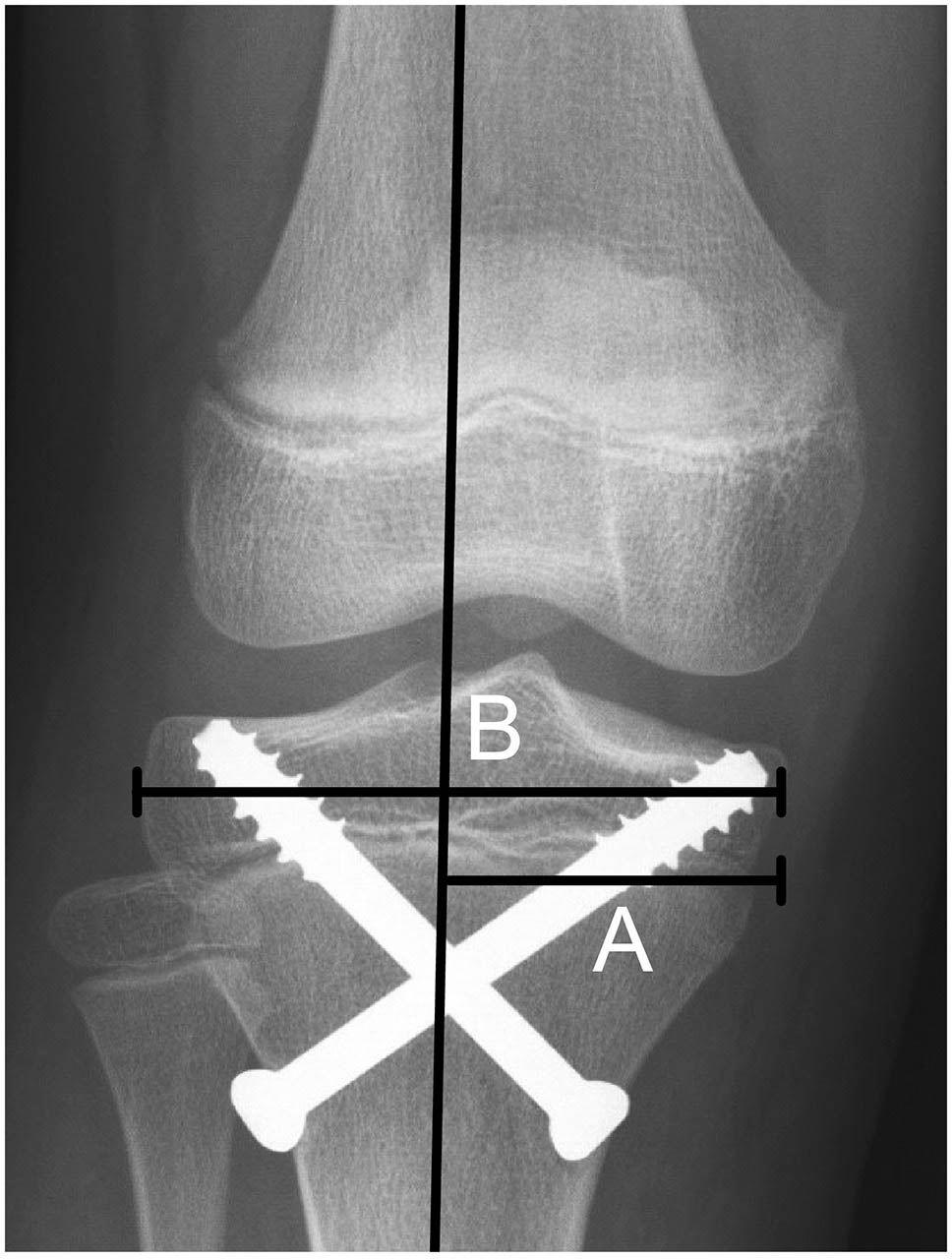
Measuring the percentile of the mechanical axis across the tibial plateau in a patient who underwent epiphysiodesis using transphyseal screws (A/B). The distance from the medial edge of the tibial plateau to the mechanical axis is marked ‘A’ and the width of the tibial plateau is marked ‘B’.
