
Abstract
Abstract
Purpose
We modified the method for tibial epiphysiodesis by solely using a lateral approach to the physis. From this small-incision approach, the lateral as well as the medial part of the tibial physis were ablated. The aim of our study was to see if this operative technique might be as effective as a bilateral approach, and reduce the operation time and usage time of the image intensifier. The epiphysiodeses were monitored by radiostereometric analysis (RSA), which is a well-established method for the analysis of micro movements and has been used to monitor percutaneous epiphysiodesis with the bilateral approach. There are no reports in the literature comparing single- with double-portal approaches for percutaneous epiphysiodesis evaluated by RSA.
Methods
Twenty children were treated by percutaneous epiphysiodesis for leg length discrepancies ranging from 15 to 70 mm, comprising 14 boys and 6 girls with a mean age of 13 (11–15) years. The timing of epiphysiodesis was determined by using Moseley's straight-line graph and Paley's multiplier method. For the tibial epiphysiodesis, ten patients were operated with a single surgical approach from the lateral side (Group I) and ten patients were operated with a surgical approach from both the medial and the lateral sides (Group II). The percutaneous epiphysiodesis was monitored by RSA, a method which allows analysis of the three-dimensional dynamics of the epiphysis relative to the metaphysics. RSA examinations were performed postoperatively and after 6 weeks, 12 weeks, and 6 months.
Results
From 0 to 6 weeks after epiphysiodesis, the mean longitudinal growth across the operated physis in the tibia in Group I was 0.26 (0.01–0.6) mm. In Group II, the mean growth for the first 6 weeks after surgery was 0.17 (0.01–0.5) mm. During the time period from 6 weeks to 12 weeks after surgery, there was a mean growth of 0.06 (0.00–0.18) mm in Group I and 0.03 (0.00–0.2) mm in Group II. The mean growth from 0 to 6 weeks after epiphysiodesis for all patients was 0.22 mm, which corresponds to 30 % of the normal growth rate. From 6 to 12 weeks, the mean growth for all patients was 0.046 mm, i.e., 6 % of the normal growth rate. From 12 weeks to 24 weeks, no significant growth across the operated physis was observed in neither Group I nor Group II. The mean surgical time was 26 (21–30) min in Group I and 43 (35–48) min in Group II. This difference was statistically significant (p = 0.006). The mean time for use of the image intensifier during surgery was 202 (191–236) s in Group I and 229 (185–289) s in Group II (p = 0.013).
Conclusions
In our study, a single-portal technique from the lateral side for percutaneous epiphysiodesis of the proximal tibia was as effective as the double-portal technique. Actual growth arrest appeared within 12 weeks after surgery. A single-portal technique for epiphysiodesis of the tibia is a safe technique, with less surgical time and less time for image intensification compared to the double-portal technique.
Keywords
Introduction
The most common surgical techniques for epiphysiodesis are the Phemister technique [1], the White technique [2], epiphyseal stapling [3], epiphysiodesis with percutaneous screws [4], and the percutaneous technique as first described by Bowen and Johnson in 1984 [5]. The open methods like the Phemister and White techniques, as well as stapling, require a surgical approach which allows adequate exposure of the physis, whereas only very small incisions are needed for the percutaneous technique. According to the original paper on the percutaneous technique by Bowen and Johnson [5], the peripheral one-third of the plate is ablated and specific surgical attention is directed towards adequate ablation over the most peripheral aspect of the physeal growth plate. The ablation is done from the medial and the lateral sides of the physis. In the original description of percutaneous epiphysiodesis, a double-portal approach was used [5]; however, a single-portal approach for percutaneous epiphysiodesis is described for the femur as well as the tibia [6, 7]. Complications reported for single-portal approach epiphysiodesis are mainly associated with the femoral site.
We modified the method for tibial epiphysiodesis by solely using a lateral approach to the physis. From this small-incision approach, the lateral as well as the medial part of the tibial physis were ablated. This modification of the operative technique might simplify the surgical approach and reduce the operation time, as well as the usage time of the image intensifier. Radiostereometric analysis (RSA) is a well-established method for the analysis of micro movements [8] and has been used to monitor percutaneous epiphysiodesis with the bilateral approach [9]. There are no reports in the literature comparing single- with double-portal approaches for percutaneous epiphysiodesis evaluated by RSA.
The purpose of our study was to see if percutaneous epiphysiodesis of the tibia with only the lateral approach is as effective as a bilateral approach in order to achieve growth arrest, and to see if the single-portal approach would reduce surgical time and fluoroscopic time.
