
Abstract
Abstract
Purpose
To investigate changes in acetabular morphology during the follow-up of slipped capital femoral epiphysis (SCFE) and search for factors associated with acetabular dysplasia at skeletal maturity.
Methods
We evaluated 108 patients with unilateral SCFE (mean age at slip, 12.3 years sd 1.7) to skeletal maturity, with a minimum follow-up of two years (median 4.5 years; interquartile range 3.2 to 6.2). Acetabular parameters obtained from initial and most recent radiographs included the lateral centre-edge angle (LCEA), Tönnis angle (TA) and acetabular depth-width ratio (ADR). Acetabular dysplasia was considered for LCEA < 20° or TA > 10°. Femoral parameters consisted of the most recent head diameter, neck-shaft angle, neck length, articulotrochanteric distance and alpha angle.
Results
At SCFE onset, the affected hip showed a slightly lower LCEA (26.4° sd 6.1° versus 27.3° sd 5.7°; p = 0.01) and ADR (330 sd 30 versus 340 sd 30; p < 0.001) compared with the uninvolved hip. At final follow-up, the affected hip showed lower LCEA (24.5° sd 7.6° versus 28.8°sd 6.6°; p < 0.001) and ADR (330 sd 40 versus 350 sd 40; p < 0.001), and TA was larger (5.5° sd 5.4° versus 2.3° sd 4.2°; p < 0.001) compared with the uninvolved hip. Acetabular dysplasia was observed in 27 (25%) of 108 hips with SCFE. Femoral head overgrowth, age at slip and SCFE severity were independent factors associated with acetabular dysplasia (p < 0.05).
Conclusion
Acetabular coverage and depth are not increased in SCFE, and the acetabular coverage tends to decrease up to skeletal maturity. A potential disturbance in the acetabular growth and remodelling exists mainly for young children with severe SCFE, and a potential for acetabular insufficiency may be observed at the diagnosis and follow-up of SCFE.
Level of Evidence
Prognostic Level IV
Introduction
Slipped capital femoral epiphysis (SCFE) is one of the most important disorders affecting the adolescent hip. 1 Several factors have been suggested to play a role in the SCFE aetiology,2–11 including variations in acetabular morphology.11–16 Acetabular retroversion,11–13,15 increased acetabular coverage of the femoral head11,14–16 and deep acetabulum 16 are morphological factors that could potentially contribute to the development of SCFE. 16
These anatomical abnormalities may generate abnormal biomechanical forces.14,16–18 Coxa profunda with excessive superior acetabular coverage may induce shearing stress across the proximal femur growth plate.14,17,18 According to the contemporary concepts of femoroacetabular impingement (FAI), abnormal dynamic contact between the femoral head-neck junction and the acetabular rim may also lead to shearing forces, with a peripheral fulcrum. 3 The phenomenon may be accentuated by acetabular retroversion, coxa profunda and acetabulum protrusio. 3 Although acetabular overcoverage has been associated with SCFE development, a recent advanced imaging study using reformatted CT suggested that the acetabulum in SCFE is not deep. There were no differences in acetabular coverage and depth in comparison with matched-control individuals, however, the acetabulum in SCFE is more retroverted. 13
Aside from the potential effect of acetabular morphology in causing SCFE, residual deformities of the femur may potentially alter the residual acetabular growth and remodelling.19–21 Hypothetically, the dynamic conflict of the slip deformities against the acetabular rim may disturb the peripheral acetabular development. Moreover, a potential overgrowth of the femoral head may relatively decrease the acetabular coverage, and induce acetabular remodelling during the late skeletal growth in adolescence.
To our knowledge, no study has yet addressed the possible effects of SCFE-related femoral deformity on the residual acetabular development to skeletal maturity. Based on our clinical observations, a primary21,22 or secondary acetabular dysplasia21,23 may be occasionally found in hips affected by SCFE. The presence of acetabular dysplasia may influence the hip stability following a surgical hip dislocation approach for the treatment of SCFE deformities. 21
We therefore sought to investigate whether: (1) the acetabular coverage of the femoral head24,25 and acetabular depth26,27 are increased at the onset of SCFE; (2) the initial pattern of acetabular morphology is preserved following skeletal maturity, searching for the rate of acetabular dysplasia; and (3) residual deformities of the femur,28–30 slip severity 31 and age at slip are associated with changes in the acetabular morphology, in patients presenting with unilateral SCFE without contralateral involvement, in order to use the noninvolved hip for comparison.
