
Abstract
Purpose
To determine age-and gender-dependent variation of epiphyseal tilt and epiphyseal angle using CT in adolescents without hip pathology.
Methods
Pelvic CT scans were obtained in 132 adolescents for evaluation of abdominal pain. Radially oriented planes around the femoral neck were reformatted and the epiphyseal tilt and angle were measured in the anterior, anterosuperior and superior planes. Variations in the tilt angle and epiphyseal angle were assessed by age group from 12 to 18 years and gender by using a linear mixed model analysis.
Results
The epiphyseal tilt did not change (p = 0.97) with increasing age. Male patients exhibited smaller tilt angle in the anterosuperior plane (p = 0.003) but no difference was detected in the anterior (p = 0.17) or superior (p = 0.06) planes. The epiphyseal angle decreased with increasing age in the anterior (p = 0.03), anterosuperior (p = 0.001) and superior (p < 0.001) planes in male patients, with no variation in female patients (p = 0.92). Male patients had larger epiphyseal angles in the anterior (p = 0.02), anterosuperior (p < 0.001) and superior (p = 0.002) planes compared with female patients.
Conclusion
We found no age-specific variations in the epiphyseal tilt and no difference in the epiphyseal tilt in male and female patients in the superior and anterior plane. The epiphyseal angle was smaller in female patients, however, the epiphyseal angle decreased with increasing age in male patients which corresponds to an increase in epiphyseal extension. The reference values reported in this study may serve as additional information in the evaluation of adolescents with hip pain and as reference for future studies investigating slipped capital femoral epiphysis and femoroacetabular impingement development.
Level of Evidence
Level III Diagnostic Study
Keywords
Introduction
Slipped capital femoral epiphysis (SCFE) and cam-type femoroacetabular impingement (FAI) deformity may result from pathologic changes in the capital femoral epiphysis development. However, the aetiology of both SCFE and FAI remain poorly understood. The shape and inclination of the epiphysis have been reported to be associated with SCFE.1–4 Structural variations of the epiphysis during growth have been associated with cam-type deformity formation.5–7
Given that SCFE and the formation of the cam-type FAI deformity occur during adolescence, it is crucial to understand the relationship of the capital femoral epiphysis with the femoral neck during normal development and skeletal maturation. Several studies have reported normative references for radiographic parameters assessing the femoral head and neck morphology in asymptomatic adolescents including the alpha angle, the head and neck offset and the epiphyseal extension.5–12 However, few studies11,13,14 reported conflicting results about the epiphyseal tilt changes during normal development and normative data for epiphyseal angle is lacking. Further, there is no available data as to whether gender-specific changes influence epiphyseal tilt and epiphyseal angle during skeletal maturation in adolescence. Establishing normal parameters for epiphyseal tilt is important because increased posterior tilt of the epiphysis has been associated with a higher risk of contralateral SCFE in patients with unilateral presentation.1,15 Further, the epiphyseal angle measures epiphyseal extension which has been described as a precursor of cam-type morphology 7 and a protective factor against SCFE development. 16
In this study, we sought to determine reference values for epiphyseal tilt and epiphyseal angle in asymptomatic adolescents in different planes across the head and neck junction using radially reformatted CT imaging. We further investigated age- and gender-specific changes of the epiphyseal tilt and epiphyseal angle during skeletal maturation.
