
Abstract
Purpose
Progressive hip displacement is one of the most common orthopaedic pathologies in children with cerebral palsy (CP). Reconstructive hip surgery has become the standard treatment of care. Reported avascular necrosis (AVN) rates for hip reconstructive surgery in these patients vary widely in the literature. The purpose of this study is to identify the frequency and associated risk factors of AVN for reconstructive hip procedures.
Methods
A retrospective analysis was performed of 70 cases of reconstructive hip surgery in 47 children with CP, between 2009 and 2013. All 70 cases involved varus derotation osteotomy (VDRO), with 60% having combined VDRO and pelvic osteotomies (PO), and 21% requiring open reductions. Mean age at time of surgery was 8.82 years and 90% of patients were Gross Motor Function Classification System (GMFCS) 4 and 5. Radiographic dysplasia parameters were analysed at selected intervals, to a minimum of one year post-operatively. Severity of AVN was classified by Kruczynski's method. Bivar- iate statistical analysis was conducted using Chi-square test and Student's t-test.
Results
There were 19 (27%) noted cases of AVN, all radio- graphically identifiable within the first post-operative year. The majority of AVN cases (63%) were mild to moderate in severity. Pre-operative migration percentage (MP) (p = 0.0009) and post-operative change in MP (p = 0.002) were the most significant predictors of AVN. Other risk factors were: GMFCS level (p = 0.031), post-operative change in NSA (p = 0.02) and concomitant adductor tenotomy (0.028).
Conclusion
AVN was observed in 27% of patients. Severity of displacement correlates directly with AVN risk and we suggest that hip reconstruction, specifically VDRO, be performed early in the 'hip at risk' group to avoid this complication.
Keywords
Introduction
Progressive hip displacement is one of the most common orthopaedic pathologies in children with cerebral palsy (CP). The incidence and severity of hip displacement in CP is directly related to the degree of gross motor function. Using the Gross Motor Function Classification Score (GMFCS), Soo et al identified the incidence of hip displacement as 0% for children with GMFCS level 1 and 90% for those with GMFCS level 5. 1 A displaced hip can result in pain, reduced range of motion, skin breakdown, difficulty with perineal hygiene, difficulty with seating and positioning, and may contribute to the development of scoliosis and pelvic obliquity.2–5 Reconstructive surgery has become the standard of care in treating progressive subluxation and dislocation of the hip in this population.6–9 Reported complication rates for hip reconstructive surgery in patients with CP have varied dramatically (0% to 81%).8,10–18 There has been minimal attention paid to the development of avascular necrosis (AVN) as a complication of hip reconstructions. The incidence of AVN reported within the literature is in the range of 0% to 69%.10,11,14,15,17–20 This variation has made it difficult to quantify and determine the true impact of AVN on children with CP. Idiopathic AVN has been reported to cause pain, limited range of motion (ROM) and an altered gait pattern. 21 In children with developmental dysplasia of the hip (DDH), Roposch et al reported that there is a large variation in the clinical presentation of AVN. 21 Severe forms lead to hip pain and premature debilitating osteoarthritis, while mild forms may have minimal deformity and dysfunction. 21 The pathology itself and the clinical effects of AVN in children with CP have yet to be determined.
Diagnosis of AVN is based on radiographic images and clinical symptoms, which is a highly subjective process dependent upon the individual surgeon. There is currently no standardised, rigorous method for the objective diagnosis of AVN. Additionally, the quantification of pain and symptoms within the CP population is particularly challenging; therefore, the clinical relevance of AVN may be underestimated in these patients.
The purpose of this study is to identify the frequency and associated risk factors of AVN for reconstructive hip procedures in children with CP.
Patients and methods
A retrospective review was performed of children with CP surgically treated for hip subluxation at a single institution between 2009 and 2013. Further inclusion criteria were: patients aged 2 to 18 years; diagnosis of CP regardless of subtype; varus derotation osteotomy (VDRO) as the primary surgical treatment; and minimum follow-up of one year. Patients with insufficient follow-up, soft-tissue procedures only, salvage procedures or pre-operative evidence of AVN were excluded from the study.
All procedures were performed by one of two surgeons at our institution and consisted of VDRO with or without adjunctive procedures. These adjunctive procedures included adductor tenotomy, pelvic osteotomy and open reduction. When required, soft-tissue releases were completed first, followed by VDRO through a standard lateral, sub-vastus approach. A relative shortening of the femur was performed in all cases through the resection of a wedge of bone for the purpose of the VDRO, but this was not of standardised length. Dega osteotomy was the preferred pelvic osteotomy where performed. All open reductions were done through an anterior approach. While there was variability in method and duration of post-operative immobilisation, the majority of patients were placed in a Spica or Petrie cast for approximately four weeks followed by long-term splinting.
