
Abstract
Purpose
Traditionally, flexible intramedullary nails (FINs) are not to be used to fix femur fractures in patients > 50 kg (110 lbs). However, studies have not examined the efficacy of this technique in overweight and obese patients who may be under this ‘weight cutoff’. The purpose of this study was to assess how patient body mass index (BMI) impacts the treatment of paediatric femur fractures managed with FINs.
Methods
Retrospective data was collected on all paediatric patients treated with FINs for diaphyseal femur fractures at a single tertiary care institution over a ten-year period. BMI was calculated and categorised according to the Centre for Disease Control BMI Calculator for Children and Teens. Patients with comorbidities affecting bone quality were excluded.
Results
A total of 54 patients met inclusion criteria. In all, 14 patients were underweight, 20 were within a normal weight range, and 20 were overweight/obese. There was no correlation between BMI and mean shortening (underweight: 7.1 mm, normal weight: 5.2 mm, overweight/obese: 7.2 mm; p = 0.55). There was no correlation between BMI and mean anterior/posterior angulation (underweight: 3.1°, normal weight: 3.8°, overweight/obese: 3.3°; p = 0.93). There was no correlation between BMI and varus/valgus angulation (underweight: -0.86°, normal weight: -0.5°, overweight/obese: -1.25°; p = 0.89). Three cases fit malunion criteria. One of these patients fell into the ‘underweight’ category and two patients fell into the ‘normal weight’ category.
Conclusion
We found no association between BMI and malunion in FIN fixation of femoral diaphyseal fractures in children. All cases of malunion were seen in underweight or normal weight patients.
Introduction
The use of flexible intramedullary nails (FINs) for the treatment of paediatric femur fractures is well established. FINs act as an intramedullary splint, providing internal stabilisation to the fractured bone while also allowing for earlier ambulation, less angulation, and fewer economic and social side effects than alternatives like spica casts, rigid reamed nails, or external fixation devices.1–4 Multiple studies have demonstrated high rates of excellent or satisfactory results and low rates of major complications when FINs are used to fix paediatric femur fractures, particularly in young children with stable fracture patterns.1,4–9
However, complication rates increase when the use of FINs is expanded to older and heavier patients. Moroz et al 7 reported that patients > 49 kg (108 lbs) were five times more likely to have a poor outcome than patients weighing < 49 kg (108 lbs), although weight was not a sensitive test for detecting poor outcomes. Several other studies have noted that weight > 50 kg (110 lbs) is a predictor for increased complication rate, more severe complications, and poorer outcomes.10,11
It is unclear if this association between high weight and increased complications is restricted to those patients > 49 kg (108 lbs) or if it may be expanded to patients with high body mass index (BMI). Weiss et al 11 suggests that obese children < 50 kg (110 lbs) may present more complications, but did not directly examine this issue. With recent trends in childhood obesity there may be an increased prevalence of young children who fall into the overweight/obese category based on BMI but weigh < 49 kg (108 lbs). There is, to our knowledge, no literature assessing the efficacy of FINs for these children. Our purpose was to assess the impact of patient BMI on maintenance of reduction and rates of complication in paediatric femur fractures treated with FINs.
Methods
Institutional review board approval from Children's Hospital Los Angeles was granted for this study.
All patients with diaphyseal femur fractures treated with FINs between 2004 and 2014 at the participating centre (Children's Hospital Los Angeles) were eligible for inclusion (n = 73). Patients were excluded if they weighed > 49 kg (108 lbs) (n = 3), had comorbidities affecting bone quality, such as osteogenesis imperfecta, mucopolysaccaridoses, or dwarfism (n = 3), failed to follow up until time of radiographic union (n = 11), or had inadequate radiographic documentation of their fracture (n = 2).
BMI was calculated and categorised according to the Center for Disease Control (CDC) BMI Calculator for Children and Teens. 12 Patients were divided into underweight, normal weight, and overweight/obese groups. Underweight was defined as a BMI < fifth percentile for age, normal weight was defined as the fifth to < 85th percentile for age, and overweight/obese was defined as ≥ 85th percentile for age.
Charts and radiographs were reviewed to determine demographic information, mechanism of injury, fracture type, post-surgical complications, and fracture angulation and shortening at time of bony union. Complications were defined as painful implants, prominent implants, nonunion, malunion, and revision surgery for any reason. Fractures were considered to be malunited if there was shortening > 2 cm, angulation in the sagittal plane (anterior/posterior) > 15°, or coronal angulation (varus/valgus) > 10°.
One-way analysis of variance was used to determine the relationship between BMI groups and shortening, sagittal angulation, coronal angulation, and complication rate. The chi-square analysis or Fisher's exact test were used to analyse the relationship between BMI groups and development of specific post-surgical complications.