Materials and methods
After institutional review board approval, a search of our institution radiology database was performed to identify patients aged 12 to 19 years who underwent a pelvic CT scan for evaluation of abdominal pain and suspected appendicitis between 01 January 2008 and 31 October 2010. The study population included a total of 132 subjects with a mean age of 15 years (sd 1.98). There were 87 (66%) female and 45 (34%) male patients. Body mass index (BMI) information was available from 129 subjects. The median BMI percentile was 78 (interquartile range (IQR) 68 to 87). A total of 12 (9%) of the subjects were considered obese (≥ 95th percentile) and 29 subjects (22%) were considered overweight (85th to less than 95th percentile). A retrospective chart review was performed to confirm that subjects included had no previous history of hip pain or surgery. The subjects included herein were previously studied in a prior publication reporting reference values for alpha angle, epiphyseal extension and femoral head neck offset in adolescents. 8
The CT images were obtained with the subjects lying supine with both hips in extension and the pelvis in a neutral position. Radially oriented planes around the femoral neck were reformatted by a paediatric musculoskeletal radiologist (SDB) using Voxar software (Voxar Inc, Edinburgh, United Kingdom). The superior plane was defined as a coronal plane aligned perpendicular to the femoral neck through the centre of the femoral head and neck. Radial images were obtained by rotating the coronal oblique plane anteriorly in 45° increments. Three planes were defined for measurement for each hip: anterior, anterosuperior and superior. The anterior plane corresponds to the axial plane oriented through the axis of the femoral head (Fig. 1) Measurements from both hips were recorded. Reformatted images were saved as Digital Imaging and Communications in Medicine (DICOM) images and sent to a picture archiving and communication system workstation for measurement by a research assistant (KPK) specifically trained in the measurement technique who did not participate in patient selection or image reformatting. All measurements were performed using JiveX DICOM Viewer software (Visus Technology, Bochum, Germany).
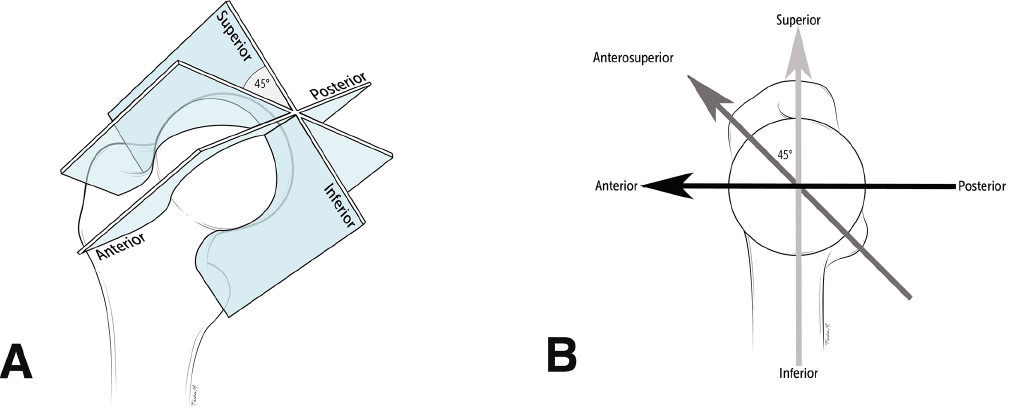
Diagrams showing the creation of the radially reformatted planes around the femoral neck axis used for measurement of the epiphyseal tilt and epiphyseal angle: (
For assessment of epiphyseal tilt, the femoral neck axis was established from the centre of the femoral head to the centre of the femoral neck and a best-fit circle was formed around the femoral head. A tangent line to the deepest portion of the femoral head in the acetabulum and perpendicular to the femoral neck axis was drawn. Then, a second line connecting the anterior and posterior aspect of the femoral physis was drawn. The angle between these lines is the epiphyseal tilt (Fig. 2). A positive value was assigned for an anteriorly tilted epiphysis while negative values corresponded to posteriorly tilt of the epiphysis in relation to the femoral neck. For assessment of the epiphyseal angle, the line through the femoral neck axis and a line from the centre of the femoral head to the anterior aspect of the physis were used. The epiphyseal angle assesses the epiphysis extension into the femoral neck. A higher epiphyseal angle implies less epiphyseal extension (Fig. 3). The epiphyseal angle differs from measurement of the alpha angle previously described by Nötzli. 17 While the alpha angle assesses the contour of the femoral head-neck junction, the epiphyseal angle measures the degree of epiphyseal extension into the metaphysis.
