
Abstract
Purpose:
To establish the rate of avascular necrosis after hip reconstruction surgery in children with cerebral palsy and to identify risk factors that influence the development of avascular necrosis in this population.
Methods:
An institutional review board–approved retrospective review was conducted on children with cerebral palsy who underwent hip containment surgery at a single institution. Radiographs were evaluated at three time points. The Reimer’s migration percentage, neck shaft angle, epiphyseal shaft angle, acetabular index, center edge angle, and acetabular angle were measured. The presence of avascular necrosis was evaluated and graded by the Bucholz/Ogden and the Kalamchi/MacEwen classification systems. Multivariate logistic regression was performed to identify risk factors associated with the development of avascular necrosis.
Results:
A total of 154 children with cerebral palsy underwent hip containment surgery on 223 hips. Twenty-nine children (18.8%) underwent both pelvic and femoral procedures; 36 children (23.4%) had only femoral procedures; 47 children (30.5%) had femoral and soft tissue; and 42 children (27.3%) had pelvic, femoral, and soft tissue procedures. Using the Bucholz and Ogden or the Kalamchi classifications, the rate of avascular necrosis was 24.7% (38/154). Of the variables evaluated, preoperative Reimers was found to be significant predictors of avascular necrosis. The rate of avascular necrosis was 26.7% for Gross Motor Functional Classification System level III, 24.1% for Gross Motor Functional Classification System level IV, and 27.3% for Gross Motor Functional Classification System level V.
Conclusion:
The overall rate of avascular necrosis in children undergoing hip containment surgery was 26.7%. Together, age at surgery, open reduction, previous surgery, preoperative Reimers, and estimated blood loss contributed to the development of postoperative avascular necrosis; however, only preoperative Reimers significantly contributed to the development of avascular necrosis in children with cerebral palsy undergoing hip containment procedures.
Introduction
Cerebral palsy (CP) affects nearly 3 out of every 1000 of American children. 1 Despite CP being a non-progressive disorder, many musculoskeletal conditions may manifest during skeletal growth and development. Hip dysplasia is very common among this population, and its severity is directly related to the Gross Motor Functional Classification System (GMFCS). Up to 90% of children with GMFCS level V have been shown to develop hip migration > 30%. 2 A displaced hip often requires containment surgery when there is progressive subluxation, as a neglected hip can cause pain, difficulty with perineal hygiene, sitting and positioning, and reduced hip range of motion, and may contribute to the development of pelvic obliquity and scoliosis. 3
Reconstructive surgery often involves a variety of procedures including combinations of varus derotational osteotomies (VDRO), shortening of the femur, pelvic osteotomies, as well as open reduction and/or soft tissue releases. Long-term results following these procedures have been considered successful in most cases; however, they are not without complications. Subluxation, dislocation, infection, fracture, hardware failure, and avascular necrosis (AVN) can all occur.4–7 Of these orthopedic complications, AVN has received little attention in literature until recently.5–8 Generally, posthip reconstruction femoral head AVN is not seen in the early postoperative period but can lead to the development of accelerated osteoarthritis. 5 This can lead to significant pain, leaving limited options for treatment in children with CP. 9
Outcomes of surgical intervention in children with CP have been reported with high rates of AVN of the femoral head. A recent review of publications cited AVN rates of 0%–46%, with rates being higher in studies where it was the main outcome. 5 The primary purpose of this study is to establish the rate of AVN after hip reconstruction in children with CP based on the type of surgery performed. Our secondary objective of this study was to identify any independent risk factors that influence the development of AVN, in order to help counsel families on the non-modifiable risk factors and to guide surgical treatment if there are any modifiable risk factors.