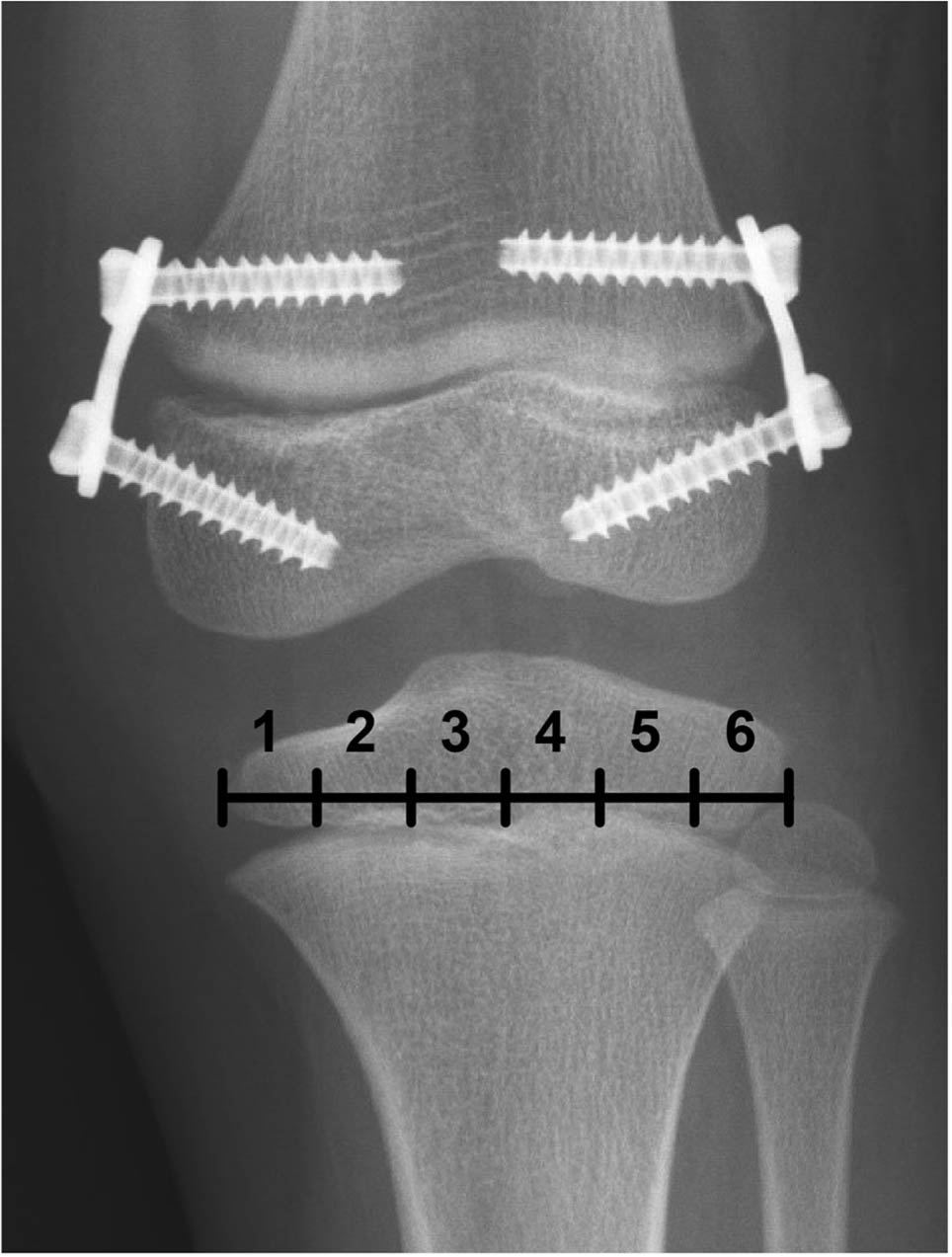
Six zones of the tibial plateau in a patient who underwent epiphysiodesis using tension band plates.