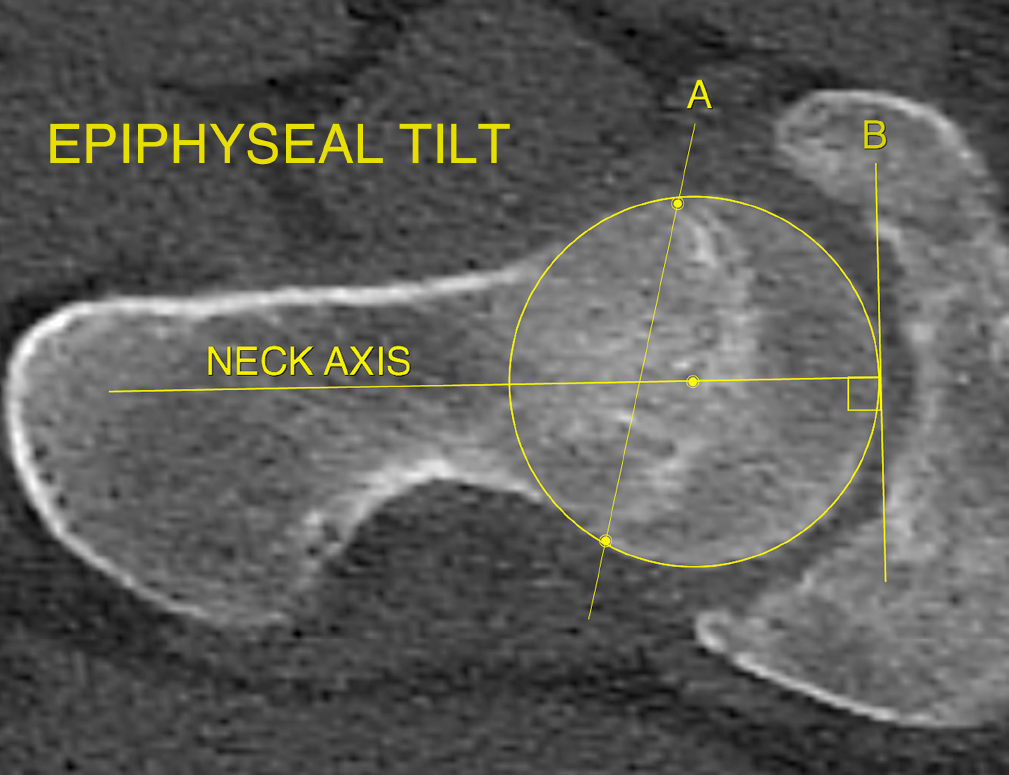
Epiphyseal tilt: the femoral neck axis and the femoral head circumference are drawn. A tangent line B is drawn through orthogonal to the femoral neck axis. A line A is drawn by the anterior and posterior aspects of the physis and the angle formed by it and line B is the tilt angle. By convention, an anteriorly tilted epiphysis gives a positive value while a posteriorly tilted epiphysis gives a negative value.
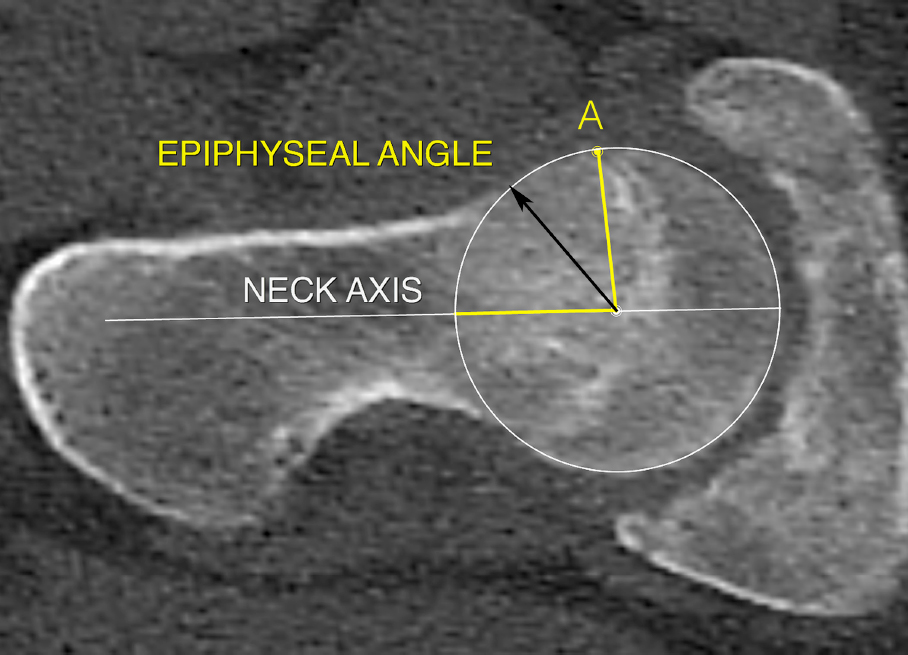
Epiphyseal angle is defined by the neck axis and a line from the centre of the femoral head to the most lateral extension of the epiphyses (point A). The epiphyseal angle is a measurement of epiphysis extension around the metaphysis: a smaller epiphyseal angle corresponds to greater epiphyseal extension into the metaphysis. The epiphyseal angle is different than the alpha angle (black arrow) that assesses the head-neck sphericity.
