
Abstract
Purpose:
This report presents the long-term results of the hip joint reconstruction in patients with spastic hip disease through open reduction, proximal femur varus derotation osteotomy, and Dega transiliac osteotomy.
Methods:
We analyzed retrospectively patients diagnosed with a spastic form of bilateral cerebral palsy with painful hip subluxation or dislocation. All patients underwent the same surgical procedure. The minimum follow-up time was 15 years. The study group comprised 15 patients (22 hips), classified with the Gross Motor Function Classification System as levels IV and V. The hip joint range of motion and anteroposterior X-ray examination at the final follow-up visit were compared with pre-operative data. The pain level was evaluated using the Visual Analogue Scale (VAS), and the femoral head shape was assessed using the Rutz classification. The patients’ caregivers answered questions regarding pain during sitting, personal hygiene activities, and at rest. The caregivers’ satisfaction with the treatment was also assessed with the Caregiver Priorities and Child Health Index of Life with Disabilities questionnaire.
Results:
We observed a significant reduction of the hip joint pain and improvement in both radiological hip stability parameters and range of motion at the final follow-up visit. Based on the Rutz classification, one hip remained type B, while the other joints became type A. Reduced pain was reported in all three positions, with the most pronounced improvement during sitting and personal hygiene activities. Interestingly, patients with unilateral hip reconstruction were more prone to pain after reconstruction than those operated bilaterally.
Conclusion:
Primary reconstruction of the painful hip joint neurogenic dislocation results in a stable joint reduction, pain decrease, and improved quality of life in patients with cerebral palsy.
Level of evidence:
IV case series.
Introduction
Spastic hip disease (SHD) comprises pathologic changes within the hip joint caused by disturbed muscle balance that lead to acetabular defect and hip joint displacement. 1 The incidence of hip joint dislocation ranges from 1% to 75% and is related to the Gross Motor Function Classification System (GMFCS).2 –4 Untreated progressive hip displacement negatively impacts the child’s health-related quality of life (HRQOL). Namely, it may cause pain and difficulty in caregiving, including dressing and perineal hygiene, especially in non-ambulatory children. 5 This hip joint pain may progress in adult life, becoming one of the most debilitating and most frequently reported problems. 6
Therefore, to reduce the risk of neurogenic hip pain, systematic, reliable radiographic evaluation of the hips at risk with early surgical intervention is necessary.7,8 It has been well established that the neurogenic hip reconstruction with femur varus derotational osteotomy (VDRO) and transiliac osteotomies brings satisfactory pain relief and good radiologic outcomes in patients with cerebral palsy (CP) and the hip at risk of displacement. 9 It is, however, unknown whether this type of treatment gives long-lasting pain relief and stable hip long term, especially in primarily painful hips. Therefore, this study aims to present the outcomes of surgical treatment of painful neurogenic hip dislocations with VDRO and Dega transiliac pelvic osteotomy after more than 15 years of follow-up.
Materials and methods
It is a retrospective, institutional review board-approved analysis of patients with CP operated in our department between 1996 and 2008 due to painful neurogenic hip joint dislocation (migration percentage (MP) >80%). All patients provided informed written consent prior the analysis. All patients were non-ambulatory and presented severe functional impairment of GMFCS level IV and V. Only patients who underwent hip joint surgery as a primary hip surgical procedure and who were observed for minimum 15 years were included in this study. All patients underwent the same staged approach, starting with multi-level soft tissue release, followed by open reduction of the hip joint, VDRO with bone shortening, and Dega transiliac osteotomy. Out of the initial group of 653 patients treated surgically due to CP, we identified 376 patients who underwent hip surgery. A total of 81 patients (115 hips) had a hip open reduction, and for further study, we have chosen only 31 patients (46 hips) who had it done due to pain. Six patients died during the follow-up, 10 patients declined participation, and 15 patients (7 females, 8 males, 22 hips in total) remained in the follow-up for a minimum of 15 years (Figure 1).