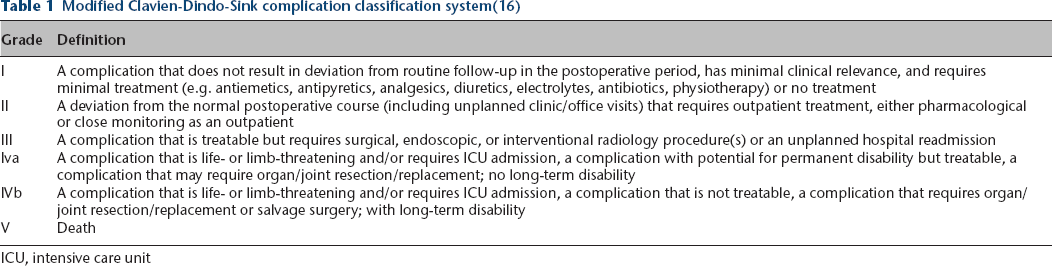
Surgical complications of temporary epiphysiodesis were graded according to the modified Clavien-Dindo-Sink complication classification system. 16 This system consists of five grades according to the severity of postoperative complications (Table 1). Knee deformities were assessed according to the position of the mechanical axis, which was defined as the line connecting the centre of the femoral head and the centre of the talus. Deviation of the mechanical axis on the tibial plateau was measured by the ratio of the distance from the medial tibial edge to the mechanical axis divided by the width of the tibial plateau (Fig. 1). The ratio was recorded as a percentile, and the 50th percentile indicated that the mechanical axis crossed the midpoint of the tibial plateau. The change in the percentile between the preoperative and two-year postoperative values was assessed. Medial shifting of the mechanical axis (varus change) was recorded as a negative value, and lateral shifting of the mechanical axis (valgus change) was recorded as a positive value. Deviation of the mechanical axis was assessed by the change in the zone of the knee joint. The tibial plateau was divided into six average zones, with zones 1 to 6 spanning the medial to the lateral directions (Fig. 2). The zone of the mechanical axis crossing the plateau was assessed preoperatively and two years postoperatively. In the patients receiving combined temporary epiphysiodesis, lateral distal femur angle (LDFA) and medial proximal tibia angle (MPTA) were measured to evaluate the bone that was more likely to cause the anatomical change related to the axial deviation. A single orthopaedic senior resident obtained all measurements using the electronic picture archiving and communications system.
Modified Clavien-Dindo-Sink complication classification system(16)
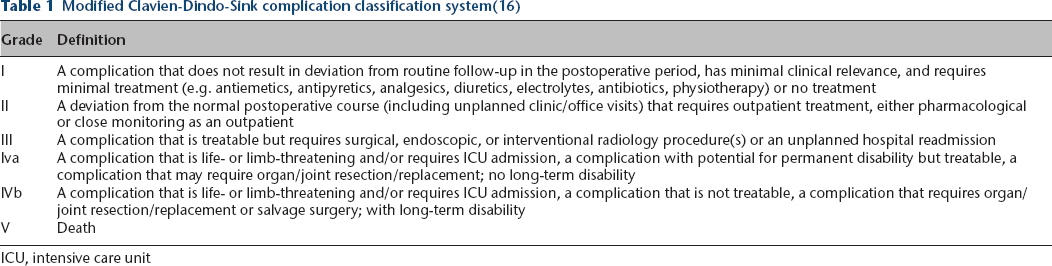
ICU, intensive care unit
Statistical analysis
The efficacy of the epiphysiodesis was evaluated by LLD (cm) and the improvement of the discrepancy from the preoperative condition to two years postoperatively. Intragroup and intergroup comparisons were performed using analysis of variance (ANOVA) and independent t-test, respectively. Mechanical axis deviation was evaluated by the mean change in the percentile between preoperative and two-year postoperative values, and a comparison between plates and PETS was performed using an independent t-test. A p-value < 0.05 indicated statistical significance.