A detailed analysis of clinical and radiological data was performed on all children meeting the inclusion criteria prior to surgery, and post-operatively at six months, one year and two years.
Radiological evaluation was completed independently by two orthopaedic surgeons using standardised anteroposterior (AP) and frog-leg lateral radiographs of the pelvis. To determine concordance of radiographic diagnosis of AVN between our reviewers, inter-observer reliability calculations were performed. Across all radiographs included in the study at all time points, substantial agreement (Kappa = 0.76) was seen between our two reviewers. Specifically, at the one-year time point for AVN assessment, almost perfect agreement (Kappa = 0.86) was seen.
Radiographic parameters collected included: Reimer's migration percentage (MP), 23 acetabular index (AI), 24 Hilgenreiner's epiphyseal angle (HEA), 25 neck shaft angle (NSA) 26 and pelvic obliquity (PO). The presence and severity of AVN was evaluated according to Kruczynski's classification, a method relying on plain radiographs and combining previous works of AVN in DDH. 27
Frequency tables were constructed for all categorical variables and descriptive statistics were calculated for all measurement variables. A combination of Chi-square and two-sample t-tests were used to compare AVN with categorical and radiographic predictors. Confidence intervals for the difference in means were constructed for all measurement predictors.
Results
We reviewed all cases of reconstructive hip surgery over a four-year period at our institution, where VDRO was the primary procedure in patients with CP. After eliminating patients with insufficient follow-up and 11 cases of pre- morbid AVN, there were 70 reconstructive hip surgeries in 47 patients available for final analysis (Fig. 1).
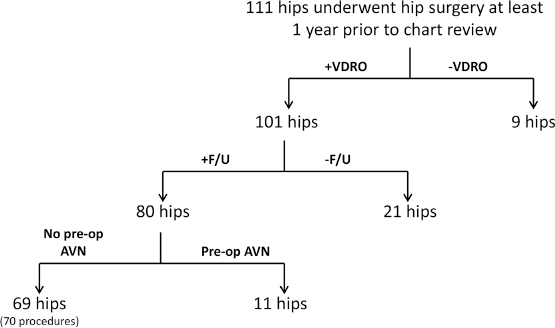
All hips in CP patients undergoing surgery at a single institution between 2009 and 2013. Included hips underwent a varus derotation osteotomy (VDRO), with at least one year of post-operative follow-up with no evidence of pre-operative avascular necrosis.
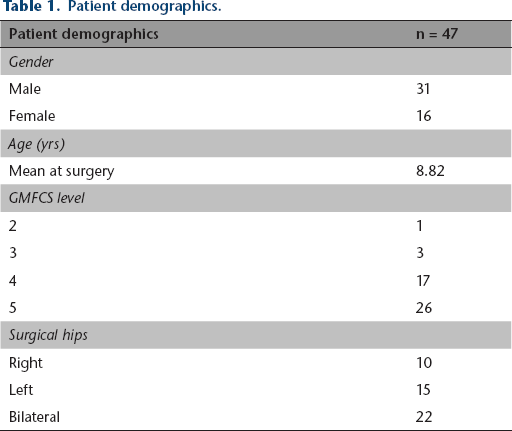
Pre-operative patient demographics are shown in Table 1. The 31 patients were male and 16 patients were female. There were ten unilateral right hips, 15 unilateral left hips, 22 bilateral cases and one revision procedure. The mean age at time of surgery was 8.82 years (3.02 to 17.3). In total, 43 of the children (91%) were GMFCS levels and 5. Given the universal lack of consensus diagnosing topographic subtype of CP we intentionally did not report or analyse this factor.
Patient demographics.
In addition to a VDRO, Dega osteotomy was performed in 60% (42 hips) of the cases, 21% (15 hips) required open reductions, and 70% (49 hips) had adductor releases. Of note, many of these patients had previous isolated adductor releases therefore explaining why it was not performed in all cases as an adjunct. Only a few hips (n = 14) required comprehensive reconstructions requiring all of the above. The mean post-operative follow-up was 2.73 years (1.0 to 6.72).