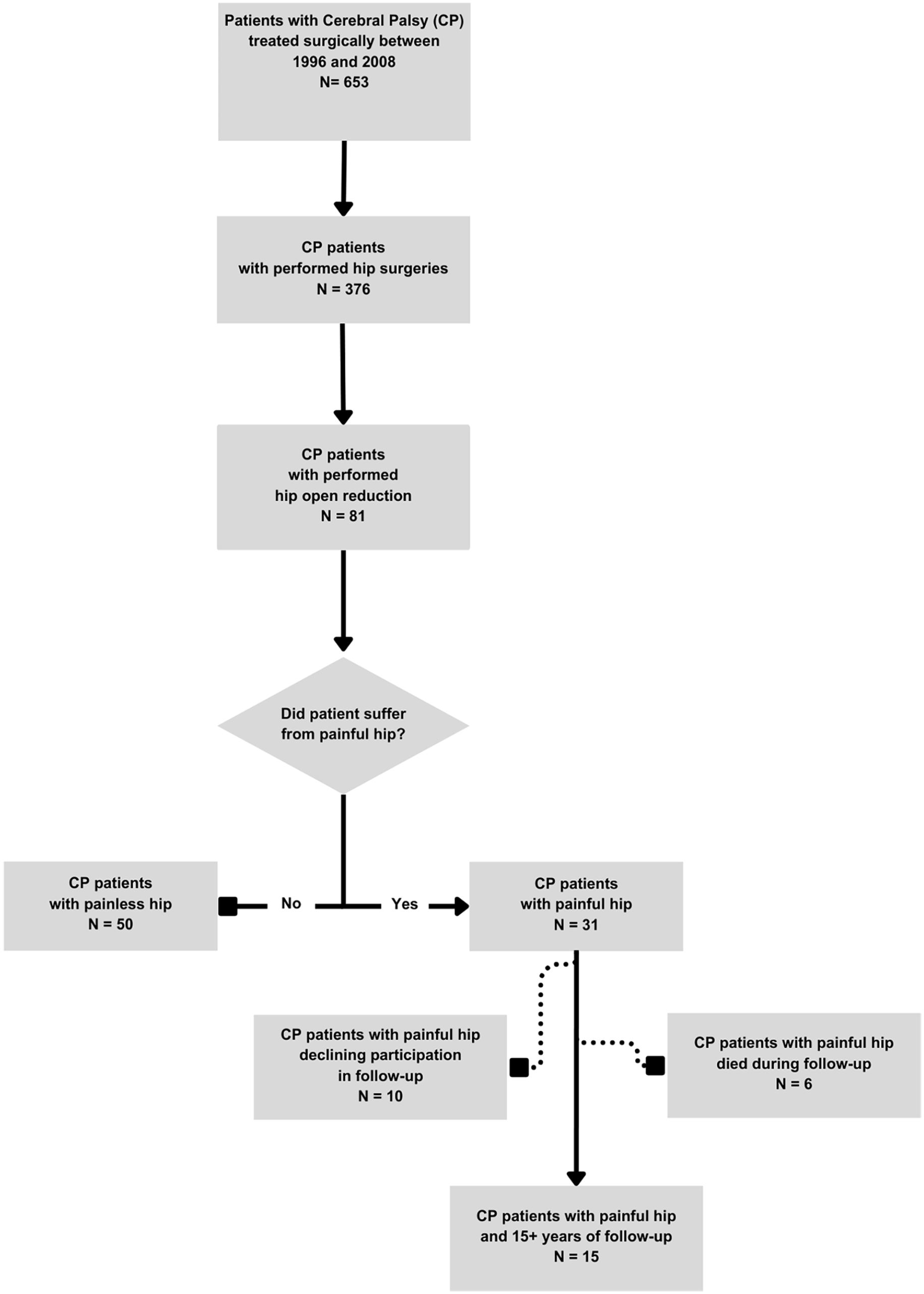
Flow chart of the study population selection.
A clinical examination of the hip joints (including measurements of hip flexion contracture, abduction with hip flexed, popliteal angle, and flexion of the knee joint) and a standardized radiographic examination were performed before treatment and at the final follow-up visit. We measured the MP and pelvic femoral angle (PFA). The head shape was assessed using the Rutz classification, 10 and the pain level was evaluated using the VAS-11 scale. Patients’ caregivers answered questions regarding pain during sitting, personal hygiene activities, and rest. The caregivers’ satisfaction with the treatment was also assessed with a validated Polish version of the Caregiver Priorities and Child Health Index of Life with Disabilities (CPCHILD) questionnaire.11,12
Treatment protocol
In all patients, we performed hip open reduction, proximal femoral varus derotation osteotomy, and Dega transiliac osteotomy in a previously described way. 13 Worth highlighting is the technique we used for the open reduction. During the procedure, the head of the femur was exposed by cutting the reflected head of the rectus femoris muscle, followed by a circumferential anterior to posterior capsule cut. After exposing the inside of the hip joint socket, cutting the ligament of the femoral head, and removing it, the inside of the acetabulum was evacuated. The shape of the femoral head was then evaluated.
