
Abstract
Purpose:
Hemi-epiphysiodesis procedures in skeletally immature patients are commonly done to correct genu valgum over time. This study seeks to demonstrate the average rate of deformity correction for genu valgum using hinged tension band plates, while examining different age groups and sex-related differences.
Methods:
A retrospective chart review of patients who underwent hemi-epiphysiodesis with hinged tension band plates for valgus knee deformity from 2012 to 2022 by one pediatric orthopaedic surgeon was performed. Expected time of growth remaining was calculated as the difference between age of skeletal maturity and bone age at time of surgery. The mechanical lateral distal femoral angle, mechanical medial proximal tibial angle, mechanical femoral tibia angle, screw divergence angle, and hinge angle were measured immediately after implant placement and prior to implant removal.
Results:
54 skeletally immature patients were treated for pathologic genu valgum. The mean age at time of surgery was 12.5 ± 1.9 years. The radiographic measurement of the valgus deformity between the beginning and end of treatment showed significant correction (p = 0.002). The lower limb axis of the younger cohort corrected significantly faster (7.5 ± 4.6°/year) than the older cohort (5.3 ± 2.8°/year) (p = 0.030). The mechanical lateral distal femoral angle correction rate was also significantly different between the two cohorts (7.0 ± 4.7°/year vs. 4.8 ± 2.8°/year, respectively (p = 0.002)). The group with greater expected time of growth remaining demonstrated a significantly faster rate of correction than the group with less than 2 years of growth remaining (p < 0.001).
Conclusion:
This study reaffirms the finding that timing is essential when performing temporary hemi-epiphysiodesis for valgus knee deformity in skeletally immature patients.
Introduction
Lower extremity growth is not linear. Children younger than 7 years old have normal physiologic genu varum that progresses to genu valgum before returning to a normal mechanical hip and knee axis.1,2 Pathologic genu valgum refers to the condition of persistent or worsening genu valgum in a patient older than 7 years of age. Genu valgum may result from endocrine, metabolic, or developmental pathologies, or it may be idiopathic. 2 There are many types of surgical treatments, however, a widely accepted technique is guided growth correction.
Guided growth correction uses various minimally invasive devices such as staples, figure eight plates, and screws to correct angular deformity in the distal femur or proximal tibia. Temporary hemi-epiphysiodesis has been shown to be associated with lower morbidity and fewer complications than an osteotomy.3,4 However, the biggest challenge of this technique is implanting these devices at the optimal time to avoid over- or under-correction. It is important to consider each individual case to determine when they will begin to have a growth spurt and when their physes will close as this will have a crucial impact on the timing of surgical intervention. Further over- or under-correction could lead to additional follow-up surgical interventions.5,6
This study aims to illustrate the rate of change of the lower limb angle in children treated with hinged tension band plates. In addition, this study hopes to provide insight into the optimal timing of implantation of hinged tension band plates in children with various years of growth remaining. We hypothesize that patients who have implant-mediated guided growth at a younger age will correct faster than patients who undergo implant-mediated guided growth at an older age.
Materials and methods
After Institutional Review Board approval, all skeletally immature patients with knee valgus deformity treated with hemi-epiphysiodesis using a hinged tension plate (Hinge-plates, Pega Medical, Inc., Laval, Quebec, Canada) from 2012 to 2022 by one pediatric orthopaedic surgeon were performed and were identified using implant item number. Patients who had subsequent clinical and radiological follow-up and underwent implant removal surgery after lower limb axis correction were included in the analysis. Patients who received previous surgical treatment for lower limb axial correction were excluded. No exclusion was made based on each patients’ etiology of genu valgum.
The patients’ diagnosis, chronological and bone age at the time of hemi-epiphysiodesis, and surgery dates of both plate insertion and removal procedures were recorded. The time interval between implant placement and implant removal was consequently calculated. Radiographic measurements performed on lower hip-to-ankle radiographs included the mechanical femoral tibia angle (mFTA), the mechanical lateral distal femoral angle (mLDFA), and medial proximal tibial angle (MPTA) (Figure 1). The screw divergent angle (SDA) and hinge angle (HA) were also measured. Every measurement was performed on the immediate post-operative radiograph following plate insertion procedure and on the last pre-operative radiograph before hardware removal surgery. The angle variation between the pre- and post-operative measurements was then divided by the duration of treatment to obtain the correction rate. To avoid bias, we considered MPTA measurements and changes only in the knees with hinged tension band plates on the proximal tibia.
