
Abstract
Abstract
Purpose
To compare patient characteristics, operative time, estimated blood loss (EBL), postoperative length of hospital stay (LOS) and complications after insertion and removal of submuscular plates (SMPs) versus flexible nails (FNs) for paediatric diaphyseal femur fractures.
Methods
We reviewed records of 58 children (mean age, 7.7 years SD 2.0) with diaphyseal femur fractures who underwent treatment with SMPs (n = 30) or FNs (n = 28) from 2005 to 2017 (mean follow-up, 22 months SD 28). Patients with pathological fractures or musculoskeletal comorbidities were excluded. Alpha = 0.05.
Results
Insertion of FNs was associated with shorter operative time (ß = –24 mins) and less EBL (ß = –38 mL) (both, p < 0.001) compared with insertion of SMPs, after adjusting for fracture type and time from beginning of study period. Removal of FNs was also associated with shorter operative time (ß = –15 min) compared with removal of SMPs (p < 0.001). EBL during removal was similar between groups (p = 0.080). The FN group had a shorter LOS after insertion (ß = –0.2 d) compared with the SMP group (p = 0.032). Four patients treated with SMPs and three treated with FNs developed surgical site infections. Two patients treated with SMPs and seven treated with FNs experienced implant irritation that resolved with removal. No other complications occurred.
Conclusion
Compared with SMPs, FNs were associated with shorter operative time (for insertion and removal), less EBL (for insertion) and shorter post-insertion LOS in patients with diaphyseal femur fractures.
Level of Evidence
III
Keywords
Introduction
Paediatric diaphyseal femur fractures, with an estimated annual incidence of 19 per 100 000, 1 are the most common fractures requiring inpatient treatment in children. 2 In skeletally immature children aged older than five years, surgical fixation is the standard of care and is recommended by the American Academy of Orthopaedic Surgeons 3 over nonoperative methods such as spica casting 4 and skeletal traction.5–7 The use of flexible nails (FNs), which enables rapid mobilization with few complications,8–10 is a well established method for treating length-stable fractures in children aged five to 11 years.3,11 Its advantages include small incisions and relatively simple instrumentation. 12 The use of submuscular plates (SMPs), a newer method, has also been associated with few complications, satisfactory alignment and high patient satisfaction in treating diaphyseal fractures.13–15
Although SMPs and FNs have both shown excellent outcomes in previous studies, they have different biomechanical properties, and few studies have compared the outcomes of these methods. The relative lack of research comparing SMPs and FNs is reflected in the ‘very low quality evidence’ reported in a 2014 Cochrane review, which found only one study comparing the two methods. 16
Our goals were to compare the following practical implications of the chosen implants: operative time, estimated blood loss (EBL), postoperative length of hospital stay (LOS), and incidence of complications between skeletally immature children with diaphyseal fractures treated with SMPs versus FNs. We hypothesized that the use of SMPs would involve more blood loss and more time to insert and remove compared with FNs, and that the incidence of complications would be similar in the two groups.
Patients and methods
After obtaining institutional review board approval, we used Current Procedural Terminology 17 codes and medical billing information to identify paediatric diaphyseal femur fractures treated by one surgeon (PDS) from January 2005 to June 2017. We reviewed operative notes, clinical records and radiographs to determine skeletal immaturity (indicated by the presence of open growth plates), comorbidities, fracture type, mechanism of injury and treatment method. Skeletally immature children who underwent initial treatment of the fracture with SMPs or FNs were included. Children with pathological fractures or comorbidities with major musculoskeletal manifestations, such as osteogenesis imperfecta, skeletal dysplasia, spina bifida and cerebral palsy, were excluded.
Patient characteristics, such as sex and age, were obtained from clinical records; age was defined as age on the date of implant insertion. Mechanism of injury was categorized as recreational (e.g. falling from climbing bars, being tackled during football), motor vehicle accident (e.g. pedestrian struck by automobile, passenger in motor vehicle crash) or other (e.g. tripping and falling at home, crush injury from furniture). Patients were categorized as having isolated injuries or polytrauma (defined as having injuries with Abbreviated Injury Score ≥ 2 in two or more regions of the body).18,19
The primary outcomes were EBL and operative time for the initial implant insertion and removal procedures. Data on EBL during implant insertion and removal were obtained from operative notes; estimates were made by the surgeon and anaesthesia team members through intraoperative assessment of volume in the suction device and number of sponges saturated. Operative time was calculated as the number of minutes between ‘incision time’ and ‘surgery stop’ in the operating room nursing documentation. Discharge summaries, hospital records and follow-up clinic notes were reviewed to determine the length of postoperative hospital stay and incidence of the following complications: surgical site infection, implant irritation, leg-length discrepancy > 2 cm, heterotopic ossification, avascular necrosis, malunion and nonunion. Radiographic records were also reviewed for evidence of abnormal healing, including malunion and nonunion. Clinical documentation by the surgeon regarding the radiographs, as well as radiologists’ assessments for each image were reviewed; evidence of healed or healing fractures, anatomic alignment, complications and abnormal healing were noted.