Methods
An institutional review board–approved retrospective review was conducted on children with CP who underwent hip reconstruction procedures at a single institution between 1991 and 2016. We set out to determine if AVN was present and to determine the presence of factors related to the development of AVN. The medical record was searched for multiple demographic and clinical parameters including the diagnosis of CP, GMFCS level, age, sex, race, procedure type, revision surgeries or surgeries for hardware removal, and any documented complications. All children with CP with neuromuscular hip dysplasia who underwent surgical reconstruction to stabilize a migrating hip or to relocate a dislocated hip were included in the analysis. Children were excluded if they had soft tissue procedures only, follow-up was <1 year, insufficient records or images, or underwent salvage procedures for a neglected hip unrelated to AVN. Adjunctive procedures included pelvic osteotomy, soft tissue release (hamstring, adductors, iliopsoas) and open reduction.
Radiographic parameters were measured to quantify the level of severity of disease by measuring the amount of hip and pelvic dysplasia. Preoperative, immediate postoperative, and the most recent pelvis or hip radiographs were evaluated. The Reimer’s migration percentage, neck shaft angle, epiphyseal shaft angle, acetabular index, center edge angle, and acetabular angle were measured and recorded for each time point by one North American pediatric orthopedic fellow and one Australian orthopedic surgeon. The radiographs evaluated were digital images in a local picture archiving and communication system (PACS) system or scanned images of printed radiographs prior to the use of PACS. The Image J program (National Institutes of Health free software: https://imagej.nih.gov/ij/index.html) with Object J as an add-on plugin was used to perform the measurements on each image. De-identified final images from the most recent follow-up for each child were evaluated for AVN by three fellowship-trained pediatric orthopedic surgeons, with a mean of 24 years of experience. If AVN was present, it was assigned a grade or stage based on the Bucholz/Ogden classification and the Kalamchi/MacEwen classification. Both classification schemes were printed and available during the grading process. When there was a disagreement on the AVN grading between surgeons, a consensus was obtained from all three graders. We defined AVN as any rating of AVN from either classification. All children who developed AVN were further analyzed to identify possible independent risk factors.
To maintain statistical independence (as one hip outcome may affect the other) and to avoid falsely inflating the number of subjects, only one hip was evaluated for each child for our primary analysis. When both hips were operated on, the hip with the more severe Reimers migration percentage was analyzed. 10 Statistical analysis was performed using Statistical Product and Service Solutions (SPSS) (IBM SPSS Statistics v. 27). Intraclass correlation coefficients (ICCs) model (2,1) was used to assess the degree of correspondence and agreement the assignment of grades by the surgeons for the Bucholz and Kalamchi /MacEwen classifications. For this study, we considered ICCs below .75 to be poor to fair, while ICCs between .75 and .90 were considered good and above .90 considered excellent. 11 The Fleiss Kappa statistic was used to determine the proportion of agreement between evaluators once chance was removed. Percentages were used to compare the number of children who had previous surgeries, the type of procedures received, and GMFCS level. Chi-square was used to determine whether there is a relationship between subjects who had a previous surgery or open reduction and the development of AVN. Logistic regression was used to examine whether patient and surgical variables (estimated blood loss (EBL), GMFCS level, age at surgery, and Reimers Migration percentage) significantly predicted the development of AVN. Surgical variables were chosen a priori. Statistical significance was set at p < .05.
Results
To identify AVN, we used both the Bucholz and Kalamchi AVN classification systems. We used the Kappa statistic to assess agreement which revealed slight to fair (Kappa range = .187–.249) agreement for the Bucholz and Kalamchi classifications (Table 1). Interclass correlations were calculated for all hips by side, and classification system revealed that the three evaluators had poor to fair ICCs ranging from a low of ICC = .354 to a high of ICC = .577. ICCs were lower for the Bucholz than the Kalamchi classification. Because of the discrepancy noted during the initial rating of AVN by the individual raters, a re-evaluation was performed and the consensus grading was used for the final analysis to define the rate of AVN.
ICC values for AVN classifications (Bucholz and Kalamchi).