Statistical analysis
Reference values for tilt angle and epiphyseal angle were summarized by mean and sd along with lower and upper limits based on 95% of the reference sample stratified by age groups and gender. Linear mixed model analysis was used to assess variation in epiphyseal and tilt angles by age group and gender using unstructured and compound symmetry correlation structures, respectively. The linear mixed models accounted for correlated values given measurements on two hips and five planes on the same subjects. A p-value < 0.05 was considered significant. For intra- and interclass correlation analysis, measurements were repeated on 22 randomly selected individuals by the same observer (KPK) and a paediatric musculoskeletal radiologist (SDB) who were blind to patients’ demographics. Inter- and intraobserver reliabilities were calculated by estimating intraclass correlation coefficients along with 95% confidence intervals (Table 1).
Inter- and intrarater reliability
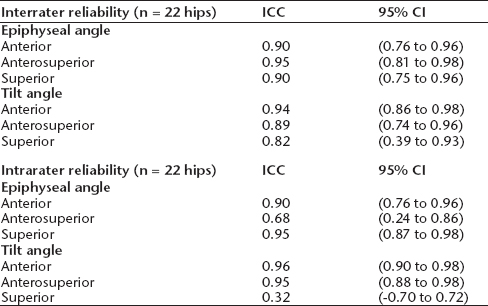
ICC, intraclass correlation coefficient; CI, confidence interval
Results
Epiphyseal tilt
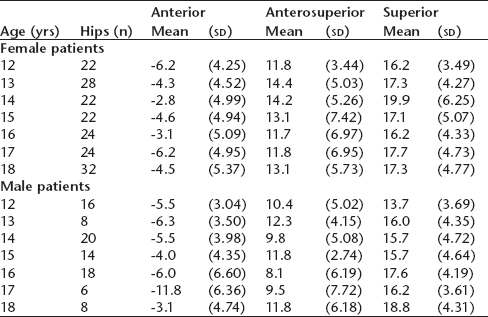
In the anterior plane, the epiphysis was found to be posteriorly tilted with a mean tilt angle of -4.5° (sd 4.96) in female patients and -5.6° (sd 4.97) in male patientss (Table 2). Male patients exhibited smaller tilt angles in the anterosuperior plane (p = 0.003) compared with female patients. No difference was detected between male and female patients in the anterior (p = 0.17) or superior (p = 0.06) planes (Fig. 4). Further, no difference was detected in tilt angle across all age groups by gender (p = 0.97) (Table 3).
Reference values for epiphyseal tilt stratified by CT plane and gender

Reference values for epiphyseal tilt stratified by CT plane, age group and gender
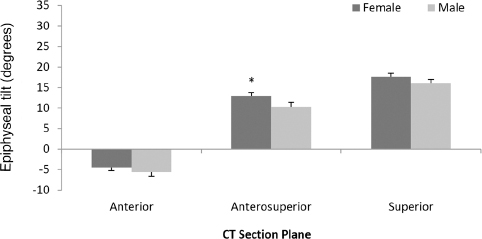
Graph comparing the mean epiphyseal tilt in the anterior, anterosuperior and superior planes in male and female patients. The asterisk corresponds to statistically significant differences (p < 0.05) between mean values in male and female patients.