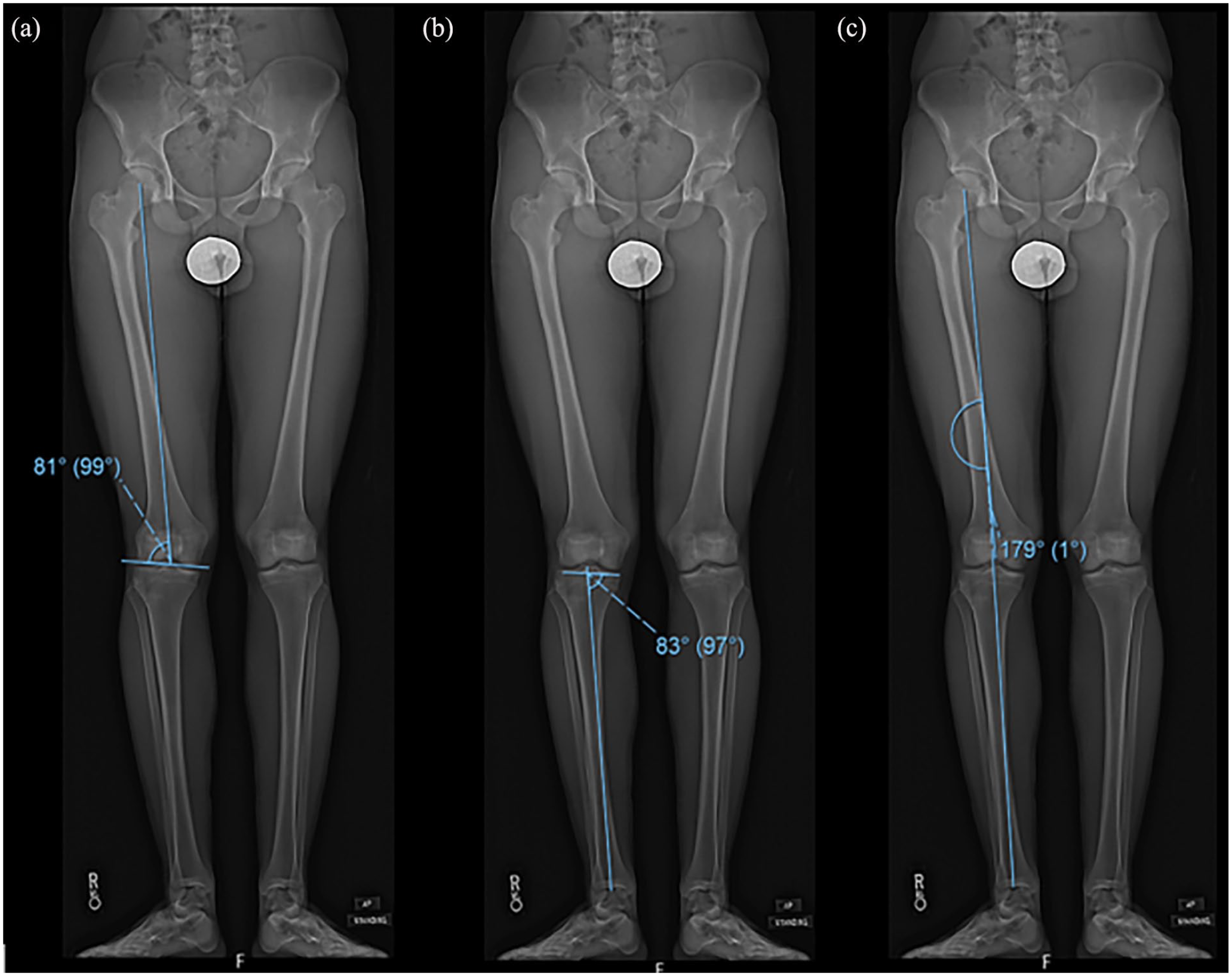
Lower hip-to-ankle radiograph measurements (a) medial lateral distal femoral angle (mLDFA), (b) medial proximal tibial angle (MPTA), and (c) mechanical femoral tibia angle (mFTA).
For analysis purposes, the patients were divided into two cohorts based on chronological age: cohort 1 included females ≤ 12 years old and males ≤ 14 years old, cohort 2 included the older patients (females > 12 and males > 14 years). The change in degrees over time of mFTA and mLDFA was compared between the two groups.
Next, the change in angles over time was compared between different groups of patients based on the years of expected time of growth remaining (ETGR). The patients were split into two cohorts, a younger group of males and females with 2 or more years of ETGR, and an older group of skeletally immature patients with less than 2 years. The ETGR was calculated using bone age whenever available (78.2%) or chronological age in the remaining cases (21.8%). The Greulich and Pyle method was used to assess bone age, and expected growth maturity was set at 14 years for girls and 16 years for boys, as reported in the literature. 7
Finally, measures of angular velocity of mFTA were univariately correlated with the growth remaining. Data failing normal distribution assumption with Kolmogorov–Smirnov (n > 50) or Shapiro–Wilk (n < 50) tests were analyzed with a Spearman coefficient and Mann–Whitney U tests, respectively. Data in normal distributions were analyzed with Pearson coefficients and independent samples t-tests.
Data analysis was performed using IBM (Armonk, NY) SPSS Statistics version 22 for Windows.
Results
Seventy-eight patients with 158 hinged tension band plates were identified using implant item number. Five patients had implants on the lateral side of the knee for pathologic genu varum and were excluded. Nineteen patients did not have their plates removed at the time of our analysis and were excluded.
