
Abstract
Background:
This large, retrospective, single-center study aimed to compare the outcomes of unilateral hip reconstruction and bilateral hip reconstruction in children with non-ambulatory cerebral palsy and ascertain risk factors for recurrent instability and reoperation.
Method:
We performed a retrospective review of 137 hip reconstructions performed for patients with cerebral palsy. Preoperative and postoperative clinical and radiological parameters were documented, including hip migration percentage, acetabular index, the Gross Motor Function Classification System, the Melbourne Cerebral Palsy Hip Classification System, hip abduction, and pelvic obliquity.
Results:
Overall, 49 patients underwent bilateral hip reconstruction, and 37 patients underwent unilateral hip reconstruction. In the unilateral hip reconstruction group, the reconstructed hip remained stable (with a migration percentage < 33%) in 59% of patients compared to 74.4% of the more affected hips in the bilateral hip reconstruction group (p = 0.02). Of the unreconstructed hip in the unilateral hip reconstruction group, 74.4% remained stable (with a migration percentage < 33%), compared to 78.8% of the less affected hips in the bilateral hip reconstruction group. A level pelvis was maintained at final follow-up in significantly more patients in the bilateral hip reconstruction group than the unilateral hip reconstruction group (p = 0.002). Further surgical intervention was performed in 41% of the unilateral hip reconstruction group, compared with 11.5% in the bilateral hip reconstruction group (p = 0.001). Surgery performed under the age of 8 years and not performing an acetabular osteotomy were found to be risk factors for recurrent instability in all groups.
Conclusion:
Our series suggests that in terms of recurrent instability after hip reconstruction in cerebral palsy, protective factors against this complication include bilateral hip reconstruction, hip reconstruction after 8 years of age, and the use of an acetabular osteotomy.
Introduction
The severity of the motor dysfunction of cerebral palsy (CP) has been graded by the Gross Motor Function Classification System (GMFCS). 1 These GMFCS levels can be applied to all children with CP but generally remain static between the ages of 6 and 12 years. In a community-based radiographic study conducted in Norway using a national surveillance program for children with CP, hip displacement occurred in 26% of the population of children with CP. However, 63% of patients with hip displacement had GMFCS levels IV or V. The average annual rise in migration percentage (MP) for kids with quadriplegic CP varies by age, with a 13% increase before 5 years of age and a 7% increase beyond that age. 2
The wider literature reports up to 75% of patients with CP having some degree of hip subluxation or dislocation making it the second most common deformity, after ankle equinus.3 –6
Untreated, these unstable hips are associated with lower quality of life scores, pelvic obliquity, poor sitting balance, and scoliosis; carers often report issues with regard to pain and perineal hygiene.7 –11 For these reasons, surgical intervention has been widely reported as beneficial.10,12 –18 The aim of surgery in the best-case scenario is to prevent the progression of a migrating hip to a dislocated hip to relieve or prevent pain. In the worst cases, the aim is to relocate the hip to reduce pain. Treatment options are on a spectrum from botulinum toxin A injections to the hip flexors and adductors, soft-tissue releases to these structures, or bony osteotomies.18 –22 Patients with CP often have asymmetrical hip deformities with associated pelvic obliquity beneficial to the patient in the long term.23 –26 Unilateral surgery in CP has been found to lead to an increased risk of subsequent subluxation and instability in the affected or contralateral hip, even in the absence of preoperative instability, leading some authors to advocate bilateral reconstruction in one sitting if possible.12,25 –27 There are also reports of good outcome without compromise of the “normal” hip in unilateral reconstruction.6,28
Therefore, the question of whether bilateral procedures should be the gold standard of care in a clinical scenario in which there is significant pelvic obliquity, a large MP, or contralateral contracture is still considered to be unanswered.29,30
The primary aim of this large single-unit study, carrying out both unilateral and bilateral reconstruction, was to ascertain risk factors for recurrent instability and reoperation. The secondary aim was to assess how the less affected hip behaved following operative intervention in each group and propose an algorithm for decision-making.
Method
We performed a retrospective review of consecutive hip reconstructions, performed at a single center by senior pediatric orthopedic surgeons specializing in CP surgery, for hip instability in patients with CP. All patients were non-ambulatory. The medical records of 132 consecutive patients (172 hips) were reviewed, with patients operated on between April 2001 and January 2016. Patients who had undergone previous hip reconstruction for either hip were excluded, as were patients in whom a staged bilateral procedure was planned (one patient). Patients who underwent salvage procedures for either the femur or acetabulum were excluded. Inclusion criteria included all patients with spastic CP with a GMFCS IV or V, who underwent hip reconstruction (varus derotation osteotomy (VDRO) of one or both hips plus/minus pelvic osteotomy) between the years 2001 and 2016. All those with a radiological follow-up of less than 4 years were also excluded, and those with incomplete preoperative, intraoperative, and postoperative clinic notes giving a total of 88 consecutive patients, with 137 hips reconstructed. Overall, 44 patients were female, and 44 patients were male. Patients’ preoperative degree of motor disability was assessed and recorded by the GMFCS. 1 However, 47 patients were Grade V, and 38 were Grade IV. The mean age at the time of surgery was 8.4 (SD 3.1) years with a mean follow-up of 6.7 (SD 1.8) years.