Patients and methods
This retrospective longitudinal study was approved by the Institutional Review Board at our institution (Boston Children's Hospital). A total of 649 patients were evaluated at our institution between 2000 and 2014, with the initial diagnosis of SCFE. Patients with bilateral SCFE (n = 61) were excluded. For the 588 patients with unilateral SCFE, 44 underwent prophylactic contralateral epiphysiodesis because of the presence of endocrine or metabolic disorders, Down syndrome or autism. Further, 154 patients were excluded because of unavailable adequate pelvic radiographs 32 from the initial presentation, 65 patients who had a subsequent contralateral slip and 217 patients who were not yet skeletally mature (i.e. open triradiate cartilage, open capital femoral or trochanteric growth plate) at the most recent follow-up radiograph (Fig. 1).
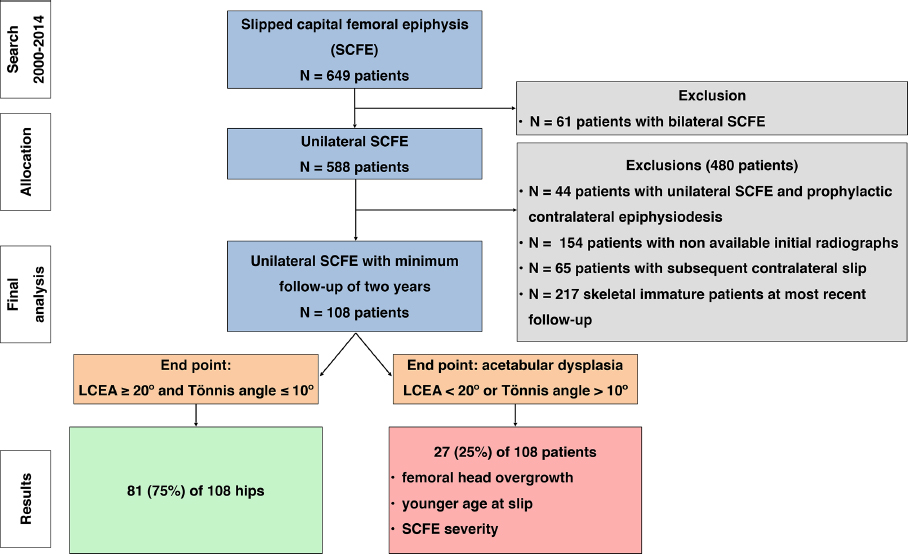
Flowchart of the study population (LCEA, lateral centre-edge angle).
The final sample included 108 patients who were followed for a minimum of two years (median 4.5 years, interquartile range 3.2 to 6.2), had no contralateral involvement and presented with closed proximal femur growth plate and triradiate cartilage. Mean age at initial diagnosis was 12.3 sd 1.7 years, 45% were males (49 boys, 59 girls). The left hip was affected in 55% of cases (59 left, 49 right). The status of the triradiate cartilage at the initial evaluation was wide open in 15 patients (14%), closing in 51 patients (47%) and closed in 49 patients (45%). 33 A descriptive analysis of the slip characteristics was performed, including the slip acuity,34,35 stability, 36 severity 31 and initial treatment (Table 1). There was one case of partial avascular necrosis of the capital epiphysis and one case of chondrolysis. The presence of hip pain on the affected side at the final follow-up was assessed, as well as any specific treatment recommended for hip dysplasia and instability.
Cohort characteristics (n = 108)
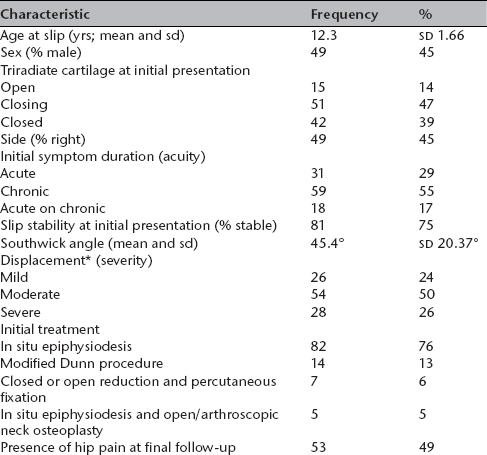
displacement was classified according to the initial Southwick angle of the affected hip: mild (less than 30°), moderate (between 30° and 60°) and severe (more than 60°) slips.