Fifty-four skeletally immature patients—28 (51.9%) males and 26 (48.2%) females—were included, for a total of 97 knees treated with 110 hinged tension band plates for pathologic genu valgum (Table 1). The mean age at time of surgery was 12.5 ± 1.9 years (range: 7.8–16.9 years). The mean duration of the treatment was 17.9 ± 7.6 months (1.5 ± 0.6 years), (range: 8.2–48.2 months). Ninety-seven plates were implanted on the distal femur and 13 on the proximal tibia, with 13 knees where the implants were positioned both on the femur and tibia. There were no cases of hemi-epiphysiodesis on the proximal tibia only. Forty-four (81.5%) patients had bilateral lower limb deformity and had implants on both left and right knees; among them, four patients (7.4%) had all four physes of the knees treated with hinged tension band plates. Ten patients had unilateral lower limb deformity, four on the right knee, and six on the left.
Demographics of the entire cohort (N = 54).
SD: standard deviation; BMI: body mass index; ETGR: expected time of growth remaining.
Lower limb angles
All 97 treated knees were studied for lower limb angles. The mLDFA showed significant correction from 84.01 ± 3.44° to 91.88 ± 3.84° at the time of plate removal (p < 0.001). The mLDFA change rate was 6.38 ± 4.44°/year. The general MPTA was 90.65 ± 2.65° pre-operative and 88.63 ± 2.61° at the time of plate removal (p = 0.001), with a change rate of 4.02 ± 3.26°/year.
The mFTA at the time of implant placement was 6.48 ± 2.99° and –1.79 ± 3.13° at the time of implant removal (a negative sign indicates a slight overcorrection to varus). This difference was statistically significant (p < 0.001). The deformity correction rate over time for mFTA was 6.78 ± 4.29°/year.
There were no statistically significant differences in the rate of mFTA correction in knees with only femoral plates versus knees with plates on both the femur and tibia (6.7 ± 4.1°/year vs. 6.9 ± 4.9°/year, p = 0.90) (Table 2).
Lower limb angles throughout treatment.
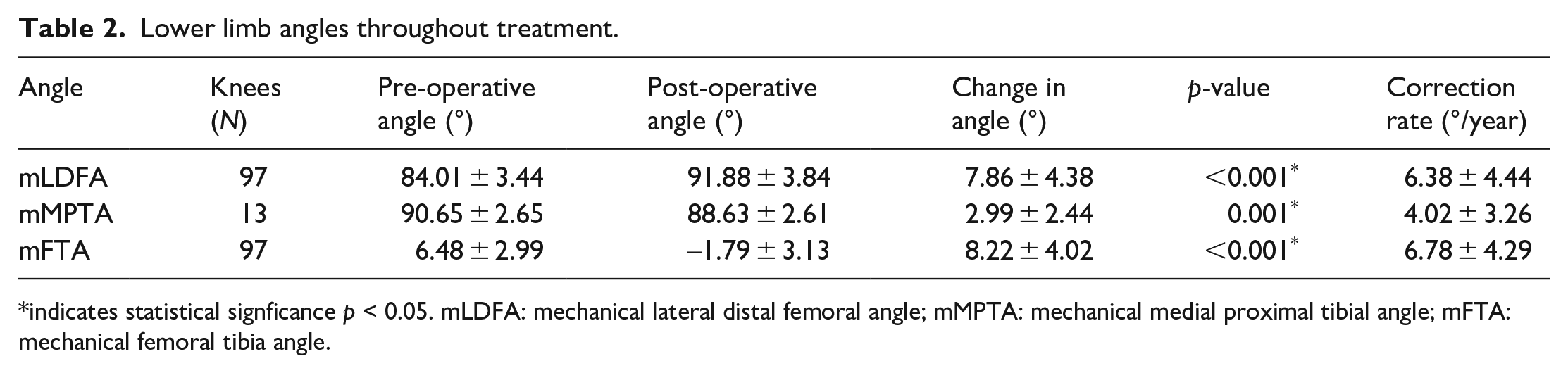
indicates statistical signficance p < 0.05. mLDFA: mechanical lateral distal femoral angle; mMPTA: mechanical medial proximal tibial angle; mFTA: mechanical femoral tibia angle.
Plate-related angles
The SDA and HA were measured and the plates implanted on the distal femur and proximal tibia were separately considered. For the 97 femoral plates, the SDA changed significantly from 11.63 ± 8.29° pre-operatively to 24.92 ± 9.72° at time of plate removal (p < 0.001). The HA also changed significantly in this group, from 23.52 ± 8.75° at the time of implant placement to 2.31 ± 5.34° at the end of the treatment (p < 0.001). For the plates on the proximal tibia, the SDA changed from 7.12 ± 6.91° to 12.47 ± 7.03° (p = 0.001), and the HA from 11.04 ± 9.08° to –0.87 ± 2.42° (p = 0.002) (Figure 2, Table 3).