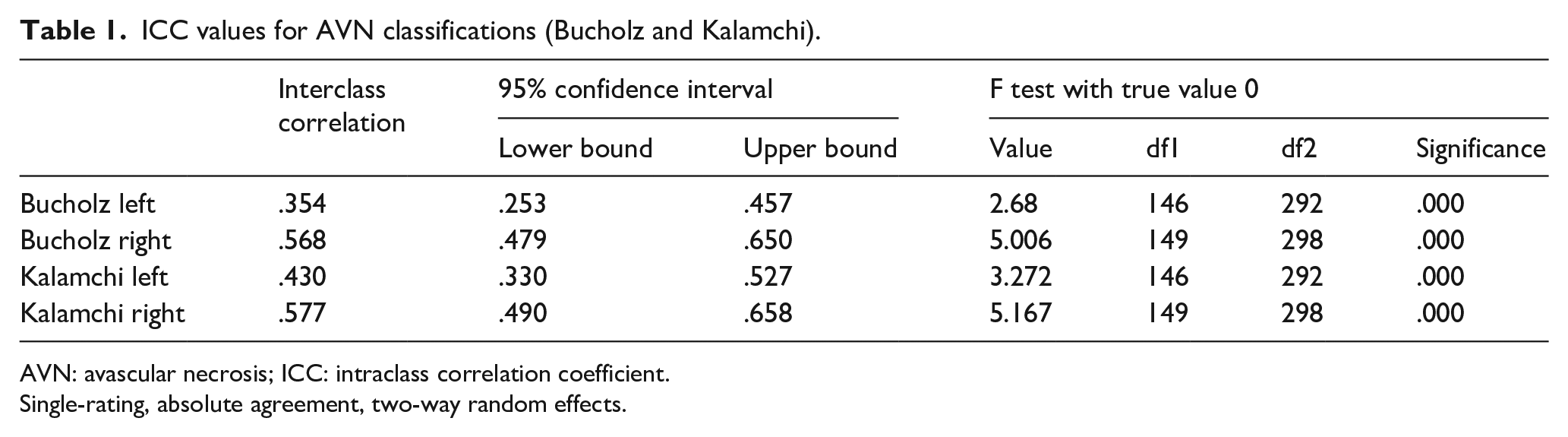
AVN: avascular necrosis; ICC: intraclass correlation coefficient.
Single-rating, absolute agreement, two-way random effects.
A total of 154 children had surgery on 223 hips. Mean follow-up was 5.3 years (SD =3.5 years) after surgery. In all, 38 children (24.7%) developed AVN and 116 (75.3%) did not (Table 2). Of the 38 children who developed AVN, 33 (86.8%) had unilateral AVN and 5 children (13.2%) developed bilateral AVN. We also calculated the rate of AVN by hip and found that in the 223 hips that were operated on, using the Bucholz AVN grading system, 43 hips (19.3%) developed AVN, whereas using the Kalamchi system, 42 hips (18.8%) were determined to develop AVN.
Number of children with AVN by surgery type.
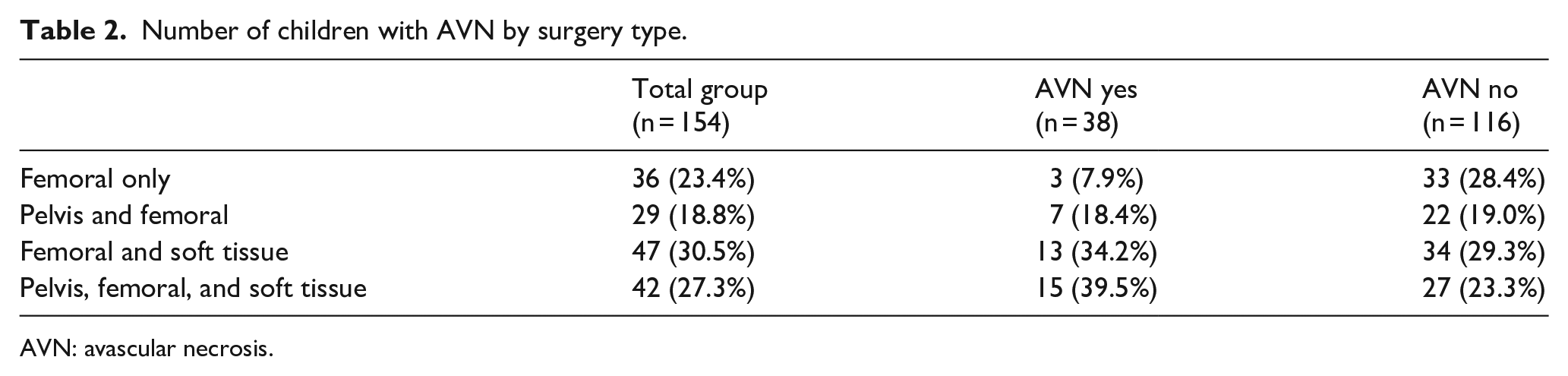
AVN: avascular necrosis.