The mean pre-operative Reimer's MP of our entire cohort measured 60%. This improved radiographically to an average MP of 11%, at six-month post-operative follow-up. The mean pre-operative AI was 32.4° and was corrected by an average of 8.9° to 23.7° at the same follow-up. This improvement in AI was influenced by a concomitant pelvic osteotomy. AI improved by an average of 14.8° (95% confidence interval (CI) 11.3 to 18.3) in hips that also underwent a pelvic osteotomy compared with 0.6° (95% CI -1.4 to 2.6) in hips that did not. NSA averaged 155° pre-operatively and was corrected to 116°. HEA changed from a mean pre-operative 10° to 53°. Pelvic obliquity remained relatively unchanged after hip reconstruction.
A total of 19 (27%) hips were identified to have radiographic signs of AVN, all occurring within the first post-operative year. All but one case of AVN was present in patients with GMFCS 4 or 5. There were three GMFCS 5 patients with bilateral AVN after bilateral hip procedures involving VDRO and adductor releases.
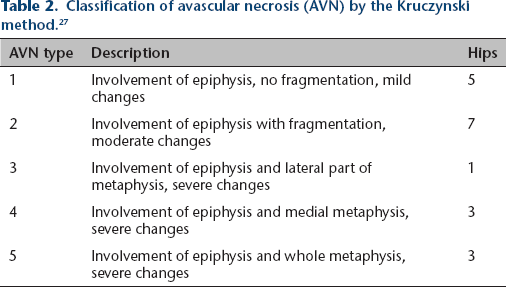
The severity of AVN was evaluated using a classification described by Kruczynski in 1987 (Table 2). 27 The majority of the identified cases (63%) of AVN had mild-to-moderate epiphyseal changes only. At the two-year follow-up, eight cases showed radiographic evidence of healing, while 11 cases of AVN persisted at last follow-up. Examples of AVN of varying severity and resolution from this patient cohort are shown in Figure 2.
Classification of avascular necrosis (AVN) by the Kruczynski method. 27
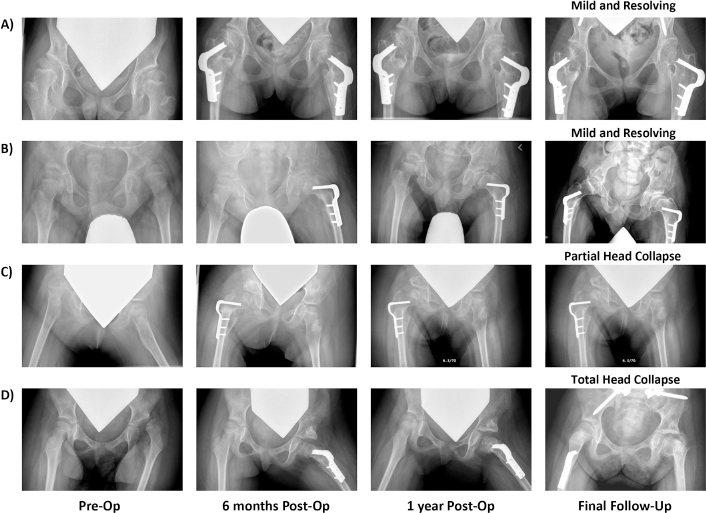
Examples of radiographic avascular necrosis (AVN) progression following varus derotation osteotomy (VDRO), depicting (
Risk factors showing a statistically significant correlation with the development of AVN included: higher pre-operative Reimer's MP (p = 0.0009); larger immediate change in MP (p = 0.002) and NSA (p = 0.02) (Table 3); and concomitant adductor tenotomy (p = 0.028) (Table 4). Additionally, a higher pre-operative NSA was suggestive of AVN development, but did not reach statistical significance (p = 0.079).
Comparison of presence of avascular necrosis (AVN) with respect to measurement predictors.
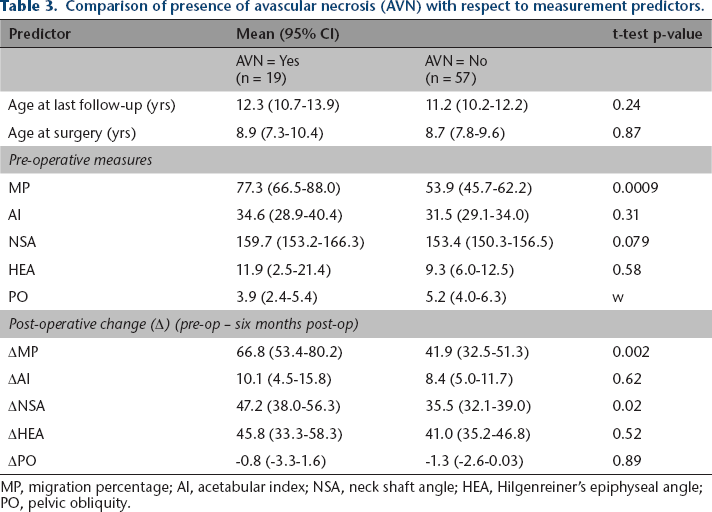
MP, migration percentage; AI, acetabular index; NSA, neck shaft angle; HEA, Hilgenreiner's epiphyseal angle; PO, pelvic obliquity.