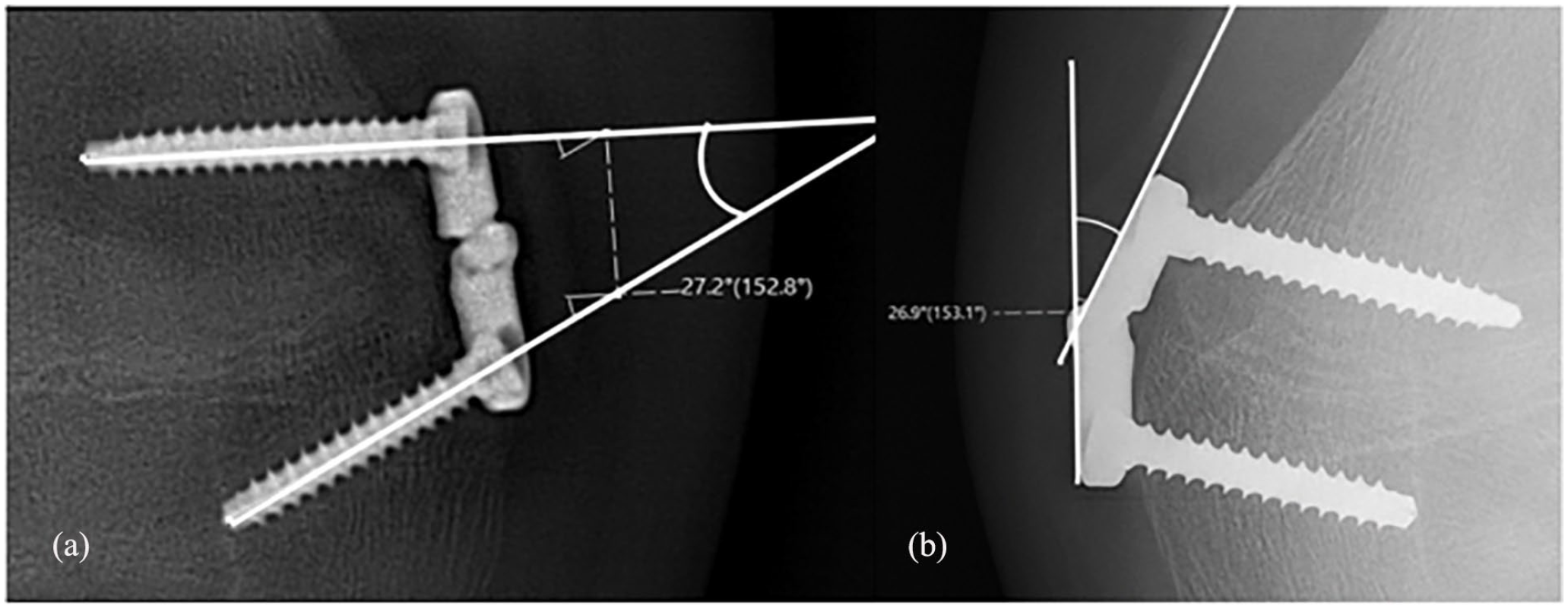
Plate-related angles (a) An example of the screw divergence angle measurement. This example shows a SDA of 27.2° (b) An example of the HA measurement. This example shows a HA of 26.9°.
Plate related angles at the beginning and end of treatment, their change, and the rate of change over time.
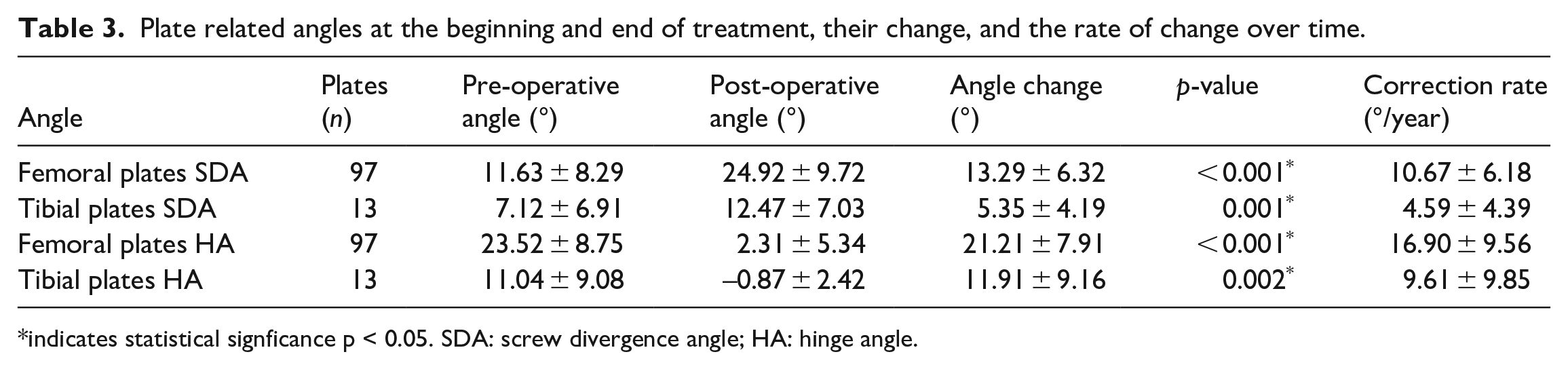
indicates statistical signficance p < 0.05. SDA: screw divergence angle; HA: hinge angle.