One orthopaedic surgeon (D.A.M.) with nine years of practise performed the radiographic measurements. For the affected and non-affected hips, the acetabular morphology was assessed in anteroposterior pelvic radiographies at two time points: initial unilateral SCFE presentation and the most recent radiographic evaluation. The acquisition protocol for anteroposterior radiographs consisted of the supine positioning of the patients, with vertical x-ray just above the pubic symphysis and 120 cm from the film. 37 If the initial preoperative radiographs had no adequate pelvic tilt (1 cm to 3 cm distance between symphysis pubic and coccyx, symmetry for obturator foramina), 32 the immediate postoperative radiograph was evaluated (17 out of 108 patients; 16%). Acetabular radiographic parameters consisted of the lateral centre-edge angle (LCEA), 24 Tönnis angle, 25 acetabular depth-width ratio (ADR), 26 coxa profunda sign 27 and crossover sign 38 (Fig. 2). The most lateral sclerotic point of the acetabular sourcil 39 was selected as a reference point for measuring LCEA, Tönnis angle and ADR. To assess LCEA in hips with moderate and severe SCFE deformities, the femoral head centre was determined using as a control the best fit circle of the capital epiphysis, under the guidance of the acetabular centre. 40 The use of the acetabular centre to assess LCEA has previously been validated in SCFE. 14 The acetabulum was classified as profunda if the acetabular fossa was medial to or touching the ilioischial line. 27 By the time of the initial presentation the ossification of the anterior or posterior acetabular rim41,42 was not visually complete in 17 skeletally immature patients (17/108; 16%), hindering the evaluation of the crossover sign. For the majority of patients (91/108; 84%), there was sufficient ossification of the anterior and posterior acetabular wall, allowing for the assessment of the crossover sign at the time of SCFE diagnosis. We defined as acetabular dysplasia hips with a LCEA < 20° 24 or Tönnis angle > 10° 37 .
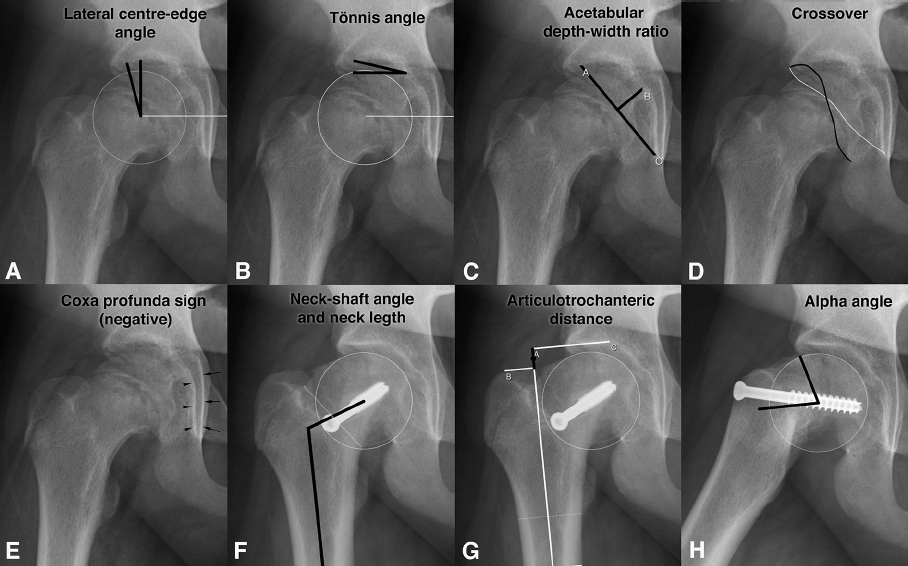
Description of the acetabular and femoral radiographic parameters. Radiographs of a boy with right slipped capital femoral epiphysis, at two time points, a) to e) from initial presentation at 13 years old; f) to h) from the most recent evaluation, at 15 years old: (
To evaluate femoral morphology, radiographic parameters were obtained from the most recent anteroposterior and lateral radiographic studies. Exception was made for patients who underwent surgical correction of FAI during the follow-up (28 out of 108 patients (26%) underwent femoral osteotomy and/or osteoplasty, 3.4 years sd 2.4 following the initial SCFE treatment) and for whom the femoral measurements were performed before FAI surgery in order to capture the original SCFE deformity. The lateral radiograph was obtained using the Lauenstein frog-leg view (hip is flexed to ∼45° and abducted to ∼45°, knees flexed to 90° and both feet are placed together) 43 or Dunn incidence (flexion ∼90°, abduction ∼45°). 37 Femoral radiographic parameter consisted of the anteroposterior and lateral alpha angle, 29 the articulotrochanteric distance (ATD), 30 the neck length, 28 the neck-shaft angle and the head diameter ratio (head diameter of the affected/uninvolved hip) 44 (Fig. 2).