Results
There were 54 patients who met the inclusion criteria. They were 44 (81.5%) male patients and ten (18.5%) female patients. Mean age at time of injury was 6.4 years (1.7 to 17.7; standard deviation (sd) 3.1). The most common mechanisms of injury were: fall (26, 48.1%), motor vehicle accidents (15, 27.8%), and pedestrian versus automobile accidents (six, 11.1%).
In all, 14 (26.0%) patients were underweight, 20 (37%) were normal weight and 20 (37%) were overweight/obese.
Mean shortening was as follows in the groups: underweight = 7.1 mm (0 to 21.7; sd 7.2); normal weight = 5.2 mm (0 to 18; sd 6.3); overweight/obese = 7.2 mm (0 to 18.1; sd 6.6) There was no correlation between BMI group and shortening (p = 0.56) (Table 1) (Fig. 1).
Shortening and angulation by body mass index (BMI) category.
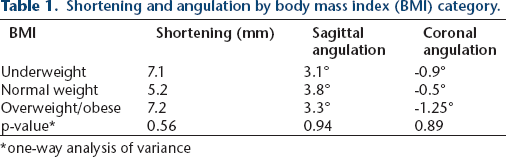
one-way analysis of variance
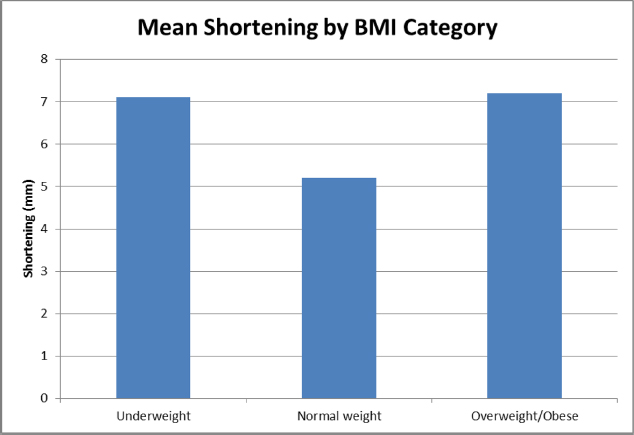
Mean shortening by body mass index (BMI) categories. There was no association between BMI and shortening (p = 0.56).
Mean angulation in the sagittal plane was as follows in the groups: underweight = 3.1° (-2° to 10°; sd 3.5°), normal weight = 3.8° (-12° to 17°; sd 6.9°), overweight/obese = 3.3° (-7° to 13°; sd 5.4°). There was no correlation between BMI group and angulation in the sagittal plane (p = 0.94) (Table 1) (Fig. 2).
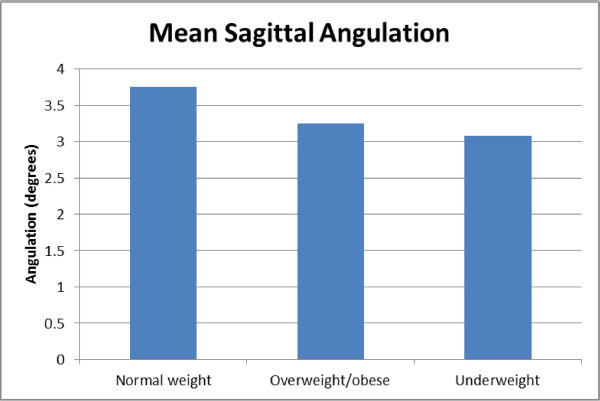
Mean sagittal angulation by body mass index (BMI) categories. There was no association between BMI and sagittal angulation (p = 0.94).
Mean coronal angulation was as follows in the groups: underweight = -0.9° (-10° to 4°; sd 4.3°), normal weight= -0.5° (-15° to 8°; sd 5.0°) overweight/obese = -1.25° (-15° to 8°; sd 4.7°). There was no correlation between BMI group and coronal angulation (p = 0.89) (Table 1) (Fig. 3).
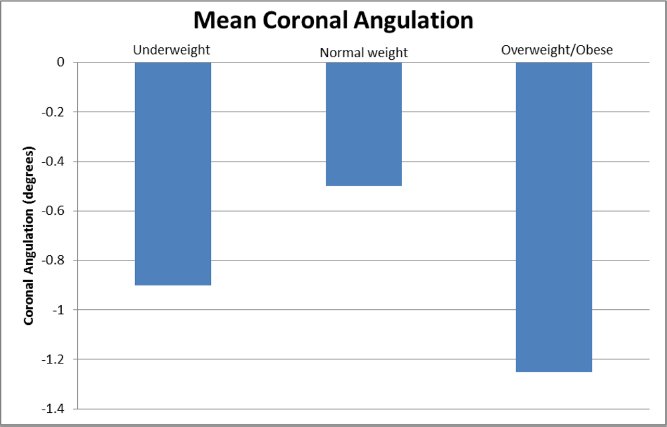
Mean coronal angulation by body mass index (BMI) categories. There was no association between BMI and coronal angulation (p = 0.89).