Postoperatively, the limbs were immobilized in a spica cast with hips in full extension, neutral rotation, and with a 25–35-degree abduction for 6 weeks, followed by spica cast removal and hip range of motion (ROM) exercises. In all patients, metal implant was removed 1 year after index procedure on average.
Statistical analysis
The calculations were performed using the TIBCO Statistica 13.3 software (Palo Alto, CA, USA). The normality of the variable distribution was tested using the Shapiro–Wilk test.
Results
This study comprised 15 patients (22 operated hips, 7 females and 8 males) with spastic quadriplegia, 1 GMFCS IV and 14 GMFCS V, with an average age of 8 years and 9 months (range = 6–12 years) at the time of surgery. The average follow-up time was 17 years, 1 month (ranging from 15 to 18 years). Seven patients underwent bilateral and eight unilateral surgery.
We observed significant improvement in hip flexion contracture (p < 0.01), hip abduction (p < 0.05), and flexion of the knee joint (p < 0.001) facilitating patients care and positioning. While popliteal angle remained unchanged (p > 0.05), rectus femoris length checked through Ely’s test showed significant improvement (p < 0.05) (Table 1). Of note, those patients who underwent unilateral surgery experienced more significant ROM deterioration in the non-operated hip joint than before the surgery (p < 0.05) (Table 2).
Comparison of ROM and Ely’s test in the observed group before surgery and at the final follow-up appointment.
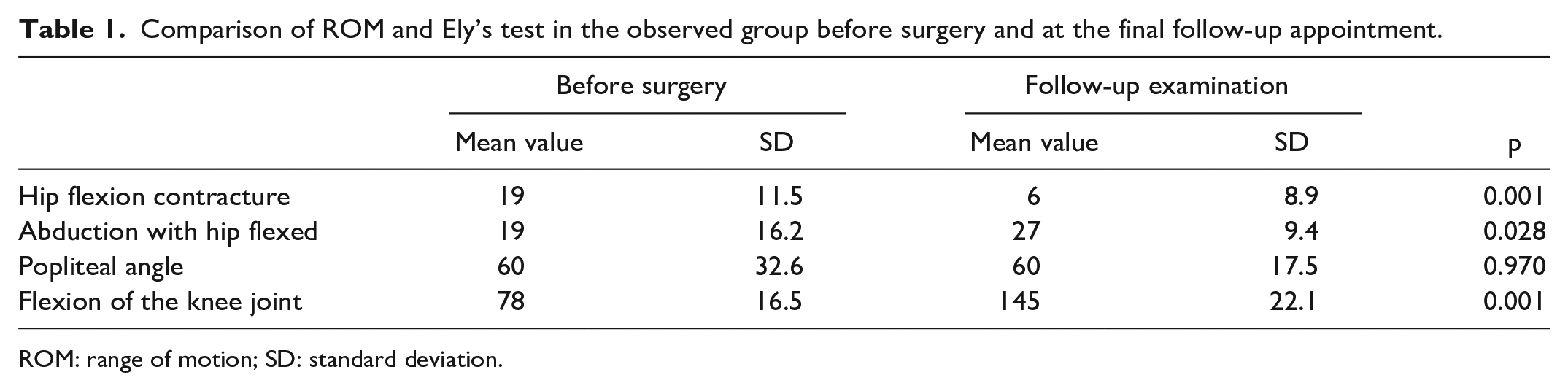
ROM: range of motion; SD: standard deviation.
Comparison of ROM on the non-operated side in patients who underwent unilateral surgery before surgery and at the final follow-up appointment.