Furthermore, little is known about the time interval between percutaneous epiphysiodesis and actual growth arrest. According to Timperlake et al. [10], a period of 4–6 months is required for the bony bridge to form across the growth plate after percutaneous epiphysiodesis. However, this assumption is made based on standard radiographs and the method for how these data are obtained is not further described. Lauge-Pedersen et al. [9] performed a RSA for monitoring percutaneous epiphysiodesis and found that growth arrest in most cases appears within 12 weeks. Therefore, another purpose of our study was to see if the results from this former study could be confirmed by our findings.
Patients and methods
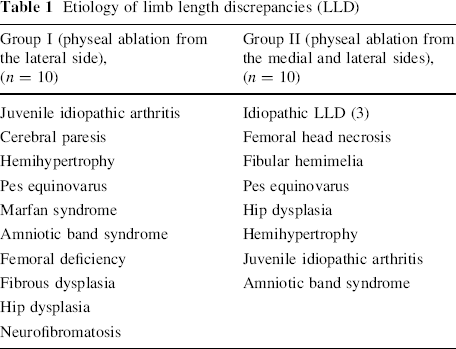
Twenty children were treated by percutaneous epiphysiodesis for leg length discrepancies (LLD) ranging from 15 to 70 mm, comprising 14 boys and 6 girls with a mean age of 13 (11–15) years. The etiologies of LLD for each group are listed in Table 1. The timing of epiphysiodesis was determined by using Moseley's straight-line graph [11] and Paley's multiplier method [12]. LLD was analyzed by orthoroentgenography with a perpendicular X-ray beam centered exactly in the joint space of each hip, knee, and ankle, respectively. Skeletal maturity was evaluated according to the atlas of Greulich and Pyle [13] by the use of left-hand X-rays. For the tibial epiphysiodesis, ten patients were operated with a single surgical approach from the lateral side (Group I) and ten patients were operated with a surgical approach from both the medial and the lateral sides (Group II). Ten consecutive patients were operated with the double-portal approach, followed by ten consecutive patients with the single-portal approach. The patients were not randomized. The surgical technique in Group I included a 1-cm skin incision laterally over the proximal tibial physis. Under image intensification, an awl was advanced 1.5 cm into the physeal plate, followed by a 6-mm drill bit. The lateral 1–1.5-cm part of the tibial physis was first ablated by fan-shaped oscillating drilling with a 6-mm drill bit and then further ablated by a 3-mm curved curette. Thereafter, the drill bit was advanced from the lateral approach to the contralateral cortex at the medial side and ablation of the medial 1–1.5 cm of the tibial physis was done in the same manner as that described for the lateral part, which included fan-shaped oscillating drilling with a 6-mm drill bit and further ablation of the physis with a 3-mm curved curette (Fig. 1). In Group II, the epiphysiodesis of the proximal tibia was performed by using a lateral incision for ablation of the lateral part and a medial incision for ablation of the medial part of the physis.
Etiology of limb length discrepancies (LLD)

After ablation of the lateral part of the tibial physis, the 6-mm drill bit was advanced to the medial part of the physis. This part of the physeal plate was ablated in the same manner as on the lateral side, with fan-shaped oscillated drilling and a curved curette
For epiphysiodesis of the proximal fibula, a 5-mm skin incision anterior-laterally over the proximal fibular physis was performed. From this incision, an awl was advanced into the physis, entering the physeal plate anteriorly in order to avoid damage of the peroneal nerve. Through this opening in the anterior cortex of the fibula, a 3-mm curved curette was used to ablate the central part of the physeal plate. Epiphysiodesis of the proximal fibula was not performed when the estimated remaining growth in the proximal tibia was ≤2 cm. Surgical tourniquet was not used in any of the patients. The surgical time and duration of image intensification for the tibial epiphysiodesis were recorded.
The percutaneous epiphysiodesis was monitored by RSA, as described by Selvik [8] and Lauge-Pedersen et al. [9]. For this purpose, six tantalum spheres of 0.8 mm in diameter were inserted on each side of the ablated physis with a hand-operated spring-loaded piston (RSA Biomedical AB, Sweden). The spheres were spread widely in a manner to allow analysis of the three-dimensional dynamics of the epiphysis relative to the metaphysis. The first RSA examinations were performed postoperatively using a specially designed calibration cage for knees (Standard Bi-Planar Cage No. 10, RSA Biomedical AB, Sweden). With the patient lying in a supine position and the knee placed in the center (Fig. 2), two X-ray films were mounted in a slide below and aside the cage. We used two ceiling-mounted X-ray tubes (Siemens, Germany) positioned at 90° to each other with simultaneous exposure, with the X-ray beam passing the cage and the leg. Further processing and final development of the X-rays was done on PACS (Picture Archiving and Communication System, Sectra, Sweden) and with an RSA analysis program (Um RSA Analysis, version 6.0, RSA Biomedical AB, Sweden). Using the RSA software, the change in distance across the physis between two subsequent examinations was calculated, as well as the change between each examination and the initial examination. The precision of our RSA measurements was evaluated based on repeated examinations performed on eight patients and calculated as described by Digas et al. [14], resulting in a precision value of 0.016 mm. Therefore, longitudinal growth >0.016 mm between two examinations was interpreted as a real (significant) change of distance (growth).