Epiphyseal angle
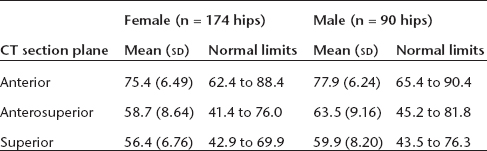
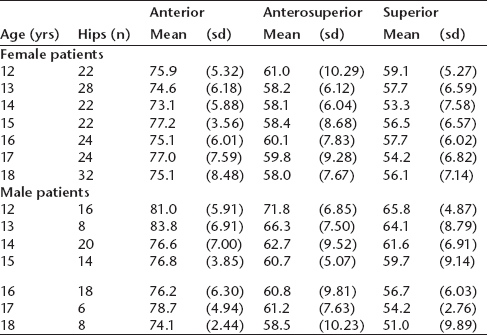
Male patients exhibited larger epiphyseal angles in the anterior (p = 0.02), anterosuperior (p < 0.001) and superior (p = 0.002) planes compared with female patients (Table 4; Fig. 5). The epiphyseal angle decreased with older age in the anterior (p = 0.03), anterosuperior (p = 0.001) and superior (p < 0.001) planes in male subjects. However, no variation in epiphyseal angle was found across all age groups for female subjects (p = 0.92) (Table 5).
Reference values for epiphyseal angle stratified by CT plane and gender
Reference values for epiphyseal angle stratified by CT plane, age group and gender
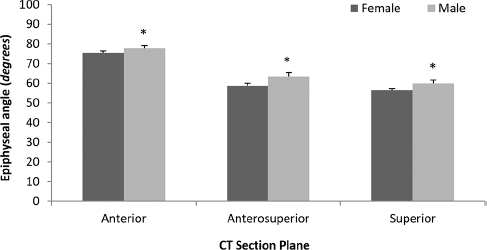
Graph comparing the mean epiphyseal angle in the anterior, anterosuperior and superior planes in male and female patients. Male patients were found to have higher epiphyseal angle (lesser epiphyseal extension) in all planes compared with female patients. Asterisks correspond to statistically significant differences (p < 0.05) between mean values in male and female patients.
Discussion
The orientation of the capital femoral epiphysis has been described as a potential mechanical factor associated with SCFE.1–4 The epiphyseal tilt, assessed on radiographs as the posterior epiphyseal slope angle has been used to identify hips at risk of developing a contralateral slip and to guide prophylactic treatment in patients presenting with unilateral SCFE.15,18–20 Abnormal epiphyseal extension around the metaphysis has been reported to precede the formation of a cam-type FAI deformity. Therefore, it is important to understand the age- and gender-specific variations of the epiphyseal tilt and extension during growth to establish how these physiologic variations may influence the pathology of SCFE and FAI. Two previous studies reported conflicting results about age-specific variation of epiphyseal tilt in children and adolescents and no information was available about gender-specific variations.11,13 Although the epiphyseal angle has been used to differentiate the morphology of hips associated with FAI, 21 to the best of our knowledge, normative data about epiphyseal angle during normal development is lacking. In this study, we investigated pelvic CT images from a large population of asymptomatic adolescents and showed that the epiphyseal tilt did not change with skeletal maturation from 12 to 19 years of age in male and female patients. No difference was observed for the epiphyseal tilt in the superior and anterior planes but male patients were found to have a smaller tilt angle in the anterosuperior plane. With regards to the epiphyseal angle which estimates the extension of the epiphysis around the metaphysis we noted that male patients had larger epiphyseal angle (less epiphyseal extension) in all planes compared with female patients. However, the epiphyseal angle decreased (the extension into the metaphysis increased) with older age in all planes in male but not in female subjects.
We found that the capital femoral epiphysis has a posteriorly oriented tilt in the axial plane with a mean posterior tilt of 4.5° in female and 5.6° in male patients. We are aware of only three previous studies investigating the capital femoral epiphysis tilt in the axial plane.11,13,14. Our findings are in line with Goodman et al 14 who investigated the proximal femur from an osteological collection and found that a posterior angulation of the femoral head ranged from -5° to 3°. However, our mean values of posterior tilt in the axial plane are slightly lower than those reported in two previous studies which may be explained by different methodology of obtaining the anterior plane 12 and the use of MRI instead of CT. 11 Kienle et al 11 noted that on 64 adolescents (127 hips; 32 male) the mean tilt angle in a MR axial plane was 11.6° for patients with an open physis. Monazzam et al 13 investigated normal developing children and adolescents between five and 19 years of age and found a mean tilt angle of 12.1° by measuring the axial oblique plane.