Statistical analysis
We randomly selected 20 patients (40 hips) to assess the reliability across two independent and blind raters (two paediatric orthopaedic surgeons (A.D.P. and D.A.M.) with two and nine years of practise in hip preservation surgery, respectively), using the kappa (k) statistics 45 and intraclass correlation coefficient with a two-way, mixed-effects model, 46 along with 95% confidence intervals (CI). Inter- and intrarater agreement were substantial to excellent for all measurements, except for the alpha angle and crossover signs (moderate to excellent agreement) (Table 2).
Reliability analysis for the measured parameters of the hip in patients with unilateral slipped capital femoral epiphysis patients at skeletal maturity. Kappa analysis and intraclass correlation with a two-way mixed-effects model for consistency of agreement was applied to quantify inter- and intraobserver reliability, between two observers
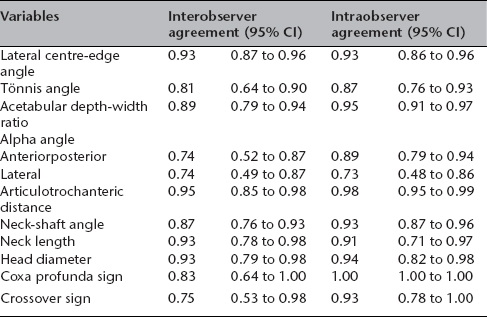
CI, confidence interval
Demographic, SCFE and radiographic characteristics were summarized for the cohort. Acetabular measurements were compared across SCFE and contralateral sides preoperatively and at most recent follow-up. Femoral measurements were compared, at most-recent follow-up, across acetabular dysplasia outcome. Continuous characteristics were summarized by mean and sd or median and interquartile range (25th to 75th percentile), while categorical characteristics were summarized by frequency and percentage.
In order to evaluate potential differences in acetabular morphology associated with the surgical treatment of FAI in the subgroup of 28 patients, we compared femoral and acetabular parameters across patients without and with FAI surgery (Table 3). Patients who underwent FAI surgery had greater anteroposterior and lateral alpha angles, but no differences were found in acetabular parameters between groups, suggesting little or no influence of the surgery in the subsequent analysis. Additionally, the identification of the femoral head centre may be difficult in a hip after SCFE. In order to evaluate potential influence of femoral deformities on LCEA measurements, we performed a correlation analysis between LCEA and alpha angle. No significant correlation was found between LCEA and anteroposterior alpha angle (Spearman coefficient = -0.12; p = 0.23) or LCEA and lateral alpha angle (Spearman coefficient = -0.09; p = 0.33), suggesting little or no influence of the proximal femur deformities in LCEA assessment.