Results
Between 1st January 2010 and 31st December 2017, 60 patients with LLD were treated by temporary epiphysiodesis using TBP or PETS. Seven patients were excluded due to concurrent epiphysiodesis at the ipsilateral proximal femur, incomplete radiography and mixed implants. In total, 53 patients were enrolled in this study. The aetiologies of LLD in the 53 patients (25 boys and 28 girls) included cerebral palsy (n = 11), lipomyelomeningocele (n = 1), developmental dysplasia of the hip (n = 6), tumour (n = 4, rhabdomyosarcoma, Ollier disease, fibrous dysplasia and osteochondroma), congenital hemi-hypertrophy (n = 4), hemimelia (n = 3), congenital pseudo-arthrosis (n = 1), Legg-Calve-Perthes disease (n = 3), arthrogryposis (n = 1), septic hip (n = 3), clubfoot (n = 2) and fracture (n = 4). The other ten patients were diagnosed with idiopathic LLD. Aetiologies in the different groups are shown in Table 2. The mean age at surgery was 11.4 years (6 to 14). The mean duration of follow-up was 25.2 months (24 to 31).
The aetiologies for leg-length discrepancies between groups
TBP, tension band plates; PETS, percutaneous transphyseal screws
Comparison of the efficacy between TBP and PETS
IN all, 38 patients underwent epiphysiodesis using TBP (tibia, 11 patients; femur, 13 patients; both, 14 patients) and the other 15 patients underwent epiphysiodesis using PETS (tibia, five patients; femur, four patients; both, six patients). The patients in the TBP group were younger than those in the PETS group. The mean preoperative LLDs were 20.8 mm and 21.7 mm in the TBP and PETS groups, respectively. At two years postoperatively, TBP and PETS caused a significant decrease in LLD (p < 0.05 in both groups, repeated-measure ANOVA). Improvements of LLD in the lower limb, femur, and tibia were comparable between the two groups (Table 3).
Efficacy of tension band plates and percutaneous transphyseal screws in improving leg-length discrepancy (LLD)
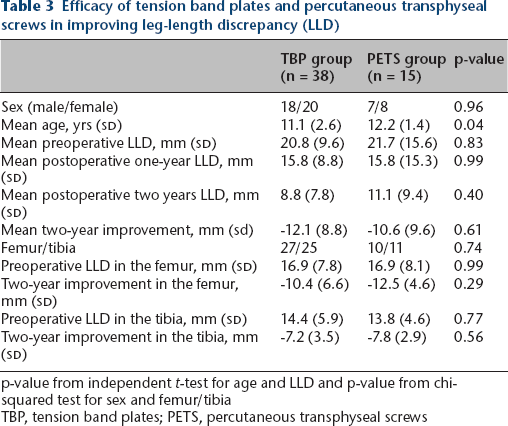
p-value from independent t-test for age and LLD and p-value from chi-squared test for sex and femur/tibia TBP, tension band plates; PETS, percutaneous transphyseal screws
Complications related to epiphysiodesis
Using the modified Clavien-Dindo-Sink complication classification system 16 , 14 patients were recorded as having postoperative complications (Table 4 and Table 5). Four patients experienced a grade I complication (occasional medial knee pain or soreness after sports activities due to irritation of the pes anserinus). Two patients had swelling and local heat around the knee after TBP at the distal femur. These complaints were relieved by anti-inflammatory drugs and were classified as grade II complications. All six patients with grade I and II complications were treated using TBP, and the implants were located at the distal femur (n = 4) and proximal tibia (n = 2). No wound infection, neurapraxia or joint contracture was recorded in either group.