We did not find variation in the capital femoral epiphysis tilt in relation to age or gender in most planes assessed. Kienle et al 11 also found that the epiphyseal tilt did not change with age although no data was reported in regard to gender variations. On the contrary, Monazzam et al 13 found a small but significant effect of age on the tilt angle. The epiphysis was noted to have a less posteriorly tilt angle with growth, with each additional year of age decreasing the tilt angle by 0.27°. Contrary to our findings, Mirkopulos et al 1 showed that during normal development the proximal femoral physis orientation in the coronal plane changed from a horizontal to a more vertical orientation with maximum increase from nine to 12 years. It is possible that we were not able to capture age-specific changes in tilt in the coronal plane because we only included patients from 12 years and older.
The epiphyseal angle was found to decrease with age in all planes in male patients. However, we did not observe a variation in epiphyseal angle across all age groups in female patients. A smaller angle corresponds to larger epiphyseal extension into the metaphysis with growth in male patients. This is in line with the findings by Liu et al 22 who studied the anatomy of the epiphysis in femoral specimens from an osteological collection and showed an increase of the peripheral epiphyseal growth with increasing age. Kienle et al 11 also showed that the epiphyseal extension increased with age. Further, we noted that the epiphyseal angle was smaller in all planes in female compared with male patients. Therefore, boys were found to have less extension of the physis than girls. However, with growth the epiphyseal extension increased in boys but not in girls. Morris et al 16 proposed that epiphyseal extension may confer growth plate stability and reduce the risk of SCFE. However, abnormal extension of the epiphysis into the metaphysis has been described in adolescents who participate in vigorous sports as a precursor of cam-type FAI deformity.6,7,23–25 Our findings suggest a morphological difference between the capital femoral epiphysis during growth in male patients that may put them at higher risk to SCFE than female patients according to the theory proposed by Morris et al. 16 Given a higher prevalence of cam-type FAI in male patients, 26 it is possible that participation in vigorous sports accentuates the tendency to a smaller epiphyseal angle (larger epiphyseal extension) with growth in male patients, while female subjects are less susceptible as normal growth did not impact the epiphyseal angle in girls. Because girls typically undergo skeletal maturation at an earlier age than boys 27 it is possible that girls may be susceptible to such changes at an earlier age than boys. Nevertheless, out data did not capture any trend in variation of the epiphyseal angle in girls.
We acknowledge several limitations in our study. First, although medical records were reviewed to determine that the patients included in this study did not have a history of hip pathology, we did not obtain a history directly from the patients. This limited the ability of our study to determine the level of physical activity and potentially abnormal findings on hip examination. Secondly, given the retrospective study design we were not able to follow the patients to find out whether or not some developed hip symptoms later in life. However, at the time of measurement of the CT imaging the patients had no history or hip disorder. Thirdly, as our study was focused on assessing the femoral head-neck alignment during development we did not measure femoral version which is associated with the development of SCFE. 28 Finally, the clinical significance of our findings relates to the possible association of the variations described herein with the development of SCFE and cam deformity. We do not have anteroposterior and lateral radiographs of the hips to determine a correlation of the findings on the reformatted CT with radiographs. However, it is possible that the normative values reported herein may add to the evaluation of patients with SCFE and FAI. Further investigation is warranted to determine whether our findings may help improve the identification of patients at risk for developing SCFFE and cam deformity.
In conclusion, our results demonstrate that in adolescents without hip pathology the capital femoral epiphysis has a posterior tilt in the axial plane. We found no age-specific variations in the epiphyseal tilt and no difference in the epiphyseal tilt in male and female subjects in the superior and anterior plane, although in the anterosuperior plane the tilt was smaller in male patients. The epiphyseal angle was smaller in all planes in female compared with male patients; i.e. male patients had lower epiphyseal extension into the metaphysis compared with female patients. However, we noted a decrease in the epiphyseal angle which corresponds to an increase in epiphyseal extension with increasing age in male but not in female patients. The normative values of epiphyseal tilt and epiphyseal angle reported in this study may serve as additional information in the evaluation of adolescents with hip pain and as reference for future studies. Further research is needed to determine the threshold values of epiphyseal tilt and epiphyseal angle that could potentially be associated with risk for development of SCFE and cam-type FAI.
Footnotes
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
Y.-J. Kim has received honoraria from Orthopediatrics. All other authors declare that they have no conflict of interest.