For the radiostereometric analysis (RSA), the patient's knee was placed in the center of a specially designed calibration cage. Radiographs were taken with simultaneous exposure by two X-ray tubes positioned at 90° to each other
RSA examinations were performed postoperatively and after 6 weeks, 12 weeks, and 6 months (Fig. 3). Longitudinal growth in millimeters was calculated for the first 6 weeks, from 6 to 12 weeks, and from 12 to 24 weeks after surgery. RSA measurements at 24 weeks were only performed when significant growth was still present after 12 weeks. According to Menelaus [15], the average normal longitudinal growth rate is 6 mm/year for the proximal tibia, which corresponds to a mean growth rate of 0.12 mm/week and 0.72 mm for a 6-week period.

Radiographs taken postoperatively and 6 weeks and 12 weeks after surgery. The images show the tantalum spheres which were placed on each side of the ablated physis (six spheres on each side) and those which were located in the calibration cage that is placed around the knee during X-ray acquisition.Note the increasing thinning of the growth plate and bony overgrowth
All analyses were done by the same trained radiologist (R.B.G). The mean error values and condition numbers, which give the exact value of the maximum inaccuracy, were within currently accepted limits [16]. Growth across the physis was calculated as the change in distance between the tantalum spheres in the epiphysis and those in the metaphysis.
Statistical evaluation was performed by the use of the independent t-test. The surgical time was measured from skin incision to completed closure of the wound, including the time used for the placement of the tantalum spheres. The time for fluoroscopy during surgery was read off the display on the image intensifier.
The study was approved by the Regional Ethics Committee (REK S-09377b 2009-8352).
Results
There were no peri- or post-operative complications. All patients regained full range of motion of the knee within 7–14 days. Full weight-bearing was achieved within 14 days. From 0 to 6 weeks after epiphysiodesis, the mean longitudinal growth across the operated physis in the tibia in Group I was 0.26 (0.01–0.6) mm. In Group II, the mean growth for the first 6 weeks after surgery was 0.17 (0.01–0.5) mm. During the time period from 6 to 12 weeks after surgery, there was a mean growth of 0.06 (0.00–0.18) mm in Group I and 0.03 (0.00–0.2) mm in Group II (Table 2).
Patient data
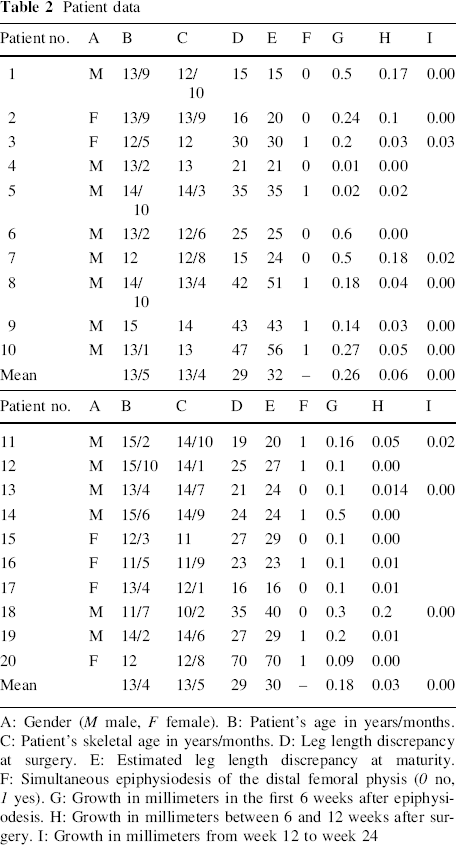
A: Gender (M male, F female). B: Patient's age in years/months. C: Patient's skeletal age in years/months. D: Leg length discrepancy at surgery. E: Estimated leg length discrepancy at maturity. F: Simultaneous epiphysiodesis of the distal femoral physis (0 no, 1 yes). G: Growth in millimeters in the first 6 weeks after epiphysiodesis. H: Growth in millimeters between 6 and 12 weeks after surgery. I: Growth in millimeters from week 12 to week 24
The mean growth from 0 to 6 weeks after epiphysiodesis for all patients was 0.22 mm, which corresponds to 30 % of the normal growth rate. From 6 to 12 weeks, the mean growth for all patients was 0.046 mm, i.e., 6 % of the normal growth rate.