Age-related differences
The rate of mLDFA and mFTA correction was different comparing the two cohorts of patients based on chronological age. The younger group consisted of females younger than 12 years old and males younger than 14, for a total of 63 knees. The older group was composed of females 12 years of age and older and males 14 years of age or older, for a total of 34 knees. The mLDFA correction rate was 7.3 ± 4.9°/year for the younger group and 4.8 ± 2.8°/year for the older group (p = 0.002). The mFTA correction rate was 7.5 ± 4.6°/year and 5.3 ± 2.8°/year for the younger and the older group, respectively (p = 0.03) (Figure 3).
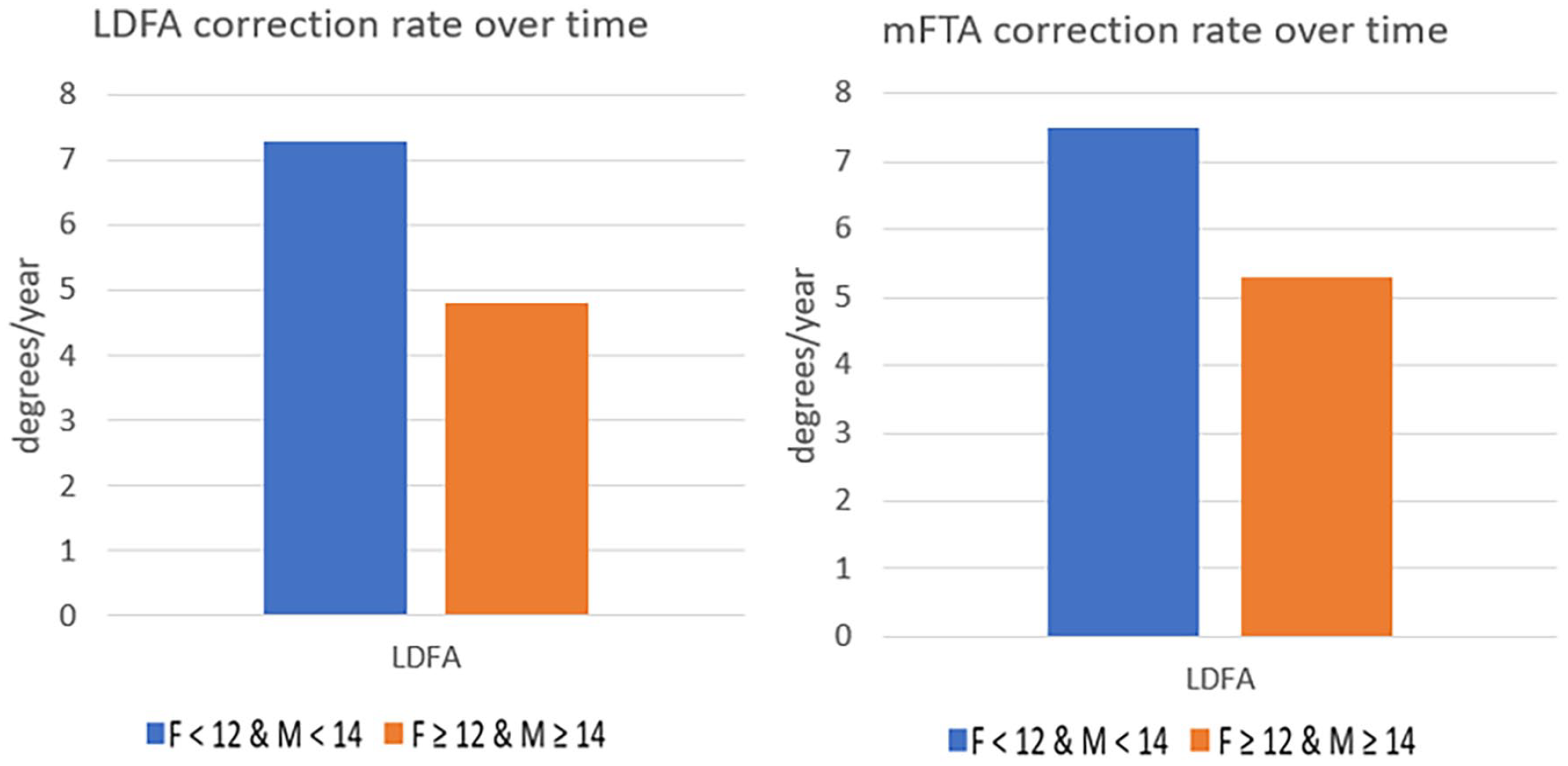
Age-related differences based on chronological age comparing the mLDFA and mFTA correction rate.