All radiographs and notes were assessed by the same examiner. Hips were grouped into categories according to the MP: < 33% MP, 34%–50% MP, 51%–100% MP, and > 100% MP. 14
Pelvic obliquity, an established proxy for sitting balance, was measured on each radiograph while the patient was supine with legs straight, in the middle of the table, using the method described by Hägglund and his colleagues31,32 preoperatively, postoperatively when out of brace or hip spica, and at final follow-up radiograph, prior to any further intervention.
Hägglund et al. 31 described the technique of measurement of pelvic obliquity. Measurement was made from standardized anteroposterior radiographs captured for hip surveillance, with the pelvis horizontal to the floor and the patella positioned anteriorly. Any lumbar lordosis secondary to hip flexion contracture is corrected by placing a roll under the knee to maintain hip and knee flexion. Hip abduction and adduction are limited to neutral as far as possible. The angle of pelvic obliquity is an angle subtended by a horizontal line parallel to the line of the frame of the radiograph with a line joining the maximum prominence of the ischial tuberosities (inter-tuberosity line, ITL) or through the inferior aspect of both triradiate cartilages (Hilgenreiner’s line) (Figure 1).
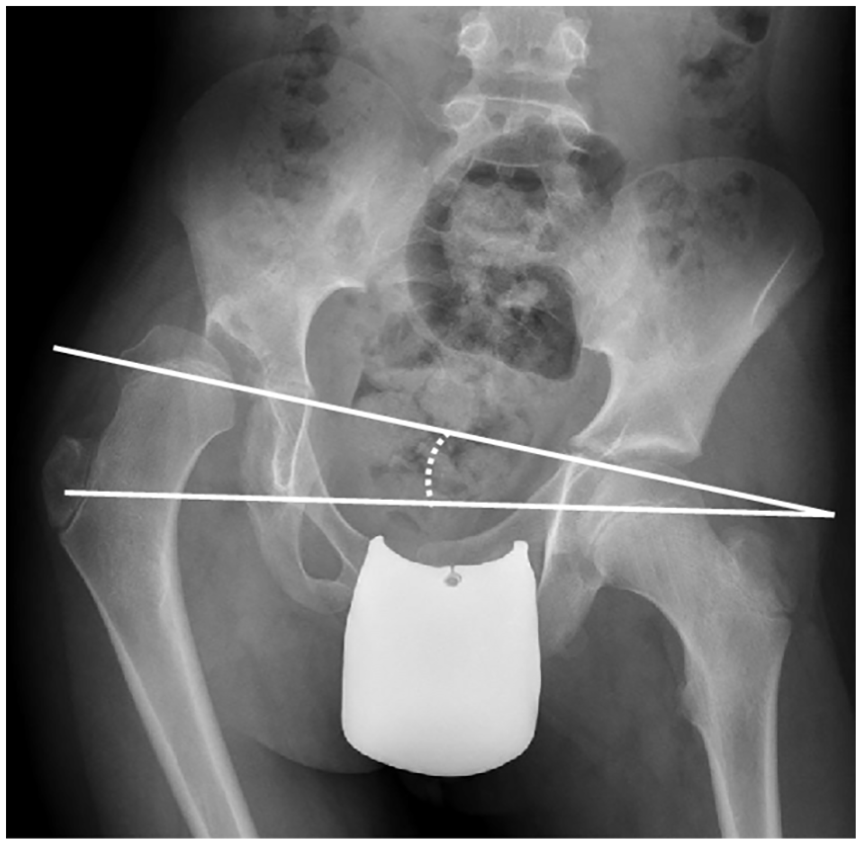
Pelvic obliquity. The angle of pelvic obliquity is an angle subtended by a horizontal line parallel to the line of the frame of the radiograph with a line joining the maximum prominence of the ischial tuberosities (ITL) or through the inferior aspect of both triradiate cartilages (Hilgenreiner’s line) (image from Hägglund 32 ).
The Melbourne Cerebral Palsy Hip Classification System (MCPHCS) was used pre- and postoperatively. It was developed as a combination of MP, pelvic obliquity, and femoral head and acetabulum morphology and is graded from I to VI, with Grade I representing a radiologically normal hip, to Grade VI, which represents a dislocated hip that has required salvage surgery. The classification used can be seen in Figure 2. 33 Index (AI) was also measured pre- and postoperatively in all hips.