Acetabular and femoral measurements of the affected hip in patients with or without femoroacetabular impingement surgery performed during the follow-up, and patients with or without hip pain at final follow-up. Values are described as mean and sd for continuous variables, or frequency and percentage for binary variables
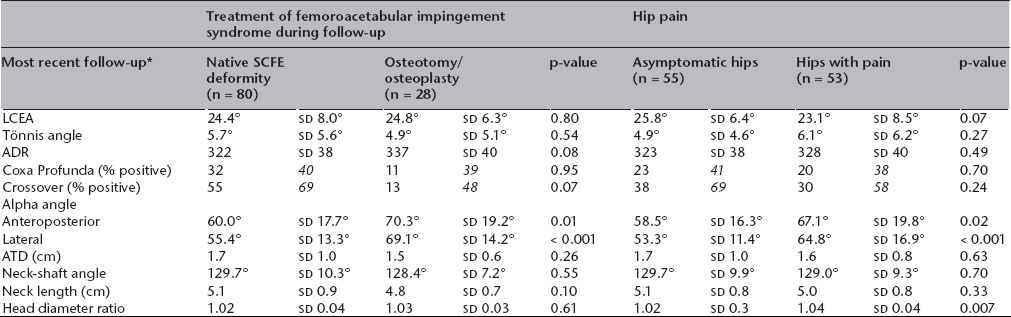
the last radiograph before the femoral surgery was used to measure femoral parameters in the osteotomy / osteoplasty subgroup
SCFE, slipped capital femoral epiphysis; LCEA, lateral centre-edge angle; ADR, acetabular depth-width ratio; ATD, articulotrochanteric distance
Paired t-tests and chi-squared tests were used to compare acetabular measurements between SCFE and contralateral sides and to evaluate change from preoperative to most-recent follow-up. Mean differences along with 95% CI were estimated for change in radiographic measures. Independent t-tests and Fisher's exact tests were used to compare acetabular and femoral measurements across dysplasia groups. Multivariable logistic regression was used to assess the effects of femoral measurements, SCFE severity (mild, moderate or severe slip) and age at slip on the development of acetabular dysplasia as independent variables, defined by LCEA < 20° or Tönnis angle > 10°. Odds ratios (OR) along with 95% CIs were estimated for significant effects. All tests were two-sided and p-values less than 0.05 were considered significant.
Results
At the onset of SCFE, the acetabular coverage of the femoral head and acetabular depth were not increased in the hip affected by SCFE, in comparison with the contralateral uninvolved side. On the contrary, affected hips had lower LCEA (26.4° sd 6.1° versus 27.3° sd 5.7°; p = 0.01) and ADR (330 sd 30 versus 340 sd 30; p < 0.001) at the initial presentation. No differences were detected in Tönnis angle (4.2° sd 3.5° versus 3.8° sd 2.8°; p = 0.17), prevalence of coxa profunda (42% versus 49%; p = 0.34) and crossover signs (71% versus 64%; p = 0.34) (Table 4).
Acetabular measurements for affected and contralateral sides (n = 108). Values are described as mean and sd for continuous variables, or frequency and percentage for binary variables
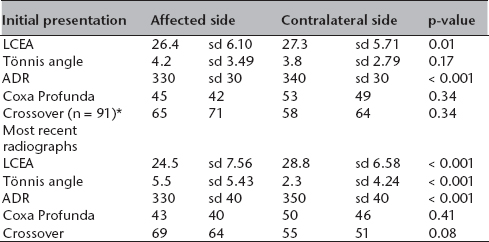
the number in parentheses represents the number of hips with available data for the given characteristic
LCEA, lateral centre-edge angle; ADR, acetabular depth-width ratio
At the final follow-up, we found that hips affected by SCFE ended up with a decrease in acetabular coverage of the femoral head, and shallower acetabulums compared with the uninvolved side (Figs 3 and 4). Compared with the initial presentation, differences increased for LCEA (24.5° sd 7.6° in the affected side versus 28.8° sd 6.6° in the contralateral side; p < 0.001) and ADR (330 sd 40 versus 350 sd 40; p < 0.001), and the Tönnis angle was eventually larger on the affected hip (5.5° sd 5.4° versus 2.3° sd 4.2°; p < 0.001). No differences were detected with respect to the prevalence of coxa profunda (40% in the affected side versus 46% in the contralateral side; p = 0.34) and crossover signs (64% versus 51%; p = 0.08). While the uninvolved acetabulums showed a tendency to maintain the pattern of femoral head coverage, the affected side had a worsening in the femoral head coverage parameters. Changes from the initial presentation to the most recent evaluation were identified on the contralateral uninvolved hip, in which the LCEA (+1.5°; 95% CI 0.5° to 2.5°; p = 0.003) and ADR increased (+10; 95% CI 7 to 18; p < 0.001) and Tönnis angle decreased (-1.5°; 95% CI -2.2° to -0.4°; p < 0.001). However, an inverse growth pattern was observed in the affected hip, with a decrease in LCEA (mean difference = -1.9°; 95% CI -3.1° to -0.7°; p = 0.002) and increase in Tönnis angle (+1.3°; 95% CI 0.4° to 2.2°; p = 0.006). No change was detected in ADR (330 sd 30 versus 330 sd 40; p = 0.41) (Table 4).