The age at surgery was not statistically different between the groups (p = .253); however, the length of follow-up was different (p = .017) (Table 3). The AVN group had a mean follow-up of 6.5 years (range: 1–16.4 years, median = 5.7 years), whereas the group without AVN had a follow-up of 4.9 years (range: 1–17 years, median = 4.2 years), suggesting that with longer follow-up, more AVN may be discovered. Children are typically followed both clinically and radiographically till skeletal maturity.
Demographic and clinical variables and relationship to the development of AVN.
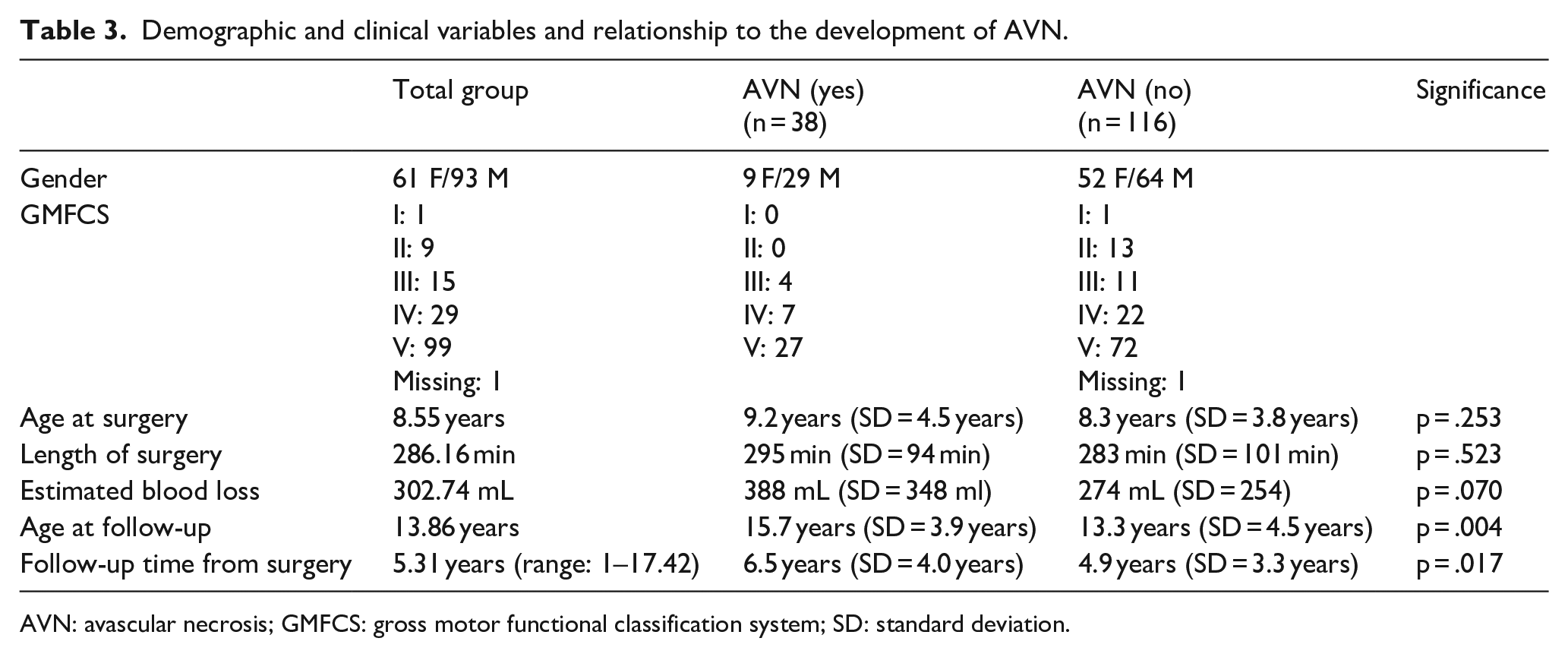
AVN: avascular necrosis; GMFCS: gross motor functional classification system; SD: standard deviation.