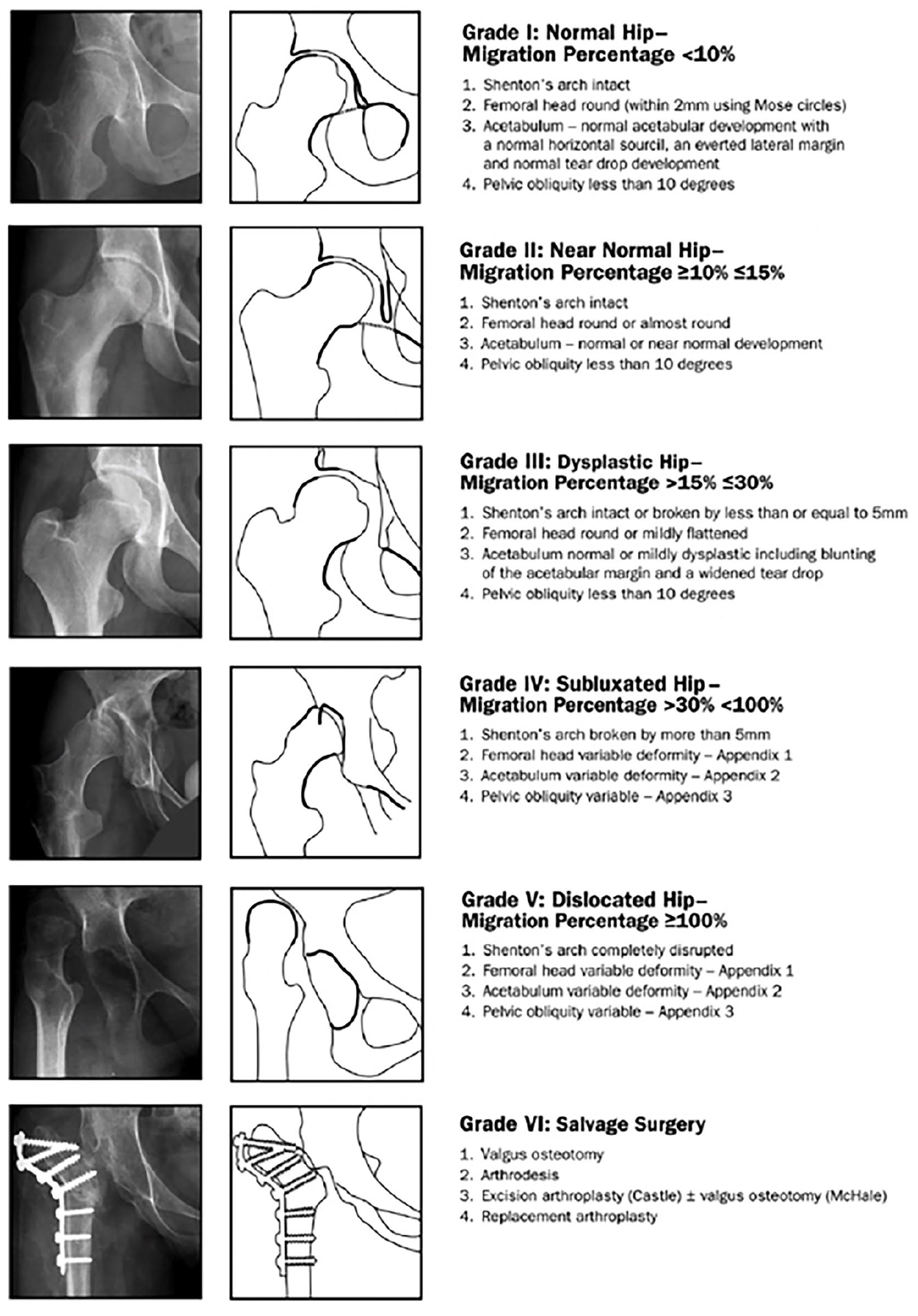
The MCPHCS. It has been shown to have excellent inter- and intraobserver reliability, and is graded from I to VI, with Grade I representing a radiologically normal hip, to Grade VI, which represents a dislocated hip that has required salvage surgery (image from Shrader et al. 33 ).
Adduction contracture was noted in the clinical setting for our patients; therefore, this information was extracted from clinical notes and categorized in line with the cerebral palsy integrated pathway (CPIP) preoperatively and at final follow-up (or before further intervention). 34 Poor abduction was classified as less than 30°, and satisfactory if 30° or more.
Bilateral (BHR) and unilateral (UHR) hip reconstruction patients were stratified into separate cohorts for statistical analysis. Pre- and postoperative clinical abduction, pelvic obliquity, acetabular index (AI), MCPHCS, GMFCS level, and soft-tissue hip adduction contracture were compared for the two cohorts.
The need for further surgery was also recorded; the authors are mindful that the fact that further surgery is recommended does not necessarily mean that this surgery will be undertaken. This last point is for the interest of the reader only, rather than specifically representing a surgical failure rate.
Preoperative and intraoperative management decision-making algorithm
Clinical and patient factors were integral to preoperative decision-making with regard to the decision to perform the BHR.
If both hips had an MP > 33%, bilateral reconstruction was undertaken in every case in this series. Poor sitting balance (pelvic obliquity) and poor abduction (<30°) of the less affected hip were the basis of the decision to proceed to bilateral reconstruction in cases where the less affected hip had an MP < 33%.