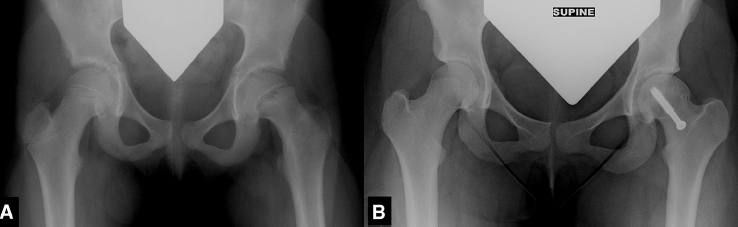
Anteroposterior radiographs of a girl with left slipped capital femoral epiphysis (SCFE): (
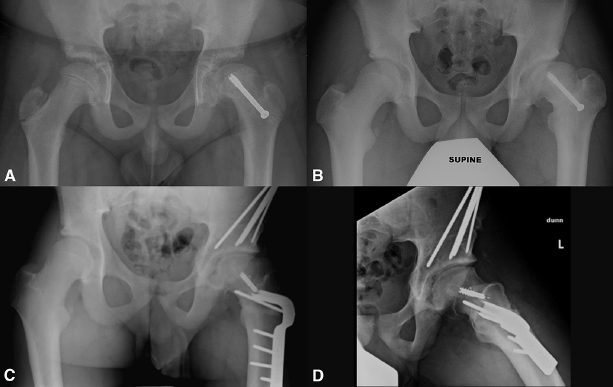
Anteroposterior radiographs of a boy with left slipped capital femoral epiphysis (SCFE) immediately after in situ epiphysiodesis: (
According to the multivariable analysis, we found that femoral head overgrowth, the severity of slip and the age at disease onset were each independent factors associated with the occurrence of acetabular dysplasia in SCFE. A total of 27 out of 108 affected hips (25%) exhibited acetabular dysplasia (i.e. LCEA < 20° or Tönnis angle > 10°) at most-recent follow-up, while 15 affected hips (14%) were considered dysplastic at initial presentation (p = 0.01). There were no differences detected across dysplastic versus non-dysplastic subgroups with respect to proportion of hip pain, alpha angle, ADR, neck-shaft angle or neck length (p > 0.05, Table 5). It was found, however, that dysplastic hips exhibited a larger femoral head diameter ratio (p < 0.001). Multivariable analysis determined that the head-diameter ratio was the only femoral measurement associated with acetabular dysplasia. For each 1% increase in the diameter ratio, the odds of dysplasia increased by 30% (OR = 1.3; 95% CI 1.1 to 1.6; p = 0.002). The severity of slip was found to be an independent factor associated with the development of acetabular dysplasia in SCFE. Hips with a severe slip had six-times increased odds compared with mild slips (OR = 6.1; 95% CI 1.1 to 35.1; p = 0.04). The age at slip was also an independent factor for the development of acetabular dysplasia in SCFE. For each year of increase in age at slip diagnosis, the odds decrease by 30% (OR = 0.7; 95% CI 0.5 to 1.0; p = 0.03) (Table 5).