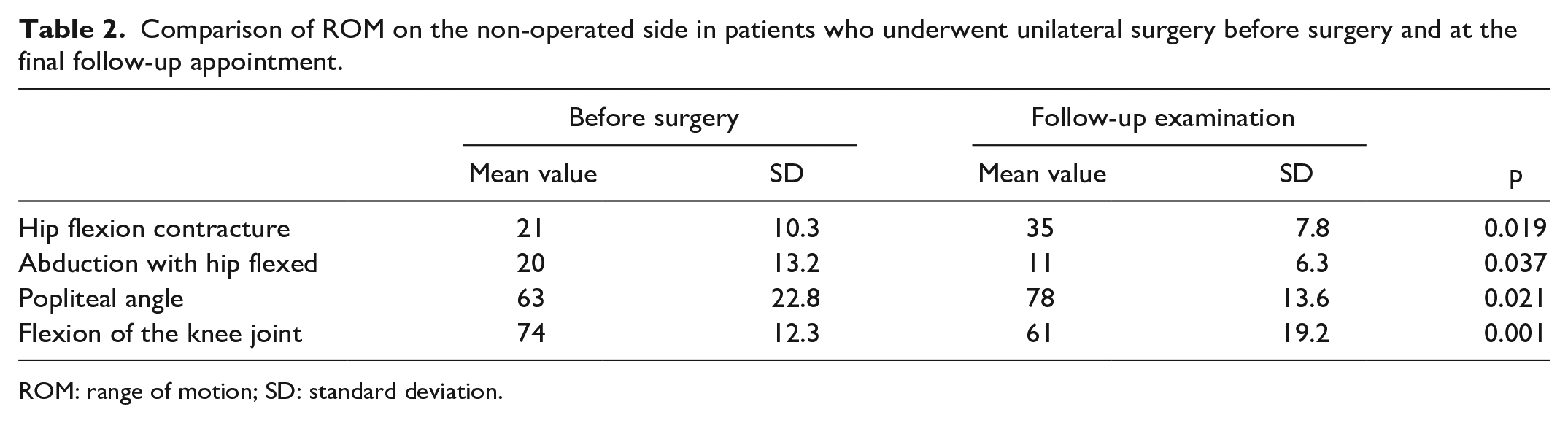
ROM: range of motion; SD: standard deviation.
Similarly to our findings in clinical examination, all evaluated radiographic parameters (MP, pelvic femoral angle, and Rutz femoral head shape classification) showed significant improvement when compared to the pre-operative findings (p < 0.001, p < 0.01, p < 0.05, respectively; Table 3). The degree of femoral head coverage significantly improved and remained stable in most patients during the long-term follow-up (Figure 2). Subluxation of one hip joint at the follow-up was observed, and one patient appeared to have a wind-blown deformity with hip dislocation of the non-operated side.
Comparison of radiological parameters in the observed group before surgery and at the final follow-up appointment.
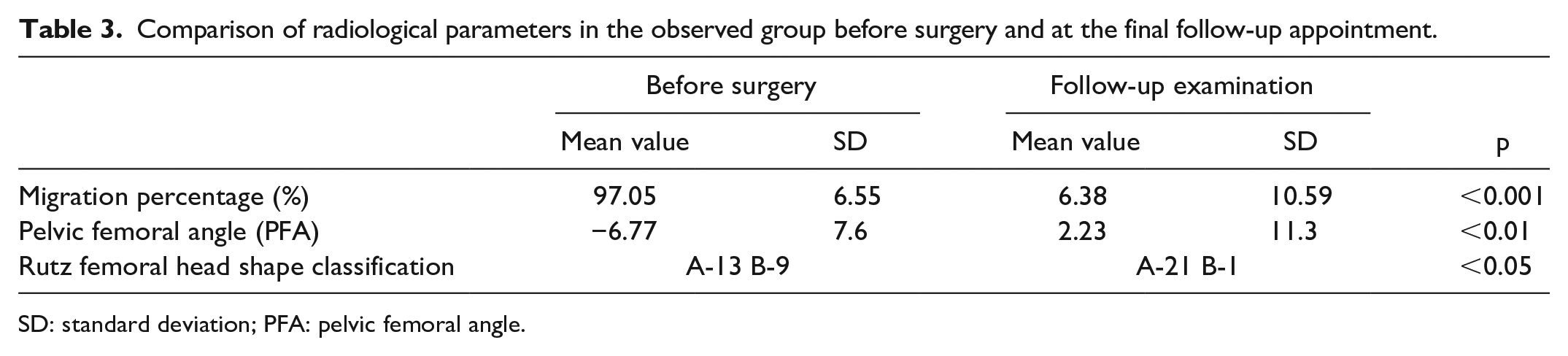
SD: standard deviation; PFA: pelvic femoral angle.