Complications classified according to the modified Clavien-Dindo-Sink classification system(16)
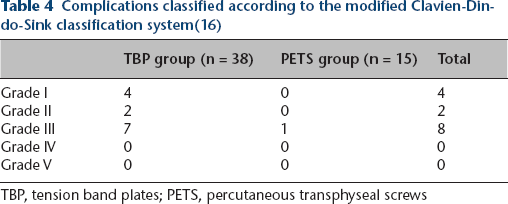
TBP, tension band plates; PETS, percutaneous transphyseal screws
List of 14 patients with postoperative complications
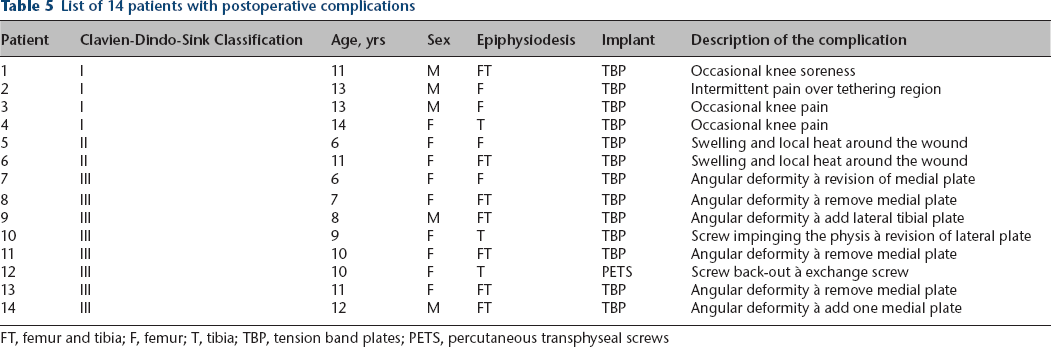
FT, femur and tibia; F, femur; T, tibia; TBP, tension band plates; PETS, percutaneous transphyseal screws
Eight patients developed grade III complications because revision surgeries were performed for angular deformities. They had epiphysiodesis at a mean age of 9.1 years (5.8 to 12.0) and had revision surgeries at 16.1 months (7 to 23) postoperatively. Seven patients were in the TBP group, six of whom had angular deformity in which the mechanical axis progressively shifted outside the central one-third of the tibial plateau (Fig. 3). The other TBP patient underwent revision for a screw impinging the physis following gradual displacement of the plate to the metaphysis. Surgical procedures included removal of one side plate in four patients, augmentation by adding one more plate in one patient and change of plate location in two patients. One patient in the PETS group underwent revision surgery for screw back-out from the medial epiphysis and angular deformity. The surgical procedure was screw exchange.
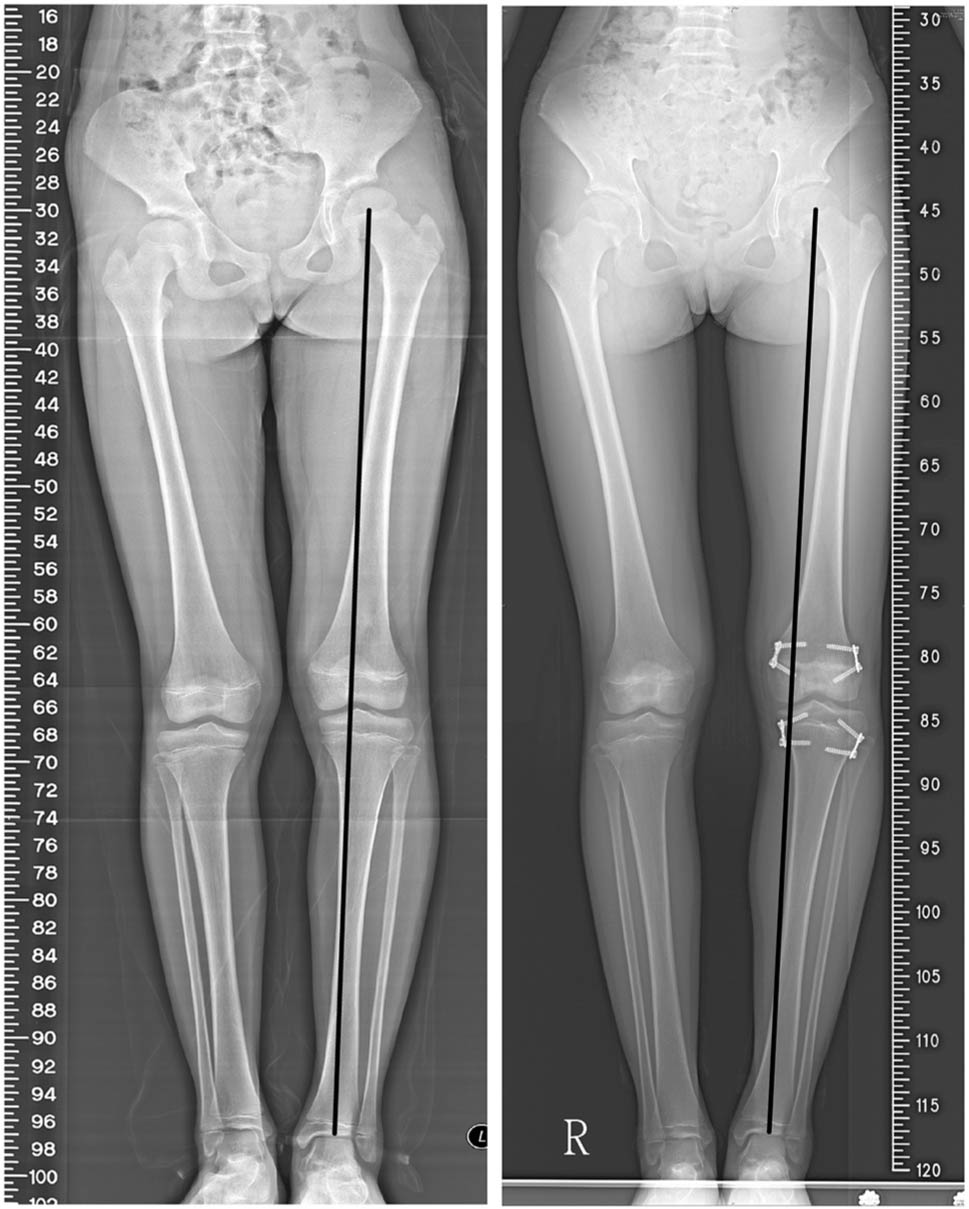
A 9.9-year-old girl with idiopathic leg-length discrepancy (LLD) underwent left distal femur and proximal tibia temporary epiphysiodesis using tension band plates. Less LLD and genu varum was observed 20 months later. Revision surgery of removing medial femoral plate was performed (case 13 in Table 6)
Angular deformity of the knee
At two years postoperatively or before revision surgeries, shifting of the mechanical axis by one zone or more was noted in 18 patients in the TBP group, and four patients had shifting by two zones, which were all medial shifts. The numbers of shift of at least one zone occurring in the femur, tibia or combined epiphysiodesis were four, six and eight, respectively. After analyzing the LDFA and MPTA of combined epiphysiodesis, five cases were generated from the femur and three cases from the tibia. Conclusively, 11 cases were femur-related and seven cases were tibia-related in the TBP group. In the PETS group, shifting of the mechanical axis by one zone or more was noted in 12 patients, and two patients had shifting by two zones, both of which were lateral shifting. With the same analysis, five cases were femur-related and seven cases were tibia-related for one zone or more in the shift of the mechanical axis. When shifting by two zones was regarded as a clinically significant change, varus change in the TBP group and valgus change in the PETS group were observed (Table 6). For all 53 patients who underwent temporary epiphysiodesis, the mean deviation of the mechanical axis was -4.2% (SD 14.9) in the TBP group and +7.1% (SD 13.1) in the PETS group (independent t-test, p = 0.04). A tendency for varus and valgus changes of the knee was found in the TBP and PETS groups, respectively.