Morphologic characteristics and age at slip according to the subgroups with or without acetabular dysplasia of the affected hip at the final follow-up. Values are described as mean and sd for continuous variables, or frequency and percentage for binary variables
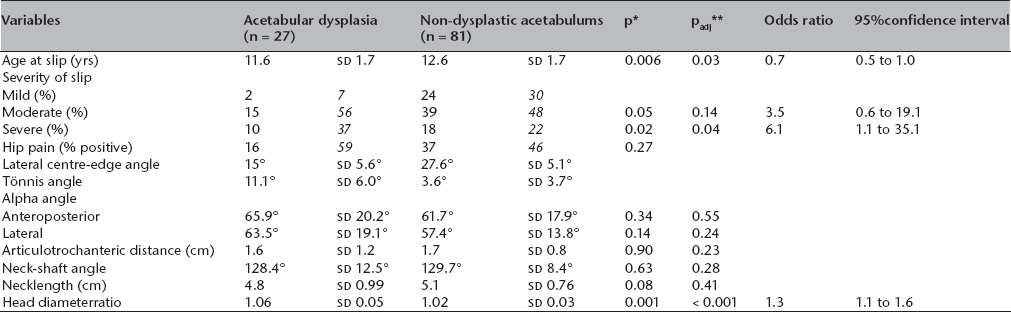
p-values represent univariate comparisons
p-values adjusted using multivariable logistic regression
In all, 55 (51%) of 108 patients had no hip symptoms. The remaining 53 patients (49%) had hip pain at final follow-up. No differences were observed in acetabular parameters between symptomatic and asymptomatic hips. Only the alpha angle (anteroposterior and lateral) and femoral head overgrowth were associated with hip pain (Table 3). Three patients developed hip pain associated with clinical instability (positive apprehension test) and acetabular dysplasia. The periacetabular osteotomy was performed in two of these three patients (followed by clinical improvement), and recommended but not yet performed for the third patient.
Discussion
Recently, the historical concept that SCFE is associated with increased acetabular coverage or depth11,14–16 has been brought into question by CT findings suggesting that the acetabulum is not deep and there is no acetabular overcoverage of the femoral head in SCFE. 13 Notably, there is little attention given to the prevalence of acetabular dysplasia as an associated comorbidity in SCFE; and considering the critical concern of an initial SCFE event, the acetabular dysplasia may be not promptly recognized.22,47 Additionally, there is a question as to whether a secondary acetabular remodelling may develop following an early SCFE presentation with residual femoral deformities, in a mechanism similar to Legg-Calvé-Perthes disease.19–21 To our knowledge, no prior study has specifically addressed the effect of SCFE on the acetabular growth up to the skeletal maturity. In this study, we longitudinally evaluated patients with unilateral SCFE that did not experience a contralateral slip, with a minimum of two years. Our results suggested that the acetabular coverage and depth are not increased in hips initially affected by SCFE. Further, we found that SCFE may alter the remaining acetabular growth or may induce a post-SCFE acetabular remodelling, leading to decreased acetabular coverage of the femoral head. Independent factors associated with the presence of acetabular dysplasia at skeletal maturity in SCFE were the age at slip, the severity of SCFE and the femoral head overgrowth.
At the initial SCFE presentation, we did not observe increased acetabular coverage and depth in the affected hip compared with the contralateral unaffected side. In contrast, some previous evidence suggested that the acetabular coverage is increased in SCFE. Kitadai et al 14 and Monazzam et al 15 did not find differences between the affected and uninvolved hips in unilateral SCFE, and both hips presented with increased LCEA angle compared with control individuals. In patients with unilateral SCFE, Sankar et al 11 suggested that the uninvolved side had increased acetabular coverage, assessed by LCEA and Tönnis angle, compared with control patients. A deep acetabulum was found in 52% of hips with SCFE and it may potentially influence the slip stability. 16 Conversely, Hesper et al 13 suggested that a hip with SCFE has a similar LCEA and ADR compared with normal hips of matched-control individuals. Acetabular retroversion has been commonly observed in SCFE.11–13,15 Similarly, we identified a high proportion of crossover sign in the hip with SCFE and also in the uninvolved hip.