Next, the change in angles per unit time was compared between two groups based on the years of ETGR. The younger group included 80 knees with angle correction rate of 6.9 ± 4.3°/year for LDFA and 7.4 ± 4.2°/year for mFTA. The older group included 17 knees with angle correction rate of 2.9 ± 2.0°/year for LDFA and 3.4 ± 2.3°/year for mFTA. The correction rate of both angles was significantly different between the two groups (p < 0.001) (Figure 4).
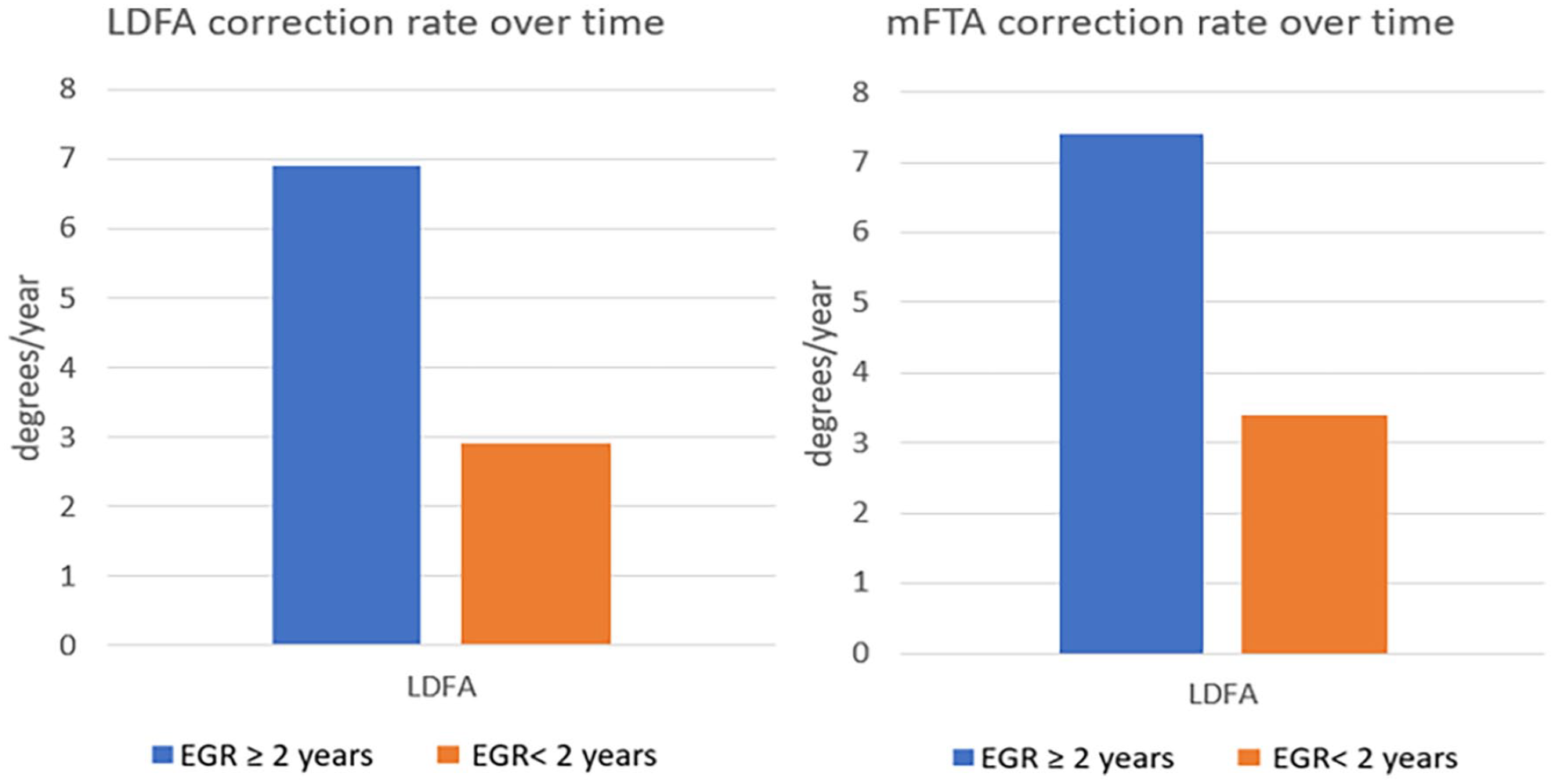
Age-related differences based on years of expected time of growth remaining (ETGR) comparing the mLDFA and mFTA correction rate.
Finally, the rate of mFTA change was univariately correlated with the years of ETGR, demonstrating a significant relationship in which each additional year of growth remaining correlated with 1.84° of mFTA correction rate change per year (Figure 5).