A logistic regression analysis was conducted to evaluate the relationships between the likelihood of developing AVN and the predictor variables of EBL, previous surgery, open reduction, age at surgery, and preoperative Reimer’s migration percentage. Together, the five predictors significantly predicted the development of AVN, χ2(5) = 11.61, p = .04; however, only preoperative Reimers significantly contributed to the equation, p = .02. For every 1% increase in migration percentage, the odds of developing AVN increase by a factor of 1.020 (Table 4). The mean blood loss of the children that developed AVN was not statistically significantly higher than those who did not, 388 versus 274 mL, p = 0.07. While a greater number of children in GMFCS level V required hip containment surgery (99 total), the rate of AVN was not significantly different between children at GMFCS levels III (26.7%), IV (24.1%), or V (27.3%).
Significance of independent risk factors.
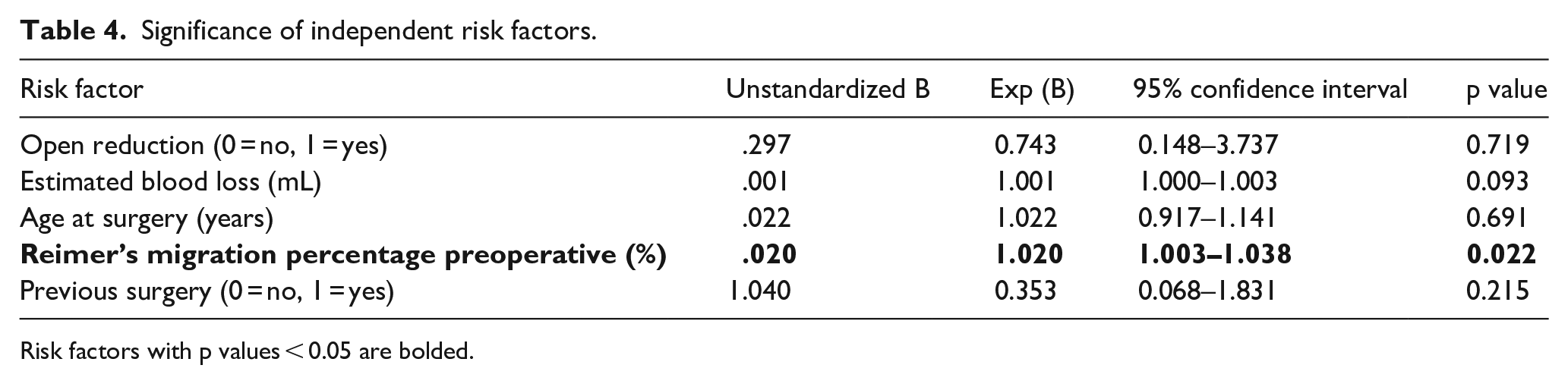
Risk factors with p values < 0.05 are bolded.
All the children in the study had a femoral procedure performed. Of the 38 children who developed AVN, 7 (18.4%) had a concomitant pelvic procedure performed, while 15 (39.5%) had both pelvic and soft tissue procedures. There was no significant difference between children who had open reduction and the development of AVN, χ2 = .386, p = .535. Similarly, there was no significant difference between children who had a previous surgery and the development of AVN, χ2 = 1.15, p = .284.