At skeletal maturity, we observed that the noninvolved acetabulum continued to grow and to increase the femoral head coverage, while in hips with SCFE, the superior acetabular coverage worsened during the follow-up. Some factors involving the relationship between the femur and the acetabulum could be hypothetically associated with the acetabular remodelling and decrease the acetabular coverage in SCFE. 48 The process of bone healing can stimulate the femoral capital overgrowth. 28 Indeed, we found that the femoral head diameter increased 6% compared with the contralateral noninvolved side, while a normal range of capital asymmetry within 2% to 3% has been reported.49,50 Femoral head overgrowth itself may reflect in lateralization of the femoral head centre and lower LCEA. Long-term studies will be worthwhile to determine if the relative decrease in femoral head coverage associated with capital overgrowth is associated with clinical instability or late dysplastic degeneration. Additionally, the combination of epiphyseal displacement in SCFE, with the resultant epiphysiodesis may result in a short femoral neck, a relatively high greater trochanter and loss of concavity at the femoral head-neck junction, each or in combination may lead to FAI mechanical conflicts. 48 These conflicts may potentially disturb the secondary ossification of the acetabular rim and terminal growth of the acetabulum. 13
In order to identify which factors were associated with the decrease in acetabular coverage in skeletally mature patients with SCFE, we conducted a multivariate analysis including demographic, acetabular, femoral and SCFE characteristics. Although our results did not confirm the hypothesis that FAI deformities alter the residual acetabular growth, we must interpret this with caution, since some patients underwent FAI treatment during the follow-up. We identified that the age at slip, severity of SCFE and the capital overgrowth are independent factors associated with the development of acetabular dysplasia in SCFE. Hip pain was not statistically associated with radiographic acetabular dysplasia in the present cohort. However, three symptomatic patients presented with clinical evidence of acetabular dysplasia and hip instability at final follow-up, and two of them underwent periacetabular osteotomy.
This study has limitations. First, the retrospective design allowed for methodological bias such as suboptimal pelvic radiographic positioning and a selection bias due to a considerable decrease in the number of initial patients. We rejected initial radiographs with poor positioning to minimize improper measurements. Furthermore, the decrease in the initial number of patients was necessary to assure follow-up to skeletal maturity, allowing evaluation of the uninvolved contralateral hip in an intra-individual pairwise comparison. The majority of the 217 patients who had not reached skeletal maturity were lost to follow-up. This decrease in the number of patients is expected for reference hospitals, which receive patients from other centres. However, some patients with persistent pain are more likely to keep following up to older ages. Even after these exclusions, a considerable number of patients were analyzed with a median follow-up of 4.5 years. Second, the SCFE onset usually occurs at an age in which the acetabulum is not completely ossified. The acetabular rim was not identifiable in a few patients, which were not included in the pairwise comparison of the crossover sign using the contralateral hip at the same study period, and the same hip for follow-up analysis. Third, all measurements were performed by the same orthopaedic surgeon, however, we identified substantial to excellent intra- and interobserver agreement, except for the alpha angle and crossover sign. We believe that our reliability is in line with the literature.13,29,44,51–53 Fourth, we acknowledge that differences that we found in LCEA may not be clinically significant for many cases; however, initially equivocal acetabular coverage may be negatively influenced by an insufficient residual acetabular growth or remodelling following SCFE. Fifth, all measurements were performed using conventional radiographs, which are not ideal to depict the 3D complex anatomy of the acetabulum. Sixth, a subset of patients underwent surgical treatment of FAI deformity. Although the surgery would have the potential to change the natural evolution, we observed no differences in acetabular parameters between patients who underwent FAI surgery and those who did not. We believe that the original SCFE deformity could have influenced the acetabular development despite subsequent FAI treatment. Finally, the morphology of the contralateral uninvolved side in unilateral SCFE may resemble a slip-like deformity, 54 and we do not have a matched-control group of healthy individuals to compare the acetabular morphology across time.
In conclusion, our results suggest that the acetabular coverage of the femoral head and the acetabular depth are not increased in SCFE. Even more importantly, we found that hips with SCFE tend to develop decreased acetabular coverage at skeletal maturity, and approximately 25% of patients met the criteria for the definition of hip dysplasia. Age at initial slip, severity of slip and femoral capital overgrowth are factors associated with the development of acetabular dysplasia in SCFE. The presence of acetabular insufficiency in association with SCFE has previously been under-reported, and its recognition may be important. Although we cannot yet comment on the effect of this phenomenon on treatment decision-making, continuing studies with large numbers and advanced imaging will be important to understand a clinical significance of the acetabular morphology in SCFE.