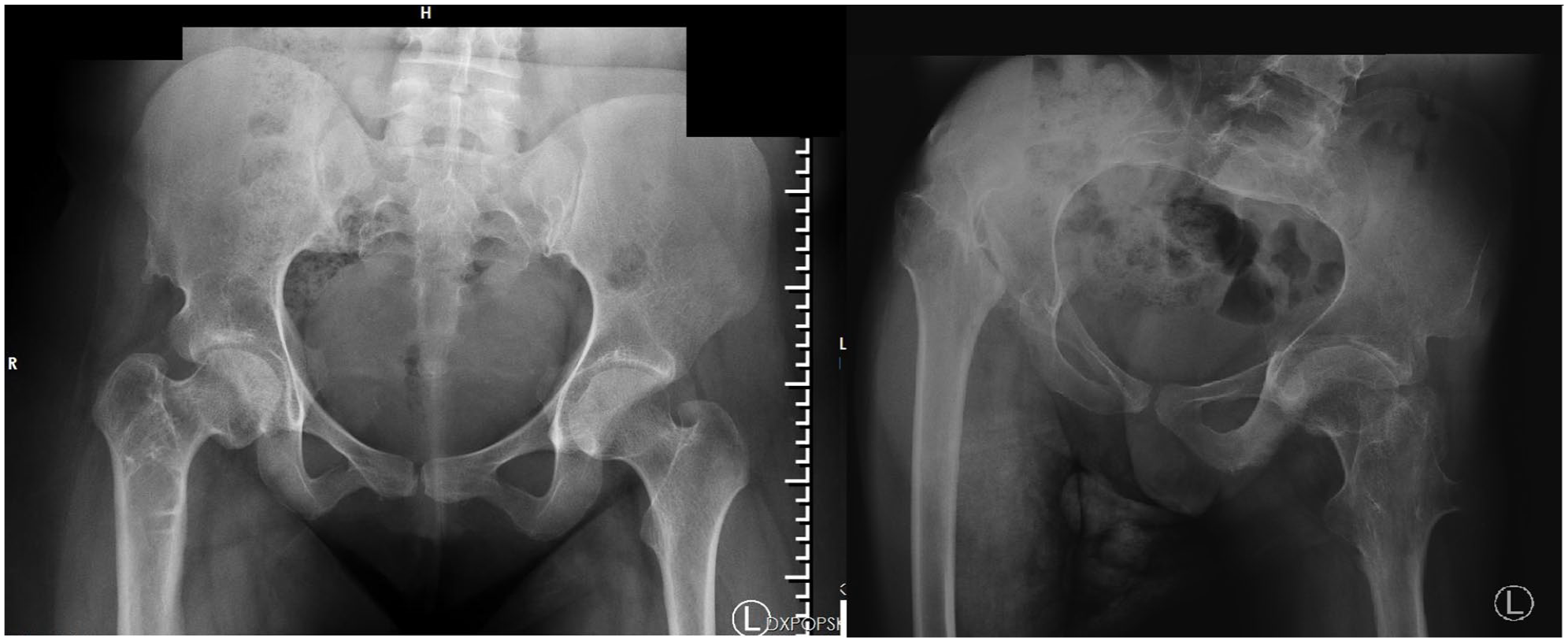
On the left AP pelvic X-ray of 29 years old female with good surgical results 16 years after unilateral open reduction, proximal femoral varus derotation osteotomy, and Dega transiliac osteotomy and on the right AP pelvic X-ray of 29 years old male with wind-blown deformity and dislocation of the non-operated joint, which appeared during follow-up.