In addition, all patients underwent an examination under anesthesia (EUA) to complete surgical planning intraoperatively, if a test of stability revealed that abduction and rotation improved reduction of the contralateral hip, then reconstruction of the contralateral side was undertaken.
All operated hips had an adductor longus, brevis (preserving the anterior branch of the obturator nerve), and gracilis release. All patients had a psoas soft-tissue release at the lesser trochanter bilaterally.
All operated hips underwent a femoral VDRO; the usual amount was 30° increase in varus, but the final amount of variation depended on how much abduction was needed on EUA to reduce the hip and keep it stable and well reduced deep into the acetabulum. Shortening of the femur was also performed to account for the break in Shenton’s line (the distance between the inferomedial border of the femoral neck and inferior border of the superior pubic ramus on an anteroposterior pelvic X-ray). A reshaping, volume reduction pelvic osteotomy was performed to treat a deficient acetabulum in all necessary cases (Dega, Pemberton, or Albee shelf). Generally, if the AI was over 30° preoperatively, an acetabular osteotomy was planned. This plan was confirmed on intraoperative EUA, and volume reduction osteotomy was added to the surgical procedure plan if flexion improved reduction and coverage of the femoral head. An open reduction via anterior approach to the hip with capsulorrhaphy was used if indicated, when VDRO was not sufficient to reduce the hip adequately.