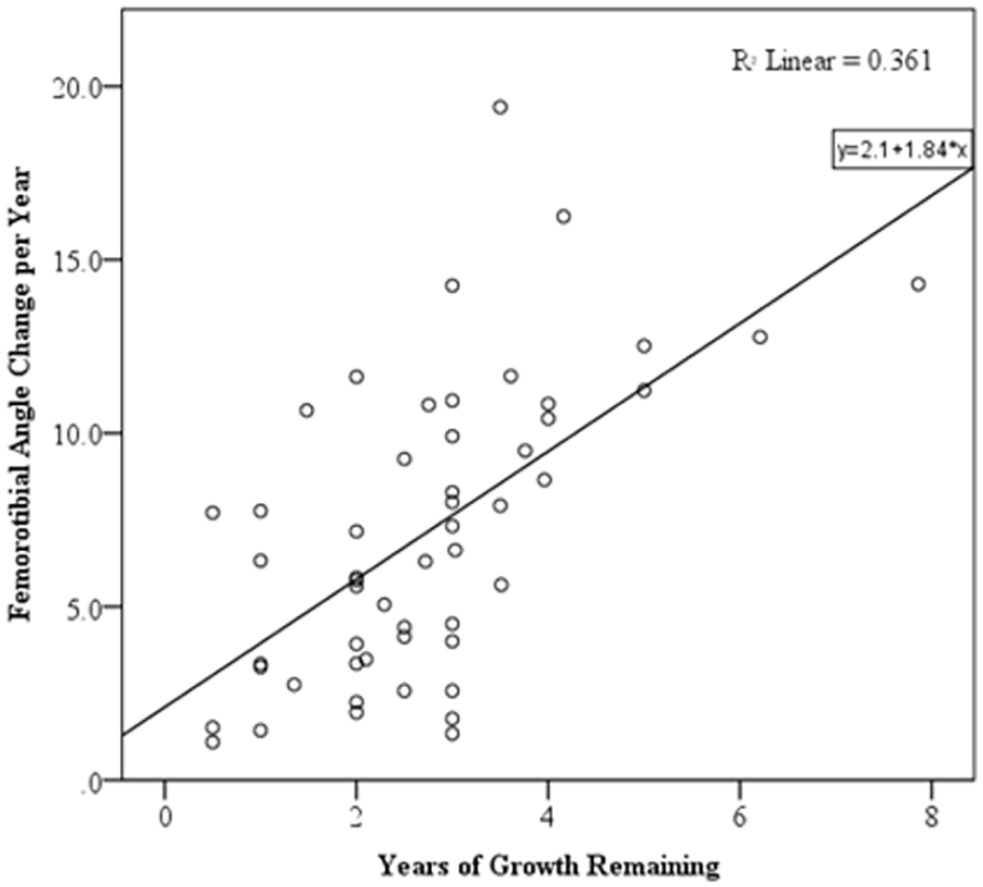
The correlation between the mFTA correction rate and the years of estimated growth remaining. Each additional year of growth remaining at the time of implantation leads to an increase of 1.84° of mFTA correction velocity per year.
Complications
No screws or plate breakages, deep infections, or premature growth arrests were observed during the study. Two (3.7%) patients experienced recurrent valgus knee deformity at follow-up and they were subsequently treated again with hinged tension plates with definitive deformity correction. Three patients had minimal residual valgus knee deformity at the time of implant removal, with mFTA values between 3.6° and 3.8°.
Discussion
Implant-mediated guided growth with plates has become a leading treatment option for lower extremity angular deformity correction in patients with open physes; however, limited data exist regarding the rate of change of the lower limb axis and the optimal time for performing this intervention. Different guided growth implants are commercially available. All the patients in our study were treated with the same implant to avoid confounders. The hinge plate is a novel design implant with the design advantage of a hinge that connects two plate halves.
Shin et al. 8 analyzed the complications of three different guided growth implants. They reported three broken cannulated screws in the peanut plate group and three screw pullout in the eight-plate group. They did not report any plate-related complications for the hinge-plate group. Plate-mediated guided growth has become increasingly popular as it reduces physis damage upon removal as the implant is placed in a periosteal position while securely fixed to the bone; the hinge plate in particular adds an additional mechanism to reduce growth stress of the physis, due to the bearing connecting the two halves of the implant. In our study, two patients had recurrent genu valgum deformity and were treated with a second hemi-epiphysiodesis. We did not have any plate-related complications in the 110 plates considered. The limited number of complications demonstrates the validity of the hinge-plate implant. The hinge plate specifically allows the implant to conform to the anatomy of the growing bone of the skeletally immature patient, as the two parts of the plate lay directly on the surface of the bone. By having a hinge plate situated over the growth plate, there may be less contact stress on the implant.
A recent study evaluated the difference between tension-band plates and percutaneous transphyseal screws hemi-epiphysiodesis; in their analysis, they found different mechanical axis deviation (MAD) correction rates comparing three different age groups. In their study group composed of 35 patients they concluded that in the tension band plate cohort the MAD correction rate progressively increases from the younger group (7–10 years old) to the oldest (14–16 years old). 9 However, they did not consider sex-related differences, which are paramount to consider in skeletal maturity and bone development.