A total of 22 patients (40.7%) experienced 23 complications. There were 13 cases of painful hardware, six of prominent hardware, three cases fitting malunion criteria, and one case of limited range of movement. Development of complications was not associated with BMI (p = 0.89). Of the three patients who developed malunions, one was underweight and two were normal weight. For a breakdown of complications by BMI group, see Table 2.
Complications by body mass index (BMI) category.

chi-squared of Fisher's exact test
Discussion
Complication rates with FINs are significantly increased in patients weighing > 49 kg (108 lbs),7,10,11 but there is little information on complication rates in patients who weigh < 49 kg (108 lbs) but are still overweight or obese. The purpose of this study was to determine the impact of patient BMI on maintenance of reduction and rates of complication in paediatric femur fractures treated with FINs.
We found no association between high BMI and maintenance of reduction or development of malunion in children. All cases of malunion were seen in underweight 1 or normal weight 2 patients. Shortening, sagittal angulation, and coronal angulation were similar across all BMI groups.
BMI also had no association with development of other complications. While rates of complication were slightly lower in the underweight group (35.7%) than in the normal weight and overweight/obese groups (45%), this was not statistically significant (p = 0.89). It is possible that this represents a trend which our study is underpowered to detect. Variations in surgeon technique between smaller and larger patients may also have had an effect on complications, although this is impossible to account for in a retrospective study.
Overall complication rate in this study was 40.7%, but only 5.6% (3/54) were major complications. The most common issues we encountered with FINs were pain at the nail site (24.1%, 13/54) and nail prominence (11.1%, 6/54), which is typical in the literature.1,4–9 The incidence of painful hardware increased with BMI (underweight: 14.3%, 2/14; normal weight: 25%, 5/20; overweight/obese: 30%, 6/20). Nail prominence occurred slightly more frequently in the underweight group (14.3%, 2/14) than the normal or overweight/obese groups (10%, 2/20). Neither of these differences were statistically significant.
In a previous study by Weiss et al, 11 there was a higher incidence of poor outcomes and complications in obese patients, but they observed that the rate of complication appeared to be related more to weight than to BMI as the majority of their obese patients weighed > 50 kg (110 lbs). The results of our study seem to confirm this observation, as rates of poor outcomes and complications are similar across all BMI groups in patients weighing < 49 kg (108 lbs).
This study is limited by its retrospective nature. Due to the constraints of the radiographs available for retrospective review, sagittal angulation was measured from the shaft of the femur rather than from comparison with the normal bow of the contralateral side. Since normal femoral bow can contribute several degrees to the measurement of anterior angulation, the inability to compare measurements with a reference normal may have skewed our data high. In addition, all radiographs were reviewed by a single observer. While this reduces inter- and intraobserver variability, it is possible that error was introduced into the measurements. However, these were problems inherent to all patients included in the study and thus it is not likely that they altered final data analysis to an extreme degree. In addition, the retrospective nature makes it difficult to control for surgeon technique. Previous literature has shown that a minimum 80% canal fill is an important factor in maintenance of fracture alignment,5,6,13,14 but we were unable to standardise canal fill retrospectively. Several patients in this study had < 80% canal fill, which may have skewed results. This study also had a relatively small number of patients which may have precluded the development of statistically significant results.
Use of FINs to fix paediatric femur fractures is well established. While the rate of minor complications is high, long-term results using the nails is satisfactory to excellent. Prior research has shown that complication rate increases in heavier patients, but it was unknown if this was applicable to patients with a lower weight but high BMI. This study suggests that FINs may be safely used in overweight and obese patients weighing < 49 kg (108 lbs).
Footnotes
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
Authors Ena Nielsen, Nana-yaw Bonsu and Rachel Goldstein declare that they have no conflicts of interest.
Author Lindsay Andras has stock or stock options with Eli Lilly; receives publishing royalties, financial, or material support from Orthobullets; is a board or committee member for the Pediatric Orthopaedic Society of North America and the Scoliosis Research Society; is a member of the speaker's bureau for Biomet, Medtronic and Nuvasive; and serves as a reviewer for the Journal of Pediatric Orthopaedics.