All patients were braced in abduction using a Newport Brace for 6 weeks, except five patients who were too small for a Newport brace and were immobilized in a hip spica plaster, bilaterally above the knee.
Statistical analysis of the data was performed by statistician, using SPSS (IBM Corp. Released 2020. IBM SPSS Statistics for Windows, Version 27.0. Armonk, NY: IBM Corp). All data series were subject to tests of variance, and parametric or non-parametric inferential statistical analysis and descriptive analysis methods were chosen accordingly, with a p-value of less than 0.05 taken as significant with appropriate Bonferroni adjustment.
Results
Overall, 49 patients underwent bilateral reconstruction of the hips (BHR), and 37 patients underwent UHR. Their pre- and postoperative data can be seen in Tables 1 and 2.
Preoperative demographic, clinical, and radiological findings.
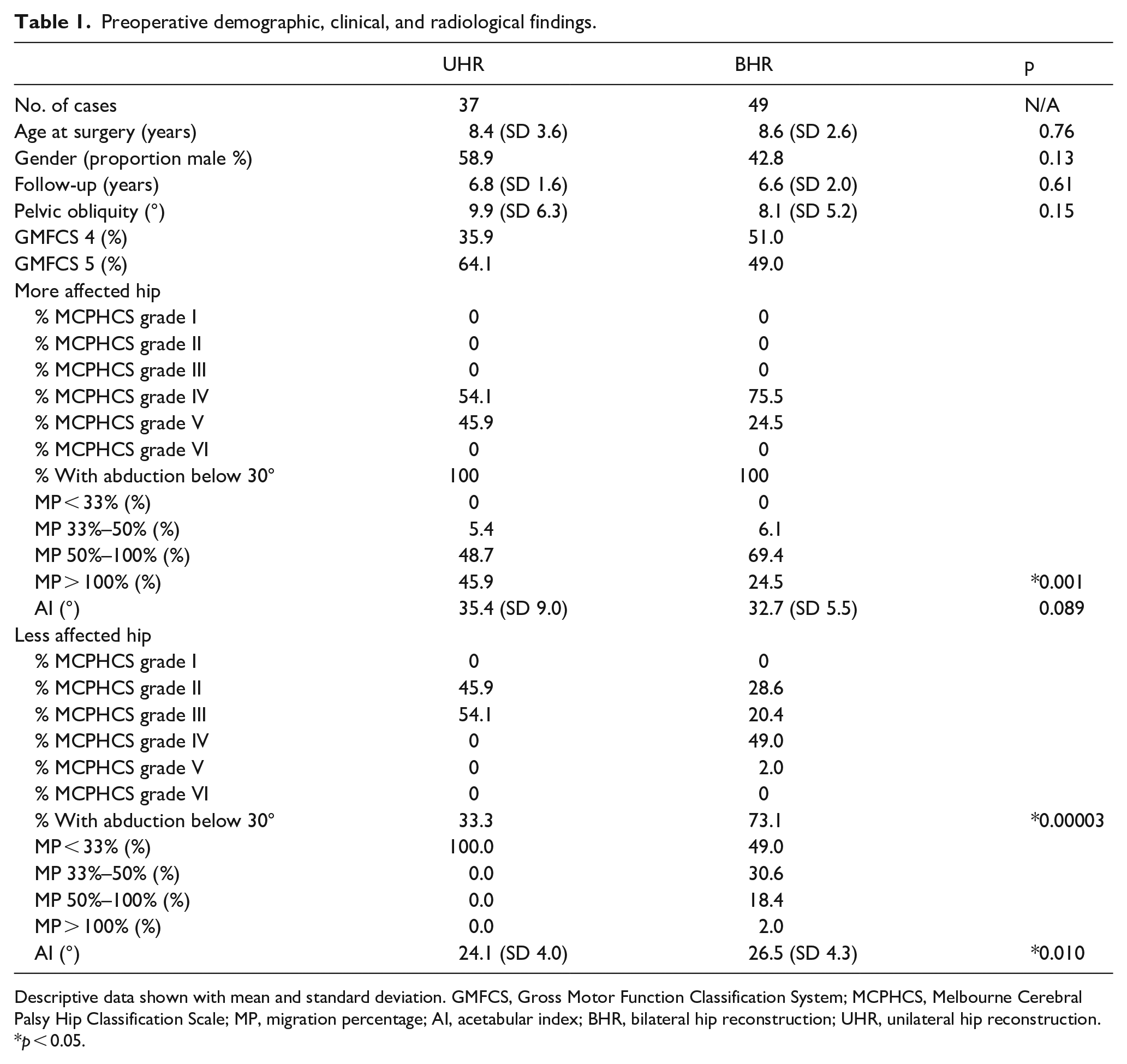
Descriptive data shown with mean and standard deviation. GMFCS, Gross Motor Function Classification System; MCPHCS, Melbourne Cerebral Palsy Hip Classification Scale; MP, migration percentage; AI, acetabular index; BHR, bilateral hip reconstruction; UHR, unilateral hip reconstruction.
p < 0.05.
Postoperative (at last follow-up) clinical and radiological findings.
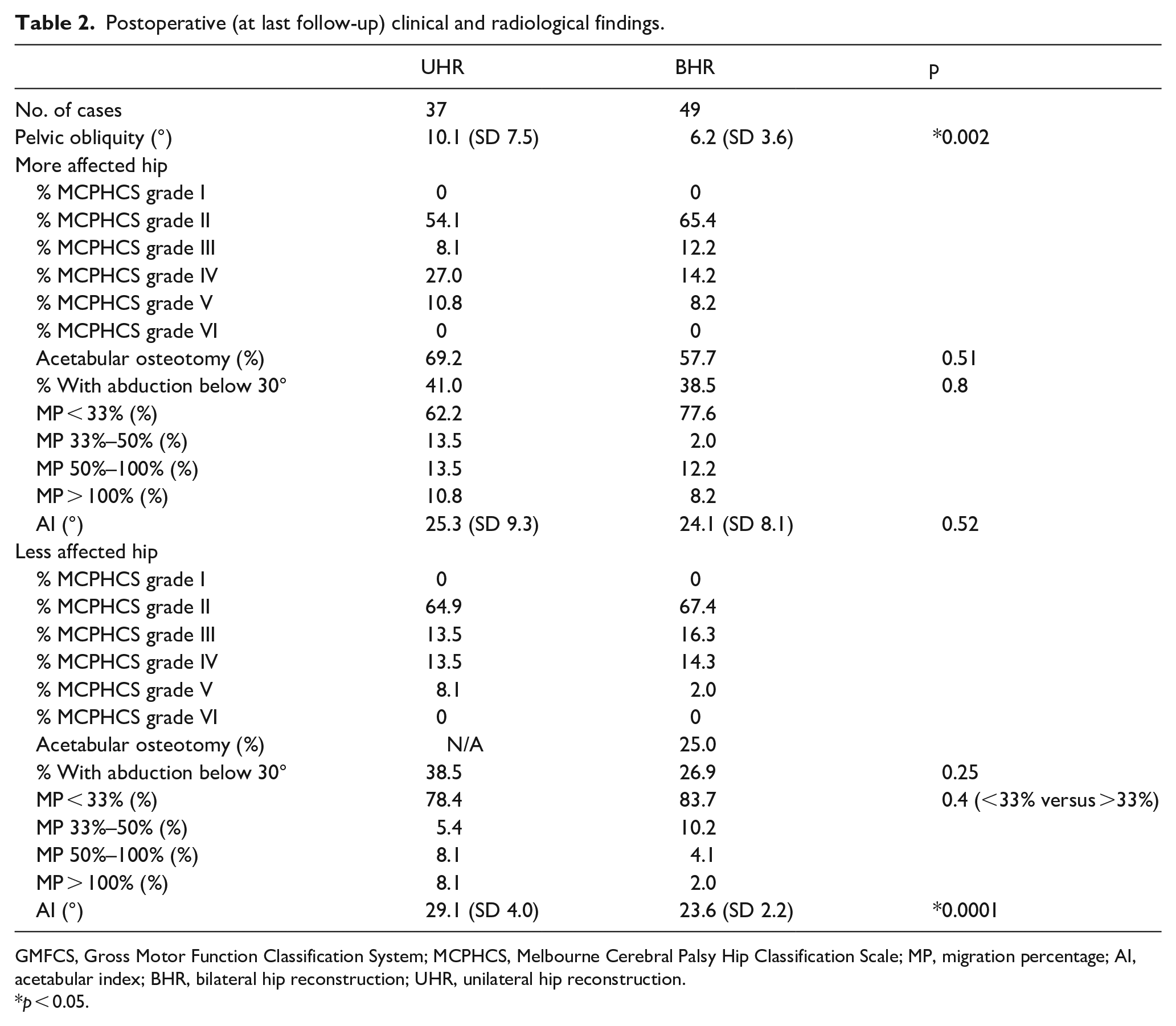
GMFCS, Gross Motor Function Classification System; MCPHCS, Melbourne Cerebral Palsy Hip Classification Scale; MP, migration percentage; AI, acetabular index; BHR, bilateral hip reconstruction; UHR, unilateral hip reconstruction.