Statistical analysis
Continuous data with a normal distribution are reported as the mean and sd and nonnormal continuous data are reported as the median and interquartile range. Categorical data are reported as frequencies and percentages. Fisher's exact and Pearson chi-squared tests were used to detect differences in categorical baseline characteristics between SMP and FN groups, where appropriate. Mann-Whitney U tests were used to detect differences in continuous baseline characteristics. Permutation tests for linear regression were performed to detect differences in continuous outcome variables while adjusting for time from the beginning of the study period and any significant differences in baseline characteristics between groups. Statistical analyses were performed with RStudio, version 1.0.143, software (RStudio, Inc, Boston, Massachusetts). Statistical significance was set at = 0.05 for all tests.
Results
Patient characteristics
In all, 30 patients treated with SMPs and 28 treated with FNs met the inclusion criteria. The mean ages were similar between groups (p = 0.131, Table 1). The sex distribution (p = 0.175) and fracture laterality (p = 0.746) were also similar (Table 1). In all, 57 of 58 patients had follow-up after implant insertion. One patient was lost to follow-up after initial implant insertion. The mean length of clinical and radiographic follow-up was 22 months sd 28 and 5.3 months sd 5.4, respectively.
Patient and injury characteristics of 58 skeletally immature children with diaphyseal femur fractures who underwent initial treatment with submuscular plates (SMPs) or flexible nails (FNs), January 2005 to June 2017
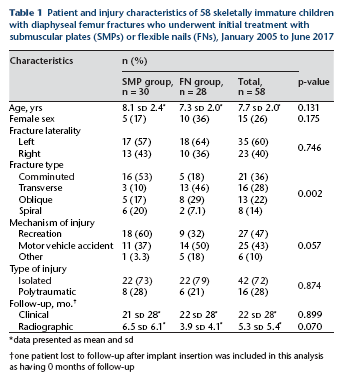
data presented as mean and sd
one patient lost to follow-up after implant insertion was included in this analysis as having 0 months of follow-up
Injury characteristics
There were 21 comminuted, 16 transverse, 13 oblique and eight spiral fractures. Comminuted fractures represented the largest proportion (16/30) of fractures treated with SMPs, and transverse fractures represented the largest proportion (13/28) of fractures treated with FNs. There was a significant association between fracture type and treatment method (p = 0.002). However, the fracture was not directly exposed with either implant; therefore, we felt that the fracture characteristics were not the primary determinants of our study variables. Mechanisms of injury included 27 recreational injuries, 25 motor vehicle accidents and six other injuries. In all, 42 patients experienced isolated injuries and 16 experienced polytrauma (Table 1).
Surgical outcomes
Because fracture type distribution differed significantly between the groups, we included fracture type, along with time from the beginning of the study period, as covariates in the regression model examining surgical outcomes. Neither fracture type nor time from 2005 significantly predicted EBL or operative time during insertion or removal procedures. Treatment with FNs, however, significantly predicted lower EBL during insertion (by 38 mL, p < 0.001), shorter operative time during insertion (by 24 minutes, p < 0.001) and shorter operative time during removal (by 15 minutes, p < 0.001). Treatment with FNs also predicted a shorter LOS after implant insertion by a mean of 0.2 days for all patients in the cohort (p = 0.032), as well as for patients with isolated injuries (p = 0.041) (Table 2).
Perioperative data from 58 skeletally immature children with diaphyseal femur fractures who underwent initial treatment with submuscular plates (SMPs) or flexible nails (FNs), January 2005 to June 2017
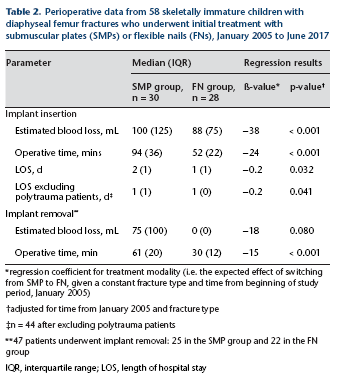
regression coefficient for treatment modality (i.e. the expected effect of switching from SMP to FN, given a constant fracture type and time from beginning of study period, January 2005)
adjusted for time from January 2005 and fracture type
n = 44 after excluding polytrauma patients
47 patients underwent implant removal: 25 in the SMP group and 22 in the FN group
IQR, interquartile range; LOS, length of hospital stay
Clinical and radiographic outcomes
No intraoperative or perioperative complications occurred in either group. Radiographic assessments, at a mean of 5.3 months sd 5.4 after insertion, showed evidence of healed or healing fracture and anatomic alignment or near anatomic alignment in all cases.