Based on radiographic analysis, the Reimer migration percentage for both hips was ≤40% for 141 of 153 (92.21%) children at immediate postoperative (1 child unable to be evaluated) (Table 5). At long-term follow-up, an additional 4 children’s images were unavailable for analysis, and 134 of 150 (89.3%) remained reduced. Preoperative, postoperative, and long-term follow-up Reimer’s migration percentage, neck shaft angle, epiphyseal shaft angle, acetabular index, center edge angle, and acetabular angle are reported in Table 2. Change in Reimers from preoperative to postoperative correlated with the development of AVN (r = .178, p = .03).
Radiographic measurements and relationship to the development of AVN.
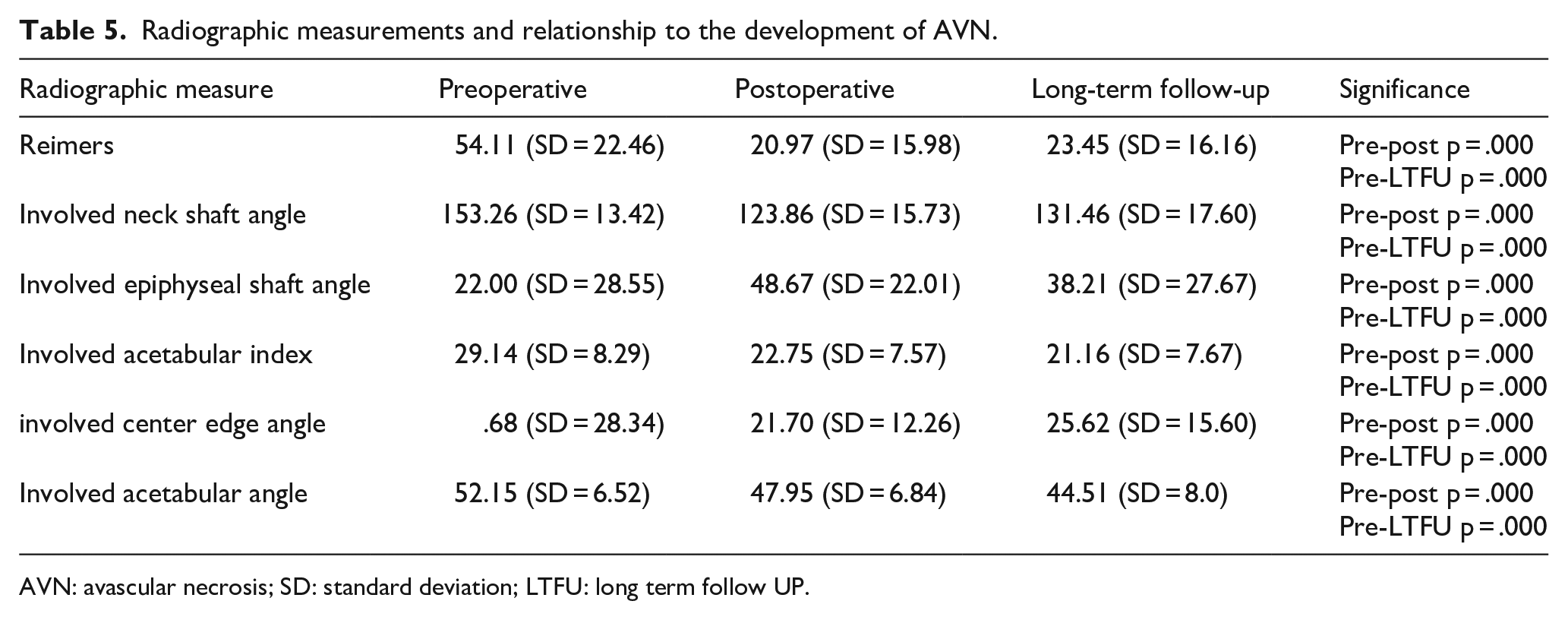
AVN: avascular necrosis; SD: standard deviation; LTFU: long term follow UP.