p < 0.05.
The average age of surgery was not statistically significantly different, 8.4 (SD 3.6) years in the UHR group and 8.6 (SD 2.6) years in the BHR group (p = 0.76). There was also no statistical difference between the gender proportions of the groups.
The median GMFCS level did differ between groups, the median GMFCS level was V in the UHR cohort and IV in the BHR cohort.
The more affected hip in both groups had an MP of above 33% and found to have abduction less than 30° preoperatively in all cases in both groups. The severity of migration was significantly different in the two cohorts—with 43.6% in the UHR cohort having an MP of over 100%, and only 19.2% in the BHR cohort with an MP of over 100% (Mann–Whitney U test, p = 0.001).
Preoperatively, the less affected hip in the UHR group was found to have an MP of less than 33% in all patients, as expected. In the BHR group, 46.2% of patients had an MP of less than 33% in the less affected hip.
In the BHR group, of the 46.2% of patients with a less affected hip with an MP of less than 33%, 54% had abduction limited to less than 30°.
There was no statistically significant difference in pelvic obliquity between groups preoperatively (UHR group 9.9° (SD 6.3°) versus BHR group 8.1° (SD 5.2°), p = 0.15). Immediately postoperatively, there was also no statistically significant difference (UHR group 4.4° (SD 3.1°) versus BHR group 4.8° (SD 3.2°), p = 0.56), although the pelvic obliquity in both groups had reduced statistically significantly (UHR group p = 0.0001, BHR group p = 0.0003). At last follow-up, the difference between pelvic obliquity in the two groups was statistically significant (UHR group 10.1° (SD 7.5°) versus BHR group 6.2° (SD 3.6°), p = 0.002), suggesting that improvement in pelvic obliquity, and thus sitting balance, persisted till final follow-up in those patients who received a bilateral reconstruction.
In the BHR group, in the subgroup of less affected hips with above 30° of hip abduction and less than 33% MP, there is a high proportion of GMFCS V patients—7 out of 11 cases, suggesting that these patients received a bilateral reconstruction because their underlying disease was worse, and it felt that the other hip was likely to deteriorate if left untreated.
All hip reconstructions were successful, that is, intraoperative stability on full range of movement on examination under image intensifier was achieved and postoperatively all hips had an MP of < 33% on first follow-up radiograph out of brace or hip spica cast.
The decision to perform an acetabular osteotomy was always based on intraoperative examination under image intensifier. Once VDRO had been performed, an EUA was performed and acetabular coverage was assessed. If the coverage was insufficient, a pelvic osteotomy was performed in the direction of the insufficiency. Therefore, not all hips with an AI considered mildly dysplastic were treated with an acetabular osteotomy. It is important to note, however, that both lead surgeons involved had a very “low threshold” for performing acetabular osteotomy. In the UHR group, 69.2% hips were reconstructed with an acetabular osteotomy to reduce the AI to below 30°. The volume-reducing osteotomy was the choice of the lead surgeon based on their training and experience, a Pemberton or a Dega osteotomy. An Albee shelf was performed when the patient was approaching skeletal maturity, above 12 years of age. However, 24.3% were Pemberton osteotomies, 59.5% Dega osteotomies, and 16.2% were Albee shelf osteotomies. In the BHR group, 57.7% of more affected hips were reconstructed with an acetabular osteotomy. Meanwhile, 37.8% were Pemberton osteotomies, 32.4% Dega osteotomies, and 27.0% were Albee shelf osteotomies. In total, 46.7% of the cases with acetabular osteotomy of the more affected side also received acetabular osteotomy of the contralateral less affected side, with the same osteotomy being performed on both sides.
The proportion of hips reconstructed with pelvic osteotomy for the more affected hip was not significantly different between cohorts, 69.2% in the UHR cohort and 57.7% in the BHR cohort (p = 0.51). However, of the less affected hips in the BHR cohort, only 25% had a pelvic osteotomy as part of the reconstruction.