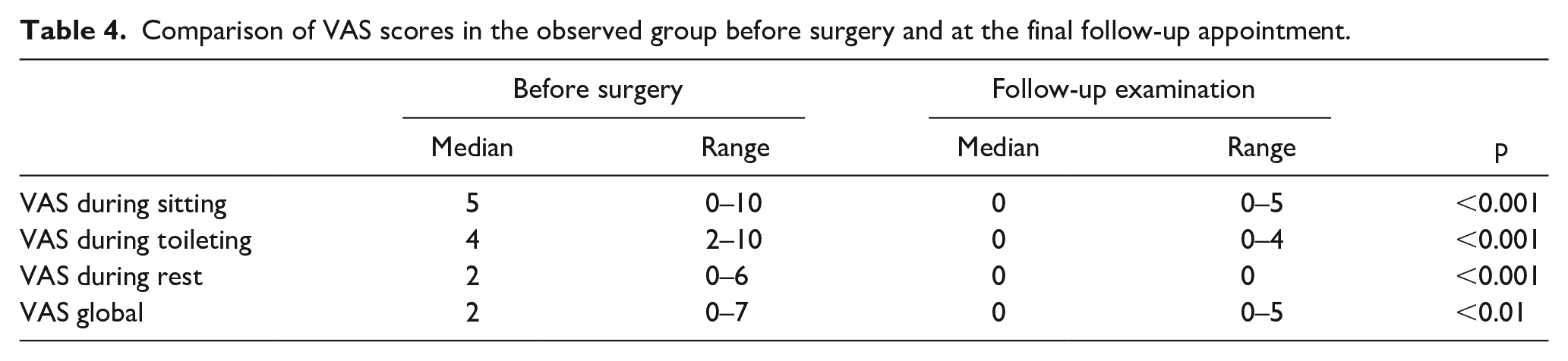
Interestingly, the surgery resulted in a significant reduction in pain (Table 4). VAS-11 score improvement was lower in older than younger children with CP in personal care activities (p < 0.05, median improvement 3 and 5, respectively). Moreover, girls experienced a more significant reduction in global VAS-11 score at the follow-up than boys (p < 0.05 median improvement 3 and 1, respectively).
Comparison of VAS scores in the observed group before surgery and at the final follow-up appointment.
The caregivers reported their children’s satisfaction of the surgical treatment outcomes through the CPCHILD questionnaire. Statistical analysis of the questionnaires revealed several interesting relations. First, the patients who underwent unilateral surgery experienced more frequent and intense pain during feeding, toileting, and sleeping (p < 0.01). In addition, the patients with a higher MP of the contralateral hip experienced more considerable and frequent discomfort during eating, toileting, and bed rest (p < 0.01). Increased PFA values correlated with more intense and frequent pain during bed rest. We also noticed that higher improvements in VAS scores resulted in less frequent and less intensive incidences of sadness and anger reported by patients (measured by the CPCHILD questionnaire) (p < 0.05). Finally, greater abduction range on the operated side positively impacted discomfort while toileting, bed rest, and sleeping.
Discussion
This study presents the long-term follow-up observations of surgically treated painful hip dislocations in patients with CP. It is a uniquely long observation for hips which were primarily painful, and which underwent reactive, surgical hip reconstruction through soft tissue releases with femur and pelvis osteotomies. Moreover, patients were not only assessed clinically and radiologically, but also patient reported outcomes were analyzed. This allowed us to systemically assess how surgical reconstruction of painful dislocated hip affects long-term wellbeing of patients with CP. Obviously, our study has some limitations, namely, the small number of patients in our group. This is, however, caused by the fact that most of the hips we operated were painless, and some of our patients were lost in long follow-up process. Nevertheless, to our knowledge, this is one of the longest observations of spastic painful hips which were reconstructed.
The Rutz classification is a revised and simplified version of the better known classification Melbourne Cerebral Palsy Hip Classification System (MCPHCS). 14 The Rutz classification of the femoral head shape is more straightforward, intuitive and independent of the MP than MCPHCS. Both classification schemas have clinical predictive value; however, MCPHCS was primarily intended for hips at skeletal maturity, and the Rutz classification can be used at any age. It is worth knowing that the femoral head shape classification system devised by Rutz was recently assessed with moderate to substantial intra-observer reliability and moderate inter-observer reliability. 15
Pain complaints in patients with CP are common with studies suggesting a prevalence of pain up to 74%.16 –18 Children with GMFCS level III–V experience hip pain more often than those at level I–II, which is also correlated with hip migration. Pain, in turn, significantly decreases the QoL.19,20 Therefore, SHD should be addressed surgically before pain appears and before hip fully dislocates. This is defined as proactive treatment and brings good results long term, both radiologically and clinically. 21 On the contrary, treatment of painful dislocated hip is more controversial, and there is a lack of evidence on the clinical and radiological fate of such hips in long-term observations. Our study addressed this problem, and we found that surgical reconstruction of painful hips in patients with CP is extremely successful with significant decrease of pain, improvement in ROM and patient (or their caregivers) feedback.