Prophylactic implant removal was recommended to all 58 patients to prevent stress risers, but the decision to undergo removal depended on patients’ and their families’ preferences. In all, 24 patients in the SMP group and 23 in the FN group chose to undergo removal. Of these patients, two in the SMP group and seven in the FN group waited until experiencing soft-tissue irritation before agreeing to removal. In the SMP group, irritation was caused by the size of the plate and by the plate serving as a stress riser. In the FN group, irritation was caused by nail prominence at the entry points or distal ends. Irritation resolved after implant removal in all cases. Mean indwelling time was 197 days and was not significantly different between the SMP and FN groups (p = 0.19).
Surgical site infection developed in four patients in the SMP group (one after insertion and three after removal) and three patients in the FN group (two after insertion and one after removal). One patient who developed an infection after plate removal required inpatient admission, intravenous antibiotics and subsequent treatment with oral antibiotics. The other six infections resolved without sequela after outpatient antibiotic treatment. No evidence of avascular necrosis, heterotopic ossification, leg-length discrepancy > 2 cm, malunion or nonunion was identified.
Discussion
This was a retrospective study of 58 skeletally immature children without underlying musculoskeletal conditions who underwent operative treatment for a diaphyseal fracture with SMPs or FNs. With a mean clinical follow-up of 22 months and radiographic follow-up of 5.3 months, we found that treatment with FNs was associated with less EBL during insertion, shorter LOS after insertion and shorter operative times during insertion and removal procedures compared with SMPs.
Although studies have examined surgical parameters and outcomes in skeletally immature patients treated for femur fractures, we were able to identify only two studies that compared treatment with SMPs versus FNs. The first study, published in 2012, found that the insertion of SMPs was associated with significantly longer operative time (104 mins versus 94.7 mins, p = 0.095) and greater (but nonsignificantly so) EBL compared with FNs (220 mL versus 185 mL, p not reported) in 55 skeletally immature adolescents ≥ 11 years old with diaphyseal femur fractures. 20 A study published in 2016 compared postoperative outcomes in 198 skeletally immature patients eight years or older who underwent treatment with SMPs, FNs or rigid intramedullary nailing, and did not examine surgical parameters such as EBL or operative time. 21 Our study results are consistent with those of the 2012 study in terms of operative time and EBL 20 and with the 2016 study in terms of a higher incidence of irritation among patients treated with FNs (23% of 61 patients treated with FNs versus 2.9% of 35 patients treated with SMPs, p not reported). 21 Soft-tissue irritation has been reported as a complication of FNs in multiple studies, with incidence ranging from < 10% to as high as 52% 22 but is minor in most cases and relieved with implant removal.8,21,23–25 Proposed risk factors for irritation include bent or prominent nail ends, 22 earlier mobilization of the knee 12 and excessive nail protrusion at the time of implantation. Accordingly, studies have advocated immobilization, 23 leaving < 2.5 cm of nail protrusion, and minimizing bending the ends of the nails outside the bony cortex during insertion and trimming of the nails to help decrease soft-tissue irritation. 24
Notably, our study examines a younger cohort (ages four to 15 years) compared with the two previous studies comparing SMPs and FNs, which had age ranges of 11 to 17 years 20 and eight to 17 years. 21 This younger cohort may have different skeletal and healing characteristics compared with the older cohorts; the results of this study may therefore benefit surgeons considering these treatment options in a younger population.
Our finding of a longer LOS in the SMP group is unexpected because SMP is considered a stable fixation method. Possible explanations are greater pain and more difficult mobilization 26 with SMPs than with FNs, although further investigation is warranted.
A strength of this study is that all procedures were performed by one surgeon with substantial experience using both techniques. We explored the possibility of including multiple surgeons at the same centre, but decided to limit the study to a single surgeon to minimize variability. The disadvantages of a single-surgeon series, however, are a relatively small cohort and consequently limited statistical power, which may have prevented us from detecting differences in the incidence of infection or implant irritation. Additional studies are warranted to determine whether these differences exist. Another limitation is that blood loss was estimated rather than directly measured, but because this was performed consistently in all patients, we have no reason to believe that this would have led to a systematic bias.
In the present study, we observed a significant association between fracture type and treatment method, with more transverse fractures treated with FN and more comminuted fractures treated with SMP. The two existing studies comparing FN and SMP had the same limitation. Despite this association, a comparison of FN and SMP is nevertheless valuable because some fractures can be reasonably treated with either method, and there were indeed some comminuted fractures treated with FN and some transverse fractures treated with SMP in our cohort. Overall, the various fracture and patient factors that should inform implant choice and operative planning are still being determined.
In summary, treatment with FNs was associated with significantly shorter operative time, less blood loss and shorter postoperative hospitals stays compared with treatment with SMPs in 58 skeletally immature patients with diaphyseal femur fractures. These findings can assist with choosing an implant, especially when most or all other factors are similar. Although SMPs are more stable in length and rotation, the advantages of FNs, including less blood loss, shorter operative time and shorter LOS, should be considered. Importantly, further investigation with multicentre prospective studies and randomized control trials should be considered to further elucidate the advantages and disadvantages of each method in different clinical contexts.