The average AI of the UHR group preoperatively was 24.1° (SD 4.0°). In the BHR group, the average AI of the more affected hip was 32.7° (SD 5.5°), and 26.5° (SD 4.3°) in the less affected hip. The average AI of hips reconstructed with pelvic osteotomy in the UHR group was 40.5° (SD 9.6°) compared to 25.8° (SD 3.2°) in those that did not have a pelvic osteotomy. In the BHR group, the average AI of hips reconstructed with pelvic osteotomy was 35.4° (SD 5.4°) for the worse hip, compared to 25.9° (SD 2.4°) in those worse hips that did not have a pelvic osteotomy. For the less affected hip, that is, the hip with the lower MP, the average AI of hips reconstructed with pelvic osteotomy was 33.9° (SD 2.1°), compared to 25.1° (SD 4.1°) in those less affected hips that did not have a pelvic osteotomy.
On analysis of hips that suffered relapse to MP > 33% by last follow-up, in the UHR group, the mean AI was 26.6° (SD 8.4°) compared to 24.5° (SD 4.3°) in those that remained with an MP of < 33%. For the worse hip in the BHR group, relapsed hips had an AI of 23.8° (SD 2.8°) compared to 23.4° (SD 2.2°) in those that did not relapse. For the better hip in the BHR group, relapsed hips had an AI of 22.3° (SD 2.0°) compared to 22.9° (SD 2.3°) in those that did not relapse. No group showed a significant difference, suggesting that recurrence of migration is not likely to have a causal relationship with AI.
In the UHR group, 10.8% of hips required an open reduction for reconstruction. Of these four hips, three were in the group that did not relapse and one in the relapsed group. There is no statistical significance between groups; therefore p = 0.58.
In the BHR group, 6.1% of more affected hips required an open reduction (two hips in the group that did not relapse and one in the group that did relapse) for reconstruction (not significant, p = 0.41), and 2.1% of the less affected hips (one case found in the group that did not relapse). All hips requiring an open reduction had an MI of over 100% preoperatively. There was no statistical difference between those hips that relapsed and those that did not with regard to open reduction of the hip during reconstruction.
In the UHR cohort, 41% of the more affected hips relapsed to less than 30° of abduction, whereas in the BHR cohort, 38.5% relapsed to less than 30° of abduction (p = 0.8). In the UHR cohort, the unreconstructed hip relapsed to less than 30° of abduction in 38.5% of patients, compared to 26.9% of patients in the less affected BHR group, which was not statistically significant (p = 0.07)
In the UHR cohort, the MCPHCS grade for the more affected hips was either IV or V (54.1% and 45.9% respectively) preoperatively. The less affected hips were graded II or III preoperatively (45.9% and 54.1% respectively). Postoperatively in the UHR group, operated hips at last follow-up were found to be 54.1% Grade II, 8.1% Grade III, 27.0% Grade IV, and 10.8% Grade V. The non-operated hip was found to be Grade II in 64.9%, Grade III in 13.5%, Grade IV in 13.5%, and Grade V in 8.1%.
In the BHR group, the more affected hip was found to be MCPHCS grade IV in 75.5% of hips and grade V in 24.5% preoperatively. Postoperatively these were graded at last follow-up as 65.4% Grade II, 12.2% Grade III, 14.2% Grade IV, and 8.2% Grade V. Preoperatively, the less affected hip in the BHR group was Grade II in 28.6%, Grade III in 20.4%, Grade IV in 49%, and Grade V in 2.0%. Postoperatively, these were Grade II in 67.4%, Grade III in 16.3%, Grade IV in 14.3%, and Grade V in 2%.
In the UHR group, 94.6% of the operated hips remained in the same MCPHCS grade or reduced grades postoperatively at last follow-up (21.6% remained in the same grade, 10.6% reduced one grade, 37.8% reduced two grades, 21.6% reduced three grades, 2.7% reduced four grades, and 5.4% increased one grade). In the unoperated hip group, 27% remained in the same MCPHCS grade. No hips in this group reduced in MCPHCS grade between pre- and last postoperative imaging, as expected. However, 45.9% increased by one grade, 18.9% by two grades, 5.4% by three grades, and 2.7% by four grades.
In the BHR group 95.9% of more affected hips remained in the same MCPHCS grade or reduced grade postoperatively at last follow-up (10.2% remained in the same grade, 18.4% reduced one grade, 57.1% reduced two grades, 6.1% reduced three grades, 4.1% increased one grade). In the less affected hip group, 91.8% of more affected hips remained in the same MCPHCS grade or reduced grade postoperatively at last follow-up (38.8% remained in the same grade, 16.3% reduced one grade, 24.5% reduced two grades, 12.2% reduced three grades, 4.1% increased one grade, and 4.1% increased by two grades).
Regarding MP at last follow-up, in the UHR group, the reconstructed hip had an MP < 33% in 59% of patients compared with 74.4% of the more affected hips in the BHR group (p = 0.02). Of the unreconstructed hip in the UHR group, 74.4% had an MP < 33%, compared to 78.8% of the less affected hips in the BHR group. Although higher, this was not statistically significant (p = 0.4).