Painful hip is considered one of the most debilitating conditions among both immature and mature patients with CP. Vinkel et al. 22 described acute and chronic pain in children with CP. Our patients usually received treatment for chronic, secondary musculoskeletal pain due to deformities, misalignment, and spasticity.22,23 It is, however, debatable whether pain assessment based on caregivers opinion is reliable enough, and which of the scales are the most reliable in patients who are non-verbal and fully rely on their caregivers. 23 The most frequently used are VAS-11 or Numerical Rating Scale, but they mainly focus on pain intensity and are difficult to use in children with limited communication skills. Therefore, apart from VAS-11, we used CPCHILD questionnaire which helps in comprehensive understanding of life quality, functional abilities, wellbeing, and pain of patients with CP. 11 Importantly, it gathers data not only from the child but also from their caregivers. It was first published by Narayanan et al. 11 in 2006, and its Polish validated version has been used since 2022. 12 Therefore, we could only assess patients in our cohort this way at the final examination, as they were all operated in the years 1996–2008.
Surgical interventions in spastic painful hip bring fairly good results with significant hip pain relief. DiFazio et al. 24 described a decrease in hip pain 5 years after a reconstruction surgery, but according to their report, it did not change the caregiver burden. Similarly, our data showed that hip reconstruction gives long-lasting hip stability and significant pain reduction. This is also in keeping with Pruszczyński et al.’s 25 findings; however, their report showed that hip reduction did not prevent from early degenerative changes of the hip. Ulusaloglu et al. 26 show that residual subluxation (MP ≥ 30.5%) of the femoral head at the time of triradiate cartilage closure negatively affects the head shape and influences the severity of osteoarthritis. Alternatively, our and previous studies show that femoral head shape can be improved with time (Rutz A shape in 13 hips before hip reconstruction, and in 21 during final evaluation in our cohort) but only when the hip is reduced to the acetabulum after hip reconstruction surgery.27,28
Interestingly, pain decrease was noticed in all the patients, but smaller in those after unilateral hip dislocation surgery than in those who underwent bilateral surgery. Of note, there is a correlation between the pain and the position of the opposite hip. Namely, the patients with high MP of the contralateral hip and high PFA were more prone to pain when examined 15 years after hip reconstruction. This finding can be possibly explained by a lack of lower limb symmetry and potential problems with balance during sitting and lying.29,30 Therefore, we now believe that even in asymmetrical/unilateral hip displacements, both hips should be addressed surgically to prevent from pelvis asymmetry and potential contralateral pain. This so-called proactive approach in decision-making process is nowadays recommended based on other authors’ observations and American Academy for Cerebral Palsy and Developmental Medicine recommendations.21,31,32
Conclusion
In conclusion, this study provides strong evidence for long-term pain relief, improvement in patient care and positioning, as well as and radiological and clinical improvement after surgical reconstruction of painful dislocated spastic hips in patients with CP.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521241233165 – Supplemental material for Long-term outcomes of reconstructive treatment for painful dislocations in patients with cerebral palsy
Supplemental material, sj-pdf-1-cho-10.1177_18632521241233165 for Long-term outcomes of reconstructive treatment for painful dislocations in patients with cerebral palsy by Aleksander Koch, Maciej Kasprzyk, Bartosz Musielak and Marek Jóźwiak in Journal of Children’s Orthopaedics
Footnotes
Author contributions
A.K. was responsible for conceptualization, data curation, formal analysis, investigation, methodology, project administration, resources, visualization, and writing—original draft. M.K. was responsible for conceptualization, data curation, formal analysis, investigation, methodology, project administration, resources, visualization, and writing—original draft. B.M. was responsible for conceptualization, investigation, methodology, visualization, and writing—review and editing. M.J. was responsible for conceptualization, funding acquisition, investigation, project administration, supervision, validation, and writing—review and editing.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The Medical Ethics Committee of the Poznan University of Medical Sciences approved this research (UMP 266/15).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
All patients and legally authorized representatives of the patients provided informed written consent prior the analysis.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.