Comparison of presence of avascular necrosis (AVN) with respect to categorical predictors.
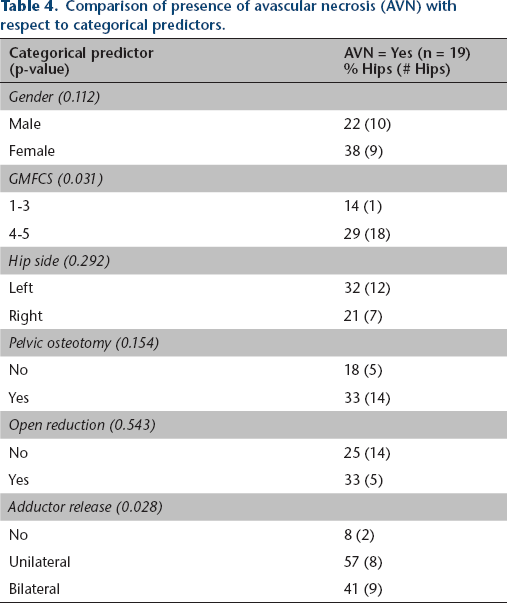
There was also evidence of a relationship between higher GMFCS level and development of AVN when comparing patients at levels 1 to 3 with patients at levels 4 to (p = 0.031); however, when comparing only level 4 with level 5 patients, this did not reach significance (p = 0.052).
There was no relationship between AVN and sex, affected side, concomitant pelvic osteotomy, open reduction or any other soft-tissue procedures (Table 3).
Other noted complications included: three fragility fractures (4.3%); three pressure sores (4.3%); and one infection (1.4%). There was one hip with a recurrent subluxation requiring re-operation.
Discussion
The reported incidence of AVN of the femoral head in children with CP after hip reconstruction is in the range of 0% to 69%.10,11,13,18,20,28–30 A recent systematic review 31 on the subject revealed that most authors simply comment on the presence or absence of AVN in their complications, without further detail. Interestingly, the reported rates in our study as well as three others where AVN was the primary outcome measure are among the highest within the literature at 27% to 69%.10,11,18 Koch et al reported an incidence of 68.7%, Stasikelis 46% and Khalife 37%.
There are no universally accepted criteria for diagnosing AVN, nor is the underlying mechanism fully understood. Therefore, making the diagnosis of AVN can be challenging and requires subjective judgment. This is made more difficult in CP where it is common to see irregular femoral head geometry, 11 flattening from chronic subluxation, 7 decreased bone density particularly in non-ambulatory patients and iatrogenic deformities such as coxa vara from surgical treatments. The literature does not suggest that any efforts have been made to create a separate diagnostic or classification system for AVN in children with CP. The most commonly used systems, including Bucholz and Ogden, 32 Kalmachi and MacEwen, 33 and the lesser known Kruczynski 27 classification, have been extrapolated from DDH literature. These classification systems all pose the same limitations of being based on plain radiography versus MRI, possible poor inter- and intra-observer reliability because of subjective interpretation, failure to provide information about mechanism/aetiology, difficulty interpreting the clinical significance and prognosis, lack of correlation with long-term outcome and lack of validation in children with CP. This points to the necessity of a standardised diagnostic and classification criteria for AVN of the femoral head in CP, as this deficiency has surely contributed to the wide variability in reported incidence.
Osteonecrosis of the femoral head is a progressive process due to multiple factors affecting the blood supply of the femoral head and the disruption of the synthesis of the bone component. 34 Two commonly proposed mechanisms of femoral head ischemia are extrinsic blood vessel compression/injury and excessive pressure on the femoral head, both of which prevent perfusion. 35 Despite the unclear mechanisms contributing to collapse, factors affecting bone necrosis have been found to be related to significant biomechanical changes and physical stress in the load-bearing area of the femoral head. 36
As it was not the purpose of this study to determine causation, we can only speculate regarding aetiology. It is, however, a reasonable hypothesis that surgically reducing a severely displaced hip could produce compression of the femoral head itself or its blood supply, especially in the setting of inadequate femoral shortening. We cannot exclude surgical technique as a cause, but were unable to compare surgeon-specific rates of AVN in our cohort because of the small percentage (13%) of procedures performed by one of the two surgeons.