Patients with shifting of the mechanical axis by one zone or more after epiphysiodesis
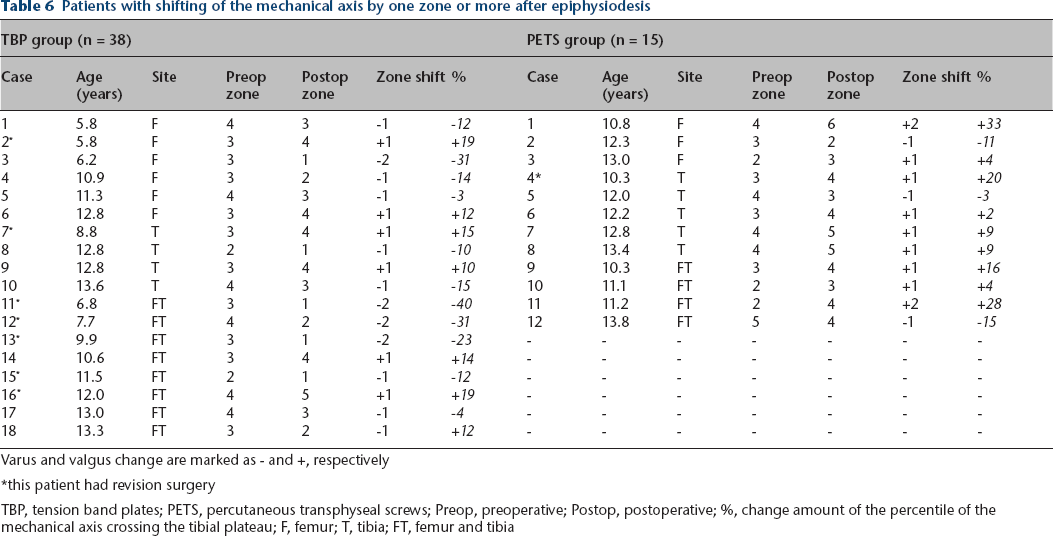
Varus and valgus change are marked as − and +, respectively
this patient had revision surgery
TBP, tension band plates; PETS, percutaneous transphyseal screws; Preop, preoperative; Postop, postoperative; %, change amount of the percentile of the mechanical axis crossing the tibial plateau; F, femur; T, tibia; FT, femur and tibia
Discussion
This retrospective study reviewed the efficacy and complications of two common implants for temporary epiphysiodesis. The similar two-year efficacy between TBP and PETS was also comparable with that of a previous study. 12 However, a greater complication rate in 38 patients using TBP, including seven revision surgeries and six minor complications, was the main issue in the study. Moreover, there was a tendency of varus and valgus change following temporary epiphysiodesis using TBP and PETS, respectively.
Varus deformity after TBP epiphysiodesis
Varus deformity had been reported in epiphysiodesis using staples. Brockway et al 17 evaluated the efficacy after stapling in 42 patients and reported discouraging results. Four patients had genu varum, all of whom had the epiphysiodesis over the proximal tibia (three had both distal femoral and proximal tibial stapling). Gorman et al 15 analyzed 54 patients who underwent epiphysiodesis with staples and reported that 27 had large shifting of the mechanical axis (> 1 cm) and 89% developed varus deformity. Significantly larger shifts were also found over the proximal tibial and combined epiphysiodeses. Our study also revealed similar tendency of varus deformity after plating.
The cause of varus deformity after epiphysiodesis using staples or plates remains unclear. Technical problems with inadequate position of the implants may play a role. Brockway et al 17 reported that greater flaring of the tibia lateral tuberosity may cause inefficacious stapling over the lateral side. Blount 18 emphasized that the staple should be perpendicular to the growth plate and the prongs should be parallel to the physis when performing epiphysiodesis. Gorman et al 15 also noted that the proximal-lateral aspect of the tibia was the most likely location for inadequate placement of staples. Continued growth of the fibula was considered one of the possible reasons for varus deformity. 15 Staples and plates share a similar structure, that is, they use two anchors in the epiphysis and metaphysis with fixed distance to suppress cellular activity in the epiphyseal plate. 19
Valgus deformity after PETS epiphysiodesis
Mechanical axis deviation after epiphysiodesis using PETS has been reported as a complication.(9,11,19,20) Ilharreborde et al 14 concluded that the use of the PETS technique in the tibia was associated with valgus deformity in 20% of the patients. Most of the deformities were attributed to the difficulty of crossing the screws in a small surface area of the proximal tibia. Another cause is screw back-out from the epiphysis following growth. Nouth and Kuo 13 stated that the purchase of the thread on the epiphysis is critical for growth retardation. Song et al 20 suggest that PETS should be a fully threaded stainless steel screw with sufficient thread depth and large screw head. However, axial deviations were still encountered in 8.5% of the 59 patients. Dodwell et al 21 reported high efficacy and low complication rate of PETS, with four (4.9%) of 81 cases developing angulation change ≥ 5°.