The main purpose of this study was to illustrate the rate of change in the mFTA and mLDFA in children who underwent hemi-epiphysiodesis for pathologic genu valgum and to identify the optimal timing of implantation, considering sex-related difference due to the different age skeletal maturity in males and females. We found that the mFTA and mLDFA correct at a similar rate. When considering all the patients, the mFTA correction rate was 6.78 ± 4.29°/year (0.57°/month) and the mLDFA correction rate was 6.38 ± 4.44°/year (0.53°/month). Considering the patients with tibial hemi-epiphysiodesis, the MPTA was 4.02 ± 3.26°/year (0.34°/month). Both the mLDFA and MPTA correction rate were in line with the results of Kadhim et al., 10 who reported 0.56°/month and 0.40°/month, respectively. Interestingly, we did not find any significant difference in the velocity of mFTA correction when we compared the knees treated with only femoral plates and the knees with plates implanted on both the femur and tibia. This is in contrast with what was highlighted in Kadhim et al. 10 study, where they reported a faster deformity correction rate if both the femoral and tibial physes were treated. We attribute this difference to our indication of performing hemi-epiphysiodesis of both distal femur and proximal tibia only in patients who are approaching skeletal maturity, therefore, having a slow growth of the physis. This data further underlines the importance of timing in the variability of correction rate when using these implants.
Both mFTA and mLDFA corrections showed a large variability among our patients when related with time. This is also evident considering that the removal of the implant is performed once the knee deformity is corrected: in our study, one patient maintained the implant for 48.2 months before removal, while the shortest treatment had a duration of only 8 months.
Since the temporary hemi-epiphysiodesis blocks only one side of the physis while the other side continues to growth, it seems reasonable to expect an expedited variation of lower limb angles during the time of the growth spurts. However, to our knowledge, no study evaluated this aspect of hemi-epiphysiodesis.
To evaluate the difference in rate of angle correction, we divided the patients into a younger and an older cohort.
We performed the first analysis based on the chronological age. The current literature reports expected growth maturity at 14 years for females and 16 years for males, 7 so we consequently considered 2 years before this age as the cut-off to consider different patients. We found that males younger than 14 and females younger than 12 had a significantly faster mLDFA correction rate than older patients; more importantly, the mFTA, which better relates to the lower limb axis and the clinical valgus deformity of the knee, also corrected at a faster rate in this cohort.
We performed a second analysis of deformity correction per unit time based on the bone age, to have a more accurate relation between the bone growth and the correction rate. Bone age indicates the level of biological and structural maturity more precisely than chronological age. 11 Both mLDFA and especially mFTA corrected faster in the younger group, with an even stronger statistically significant difference (p < 0.001) than the previous analysis. Orthopaedic surgeons performing plate-mediated guided growth should be aware of these differences to correctly counsel patients and to plan adequate timing for plate positioning, subsequent follow-up, and implant removal surgery.
There were important limitations in our study. In addition to limitations due to the retrospective nature of our research, bone age was available in 78.2% of patients.
One strength of our study is the homogeneous population. All the 97 lower limbs with pathologic genu valgum had the medial distal femoral physis treated, which allowed us to evaluate plates acting on the same location of the knee. The majority of the published studies regarding temporary guided growth implants considered small cohorts without differentiating the multiple combination of hemi-epiphysiodesis—medial side for valgus deformity, lateral side for varus deformity, femur only, tibia only, cases with both the femur and the tibia treated— which we strongly believe can lead to erroneous conclusions when considering all the lower limb axial angles at the same time.
Skeletally immature patients with pathologic genu valgum treated with hinged plate-mediated hemi-epiphysiodesis have an expedited correction when they have 2 or more years of ETGR compared to older patients. Further studies are necessary to evaluate different age-related groups to further define the best timing for hinged plate-mediated guided growth treatment.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521241229976 – Supplemental material for Temporary hemi-epiphysiodesis with tension band plates in skeletally immature patients with genu valgum: Faster correction in patients with more than 2 years of expected time of growth remaining
Supplemental material, sj-pdf-1-cho-10.1177_18632521241229976 for Temporary hemi-epiphysiodesis with tension band plates in skeletally immature patients with genu valgum: Faster correction in patients with more than 2 years of expected time of growth remaining by Damiano Salvato, Danielle E. Chipman, Peter Cirrincione, Joseph Hawes, Emilie Lijesen and Daniel W. Green in Journal of Children’s Orthopaedics
Footnotes
Author contributions
D.S., D.E.C., P.C., J.H., and D.W.G. developed the methodology of this protocol. D.S., D.E.C., P.C., J.H., and D.W.G. drafted the manuscript. D.S., D.E.C., P.C., J.H., E.L., and D.W.G. edited and approved the final draft of the manuscript.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: D.S., D.E.C., P.C., J.H., and E.L. have no conflicts of interest to disclose. D.W.G. is a consultant for Arthrex, Inc. and receives royalties for Arthrex, Inc. and Pega Medical. D.W.G. is a consultant for Arthrex, Inc. and receives royalties for Arthrex, Inc. and Orthopediatrics.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study was reviewed and approved by the Hospital for Special Surgery Institutional Review Board.
Informed consent
Not required for this study, as it was retrospective.
Supplemental material
Supplemental material for this article is available online
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.