An essential element in making the diagnosis of AVN is allowing passage of sufficient time for changes to manifest on a radiograph. This was a retrospective review and while our average follow-up was 2.73 years, we had a number of rapidly evolving cases of AVN, which is in conflict with the previously proposed diagnostic criteria of Salter, 37 where a minimum of one year is required to diagnose AVN. These cases could represent a pseudo-osteonecrosis state with transient epiphyseal mechanical deformation or growth modulation post reduction, but this cannot be confirmed within the confines and limitations of this retrospective study As of yet, we do not have any terminology or nomenclature to distinguish this process from AVN.
There were several, further limitations to this study. First, AVN is inherently a subjective outcome measure that may be impacted by timing and radiograph positioning. A lack of rigorous, standardised positioning for routine AP radiographs may have interfered with the interpretation. However, we mitigated this subjectivity by having two independent reviewers rate each radiograph included in the study and they demonstrated substantial to near-perfect agreement. Second, being retrospective in nature, we were prevented from establishing the long-term clinical, functional or health-related significance of AVN as a complication of hip reconstruction. The majority of our cases of AVN were of mild and moderate severity, as classified by Kruczynski. 27 Previous authors have reported that limited involvement of the epiphysis alone results in minimal deformity and little long-term dysfunction.32,33,38,-40 Koch et al 11 noted a strong correlation between post-operative pain and the severity of the grade of AVN following hip reconstructions in CP. However, quantification of pain and disability in children with CP is a controversial topic and there is a paucity of literature on quality of life related to AVN following hip reconstruction.
We have identified pre-operative risk factors for the development of AVN as higher Reimer's MP, VDRO performed with concomitant adductor tenotomy, and larger operative corrections in MP and NSA, all of which highlight the chronicity and severity of hip displacement. We further witnessed an increased incidence of AVN in children of higher GMFCS levels, which is consistent with existing literature correlating worsening hip dysplasia and prognosis in children with higher GMFCS levels.19,41–43
We had a mixed group of CP subtypes and intentionally did not analyse this as a separate factor. Several studies have shown that GMFCS levels are more correlated to hip displacement than topographic CP subtype. Thus, our results were not likely affected by this variable. 44
We conclude that the severity of hip displacement correlates directly with the risk of AVN - a theory which is supported by Koch et al. 11 We have shown that severity of dislocation, as determined by MP, is the most significant predictor of AVN following hip reconstruction in CP. The same risk factor was identified as being significant by Khalife et al 10 in their group of 89 neuromuscular hips undergoing femoral varus osteotomy. Their group also found older age to be a risk factor, which we did not replicate. Stasikelis et al 18 found that the only risk factor was concomitant pelvic osteotomy in their group of 94 VDROs. Koch et al 11 has the highest published incidence of AVN, 68.7%, in a group of GMFCS 4 and 5 children with dislocated hips, all of which underwent open reductions, femoral and pelvic osteotomy. While our cohort had a spectrum of hip displacement, open reduction did not appear to be a risk factor for AVN.
Our findings support proponents of early intervention in the 'hip at risk' group to prevent poor outcome.3,4 In fact, our data would suggest that a delay in hip reconstruction beyond a Reimer's MP of 65% is associated with a higher rate of post-operative AVN. Therefore, we recommend in cases of progressive hip displacement that reconstructive procedures be performed within a safe range, namely a Reimer's MP of 40% to 60%, to avoid AVN of the femoral head. We appreciate, however, that the clinical significance of developing AVN and the subsequent impact on the quality of life of patients with CP remains uncertain and warrants further study.
There is significant variability in the reported incidence of AVN of the femoral head after hip reconstructions in CP. While this could be a result of the heterogeneity of studies, it is surely confounded by the lack of a systematic identification process of AVN in these patients. Our incidence of 27% is similar to the higher reported rates in other studies looking at AVN as a primary outcome. We conclude that the severity of hip displacement correlates directly with the risk of AVN and suggest that hip reconstruction, specifically VDRO, be performed early in the 'hip at risk' group to avoid this potentially devastating complication. There is a need for large group prospective data on this subject in order to identify true predictors of AVN and its relationship to quality of life.
Footnotes
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
No funding was received for this study.
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
As a retrospective study, a waiver of informed consent was approved by the institutions ethical review board.
KM has received research grants from the International Hip Dysplasia Institute, Pega Medical, Depuy (Johnson & Johnson) and Allergan. None are specific to this study. LP, KH, ES, JA and JF declare no conflicts of interest.