Greater risks of complication after TBP epiphysiodesis
A main issue of this study is that TBP had greater risks of complications than PETS did. Although the wound in TBP was small, it was larger than the stab wound for PETS. TBP at the distal femur were placed within the knee joint, whereas PETS were placed through the metaphysis without implants irritating the synovium. The above difference may result in more grade I and II complications in the TBP group. TBP were applied on the medial and lateral edges of the physis, and PETS inhibited bone growth at the medial and lateral thirds of the physis. The distance between two TBP was longer than that between two PETS. When the inhibition capacity is not equal between medial and lateral implants, such as malposition or loosening of implant, TBP produce greater imbalanced inhibition at the physis. The difference of fixation configuration between TBP and PETS is one of the reasons why deformity was more common in the TBP group.
Surgical tips from this study
The risk of knee deformities may be useful information in preoperative planning. Previous studies as well as the present study presented varus deformity after plating or stapling and valgus deformity after screwing. If the mechanical axis crosses zone 1 or 2, i.e. genu varum before epiphysiodesis, PETS may be the implant of choice for epiphysiodesis. If the mechanical axis crosses zone 5 or 6, i.e. genu valgum before epiphysiodesis, TBP may be the implant of choice. The surgical techniques for TBP and PETS should be executed exactly under the fluoroscope. When using TBP for epiphysiodesis, the plates should be parallel to the sagittal axis of the bone. PETS should be parallel to the sagittal axis and enter the epiphysis with sufficient thread depth. 20 Moreover, before epiphysiodesis, the patient and their families should be well informed of risks of angular deformity. Postoperatively, a split scanogram is recommended every six months to detect any angular deformities.
Limitations
This study has some limitations. Firstly, this study has the inherent limitations of a retrospective design. Age and heterogeneous aetiology of LLD may introduce some bias in comparing the efficacy and complications. Secondly, some patients who had shifting of the mechanical axis by two zones did not undergo surgery, such as case 1 in the TBP group and cases 3 and 12 in the PETS group. Thirdly, further analysis of the association between angular deformities and contributing factors such as age, location of epiphysiodesis, partial or full threaded screws and suboptimal placement of implants was limited by the small sample size. Fourthly, deformity on the sagittal plane was not considered in this study. Anterior placement of the epiphysiodesis implants is associated with extension deformity. 22 Genu recurvatum and standing in a in-toeing/out-toeing posture may affect the measurement of the mechanical axis. Lastly, the follow-up of two years is relatively short, and there was no data for the resumption of growth. There might be more complications noted with longer follow-up.
Conclusion
This study confirmed that TBP and PETS provided similar efficacy in decreasing LLD. However, more wound-related complications and revision surgery for angular deformities were associated with TBP. Thus, the patients and their families should be informed about the risks preoperatively and regularly followed postoperatively. New implants or methods for balanced suppression of bone growth are required.
Footnotes
Acknowledgements
The collection and analysis of medical records and radiographs was provided by the Institutional Review Board of the authors’ hospital.
H-KK: Conceptualized and designed the study.
Y-HC: Executed radiographic measurements, Drafted the initial manuscript. Y-FT: Carried out the initial analyses, Revised the manuscript.
W-EY: Carried out the initial analyses, Revised the manuscript.
C-HC: Reviewed and revised the manuscript.