Discussion
AVN of the femoral head epiphysis is a potentially severe complication of the treatment of developmental dysplasia of the hip. Until recent years, there has been little information about AVN in the treatment of hip dysplasia associated with CP. The published rates of AVN in this population vary widely from 0% to 75%.4–8,12 The purpose of this study was to identify the rate of AVN in children with CP who underwent hip reconstruction for hip dysplasia at a single institution. A secondary goal was to identify any potential risk factors associated with developing AVN in this group of children.
In this study, we found that the overall rate of AVN in children with CP undergoing hip containment surgeries was 24.7% (38/154). This is in range with the currently published data.4–8,12 Thirty-three children developed unilateral AVN and 5 children developed bilateral AVN. All 38 hips that developed AVN had femoral procedures performed, whereas 7 of 38 (18.4%) had pelvic procedures as well. Because we evaluated the rate of AVN by child, it only included one hip of each child that developed bilateral AVN.
Several variables were evaluated to determine risk factors for developing AVN in this population (EBL, open reduction, Age, Reimers Migration, and prior surgery). While more children with GMFCS level V required a hip containment procedure, the rate of AVN development was similar for GMFCS levels III, IV, and V. While the unstandardized beta value was low, higher Reimers migration percentage was found to be a predictable risk factor in developing AVN, with children who developed AVN having a significantly greater (61.3 vs 51.1) Reimers migration percentage. This could be a result of the increasing severity leading to a more technically demanding surgery as well as perhaps more stretch or injury to the blood supply of the hip with reduction.
In reviewing the literature, other studies have been performed in order to identify the rate of AVN in children with CP who had hip containment surgery.4–8,12 Some of those studies have small patient cohorts. Our current study has one of the largest patient population of such studies, including 154 children. In addition, to our knowledge, no other study has used both the Bucholz/Ogden and the Kalamchi/MacEwen classification systems to assess postoperative development of AVN. Most studies use only one classification system to rate AVN, and one study did not use any classification system to grade AVN but rather used surgeon experience to determine if AVN was present or not. 8
A retrospective review of children with CP who underwent hip reconstruction for dysplasia involved 81 children. 6 To be included in their analysis, children required a hip migration > 80% and follow-up >1 year. All children underwent open hip reduction, combined with proximal femoral and Dega osteotomies. The primary outcome was to evaluate the incidence of AVN in this subgroup of children. They reported signs of AVN in 68.7% (79/115) of the hips in their study. When classified using the Kruczynski modification of the Kalamchi/MacEwen classification, they found that most hips had minor involvement while 18% (23/115) had more severe involvement (Grades III–V). 6 This rate of AVN is much higher than the rate found in the current study, which may be due to their strict inclusion criteria which included only those children with hip migration percentage > 80%.
In a recent review of the literature on AVN in the CP population, the authors reported that the frequency of AVN ranged from 0% to 46%. 5 Twenty-nine studies that commented on the presence or absence of AVN and had more than 12 months of follow-up were included in the analysis. Seventeen of the studies reported a rate of AVN of 0%. Four studies reported an AVN rate of >20%. The overall rate of AVN among the 1424 hips in the combined analysis was 7.5% (107/1424). Only two studies recorded AVN as the primary outcome measure. In these studies, the rate of AVN was found to be much higher than the rest at 37% and 46%. Based on their findings, the authors suggest that the true frequency and severity of AVN after hip reconstruction in CP are generally poorly reported and may be higher than is currently understood. 5
Another recent retrospective analysis was conducted in 47 children with CP. 7 They performed 70 VDROs with 60% having a combined pelvic acetabuloplasty. All had a minimum of 12 months postoperative follow-up. Kruczynski’s modification of the Kalamchi and MacEwan classification was used to grade AVN in their cohort. Twenty-seven percent (19/70 hips) were noted to have AVN. Most of the cases of AVN were classified as mild to moderate. They found that preoperative migration percentage, postoperative change in migration percentage, GMFCS level, change in neck shaft angle, and concomitant adductor tenotomy were found to be statistically significant risk factors in developing AVN. Of these, the preoperative migration percentage and the change in migration percentage were found to be the most significant predictors of AVN. To conclude, the authors recommended performing VDRO early in the “hip at risk” as the severity of hip displacement correlated directly with the risk of AVN.