The differences in growth between the two groups for the period 0–6 weeks and after 6–12 weeks following epiphysiodesis were not statistically significant (0–6 weeks: p = 0.26; 6–12 weeks: p = 0.28) based on the independent t-test.
From 12 to 24 weeks, no significant growth across the operated physis was observed neither in Group I nor in Group II.
Translation and rotation in all patients was less than 0.001 mm and 1°, respectively. No asymmetrical growth was observed.
The mean surgical time was 26 (21–30) min in Group I and 43 (35–48) min in Group II. This difference was statistically significant (p = 0.006). The mean time for use of the image intensifier during surgery was 202 (191–236) s in Group I and 229 (185–289) s in Group II (p = 0.013).
Discussion
Our study shows that a single-portal technique for percutaneous epiphysiodesis of the tibia is as effective as the double-portal technique. The surgical time and time for fluoroscopy were significantly shorter for the single-portal technique. No failures of the percutaneous epiphysiodeses were observed in either group.
Percutaneous epiphysiodesis for LLD is a well-established method. However, failure to achieve fusion of the operated physis has been described. Scott et al. [17] found three failures of the epiphysiodesis in 20 patients, and Surdam et al. [18] reported two failures in 56 patients. Both single-portal and double-portal techniques for percutaneous epiphysiodesis have been described. In the original description of percutaneous epiphysiodesis, a double-portal approach was used [5]. A single-portal approach for percutaneous epiphysiodesis is described for the femur as well as the tibia [6, 7]. Complication rates are found to be higher in the single-portal techniques, whereas the increase of complications is mainly ascribed to crossing of the midline in single-portal techniques [6]. In the femur, the middle part of the physis is quite close to the femoral notch, which makes it likely to perforate into the knee joint when ablating this part of the physis, resulting in postoperative hemarthrosis of the knee. Therefore, single-portal techniques for percutaneous epiphysiodesis of the femur might not be recommended. In the tibia, however, crossing of the midline does not compromise any anatomical structures but the physis itself. In our study, the single-portal technique of the tibial epiphysiodesis was not associated with a higher complication rate than the double-portal technique. Surgical techniques used for percutaneous epiphysiodesis might differ somewhat. Our surgical technique is comparable to the technique as described by Canale et al. [19]. Although other authors prefer large-sized drill bits up to 10 mm in diameter [7], the 6-mm drill bit used seemed to be sufficient in order to achieve physeal arrest in our study.
In our patients, the mean longitudinal growth of all patients (including both groups) across the operated physis was 30 % of normal growth according to Menelaus [15] from 0 to 6 weeks and 6 % from 6 to 12 weeks after epiphysiodesis in the tibia. Hence, during the first 6 weeks after the surgical intervention procedure, significant longitudinal growth can still be observed. However, 12 weeks after surgery, growth arrest was apparent in all patients after percutaneous epiphysiodesis (i.e., minimal and ignorable growth without clinical importance, even if >0.016 mm).
These results confirm the conclusions of Lauge-Pedersen et al. [9], who found growth arrest to appear in most cases 12 weeks after percutaneous epiphysiodesis based on RSA.
There is no standard method to monitor the effect of percutaneous epiphysiodesis. Physeal arrest might be documented by ordinary radiographs [19]. However, the interpretation of standard X-ray films according to the success of an epiphysiodesis might be difficult. In our study, RSA was an excellent method for monitoring percutaneous epiphysiodesis when comparing two different surgical techniques.
We did not perform epiphysiodesis of the proximal fibula, when the estimated remaining growth in the proximal tibia was ≤2 cm. Symptoms which could be attributed to overgrowth of the fibula were not found.
A weakness of our study is the rather low number of patients included in our investigation. However, considering that patients are exposed to radiation more often when performing RSA compared to normal follow-up after epiphysiodesis, we kept the number of patients as low as possible.
Conclusion
In our study, a single-portal technique for percutaneous epiphysiodesis of the proximal tibia was as effective as a double-portal technique. Actual growth arrest appeared within 12 weeks after surgery. A single-portal technique for epiphysiodesis of the tibia is a safe technique, with less surgical time and less time for image intensification compared to the double-portal technique. Additionally, this study might further contribute to a better understanding of the effects of percutaneous epiphysiodesis. The knowledge of the actual time interval from surgery to growth arrest has an importance for the timing of the epiphysiodesis in order to achieve a maximum of accuracy and to check the efficacy of the surgical intervention by the anticipation of no more growth after 3 months postoperatively.
Footnotes
None.