One of the studies that most closely matches the size of our study recently reported a much lower rate of AVN at 3%. 13 This was the rate of AVN of each hip, and not that of the child. It is not clear if there were any cases of bilateral AVN in their study, so the rate of AVN per child cannot directly be made but would be likely >3%, yet significantly less than our rate. The follow-up in their study was slightly less than the current study (3.2 vs 4.5 years) and included more children with isolated acetabular surgery than our cohort. In their cohort, they found a relationship of AVN with open reduction, while we found no difference. This could be due to the smaller number of children with AVN in their group (n = 11) which may not have been adequately powered to clearly define a relationship.
There are several potential limitations to this study. It was retrospective in nature and incurs the limitations with such a study design. Some of the radiographic measures were difficult to obtain and limited by image quality. Images from earlier years printed on film may have been more difficult to measure and evaluate thus leading to potential bias. Some errors may have occurred during the measurement process; however, the sample size was large and the number of radiographs that were difficult to measure was low. While the children who were excluded for inadequate radiographs could influence the overall rate of AVN, the total number excluded for inadequate radiographs or salvage procedures was low. Furthermore, there is no established femoral head AVN grading system for use in children with CP. While not designed to evaluate AVN in CP, both the Bucholz/Ogden and Kalamchi/MacEwen have been used in multiple studies to determine the presence of AVN. These classification systems were established for use in patients with developmental dysplasia of the hip (DDH), and patients with neuromuscular conditions were excluded from analysis in the original descriptions of these systems.12,14–16 The inter-rater reliability of the Bucholz/Ogden classification in DDH has been found to be low at .34, which is similar to our findings.
AVN secondary to surgical procedures on the neuromuscular hip may manifest in ways different to those categorized by these systems, so the actual incidence of AVN may be misrepresented based on the limits of the classification systems used in this study. Valgus angulation is integral to the natural history of neuromuscular hip dysplasia. Such valgus angulation can be difficult to distinguish from the valgus deformity secondary to AVN as classified by Bucholz and Ogden as type II, or Kalamchi and MacEwan type III. Likewise, significant postoperative varus may be confused with type IV AVN in both classification systems. While the ICC values of intra-observer reliability were good, the interobserver correlation values among three experienced surgeons were poor, demonstrating the difficulty with this classification system. In our review of the radiographs, any hip that met criteria for either of the classifications was marked has having AVN even if it may have been due to the natural history. This would lead to us overreporting the rate of AVN. However, the rate of AVN by either system was quite similar, leading us to believe that both systems are able to detect femoral head changes at the same rate. Due to these limitations of the current grading schemes for hip AVN, a new AVN classification system specific for AVN in children with CP may be beneficial. It is possible that a more functional grading scale, such as the Melbourne Cerebral Palsy Hip Classification System would be a more appropriate radiographic outcome than a classification of AVN. 17 In addition, we do not have patient-reported outcomes for these children, so it is difficult to know what significance the finding of AVN would have on the child. While it is standard practice for us to collect patient-reported outcome scores, it was not consistently recorded during the study period. Pain, hygiene, standing, and sitting ability are all important determinants of quality of life and were not elucidated in this study, though they have been shown to improve after hip reconstruction. 18
Conclusion
The rate of AVN in a large population of children with CP that underwent hip containment surgery was 24.7%. With current AVN classification systems, it is difficult to distinguish between AVN and natural hip deformities that occur in CP. Because a larger preoperative Reimers migration percentage was associated with a higher rate of AVN, continued efforts to detect hip dysplasia and intervene earlier are warranted. Further studies to determine the clinical implications of AVN will be important as well as a clinically relevant radiographic AVN classification specific to children with CP.
Footnotes
Author contributions
Compliance with ethical standards
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of XXXX (number 00017164) on 2 May 2017, with an exemption from informed consent. No specific consent is needed for statistical analyses of aggregated de-identified data. For this study, the raw data were first extracted from HIS, and patients’ identities, including names, screening IDs, patient IDs, and mobile phone numbers, were de-identified.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.