Regarding further surgical intervention, there was a significant difference between groups. Further surgical intervention, limited to revision reconstruction, reconstruction of the unoperated side, and proximal femoral excision of an operated hip, was performed in 41% of the UHR group, compared to 11.5% in the BHR group (p = 0.001). When stratified by age, it is found that the reoperation rate in both groups is mostly in patients operated on when below 8 years of age; in the UHR cohort, 16 of the 17 patients needing further surgery were below 8 years of age at the time of hip reconstruction. In the BHR cohort, five of the six patients needing further surgery were below 8 years of age.
The frequency of other complication was low. There was a fracture rate of 2.6%, zero cases of avascular necrosis, and a 9% rate of superficial infection with no cases requiring metal removal or wound debridement.
Table 3 compares the preoperative data of reconstructed hips that relapsed to over 33% MP by the end of the follow-up period. Two consistent risk factors for relapse are identified—surgery performed below the age of 8 years, and not performing an acetabular osteotomy. The percentage of relapsed hips in the UHR group reconstructed below the age of 8 years was 52.2 and only 7.1% in those that did not relapse (p = 0.00001). In the worse hip of the BHR group that relapsed, 55.5% were reconstructed below the age of 8 years, and 38% in those that did not show relapse (p = 0.01). Of the better hip in the BHR group, 73% of the relapsed hips were reconstructed below the age of 8 years, versus 50% in those that did not show relapse (p = 0.0008). The differences in all three groups are very statistically significant. Performing hip reconstruction after the age of 8 years is therefore protective, but not always practical. Due to the progressive nature of migration of the hip in CP, it is recommended that early intervention is performed, but the outcome stratified by age is an important discussion point for future planning and informed consent.
Relapsed operated hips versus successful reconstruction at last follow-up.
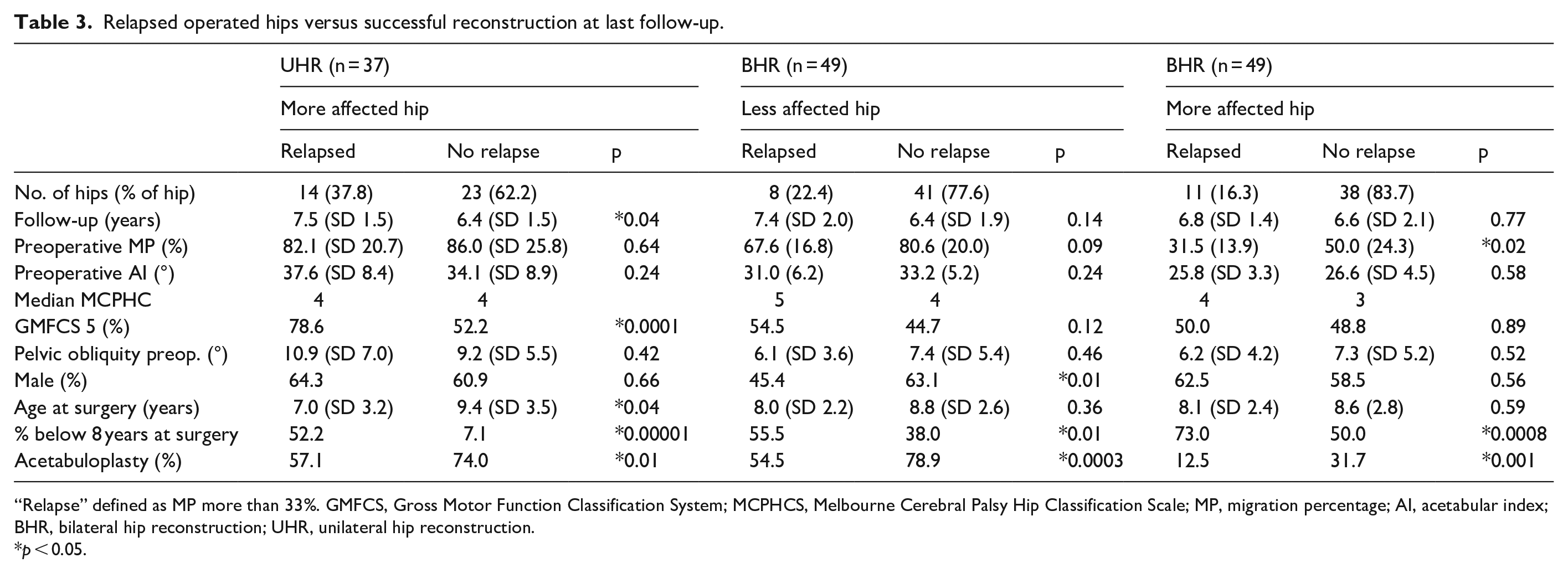
“Relapse” defined as MP more than 33%. GMFCS, Gross Motor Function Classification System; MCPHCS, Melbourne Cerebral Palsy Hip Classification Scale; MP, migration percentage; AI, acetabular index; BHR, bilateral hip reconstruction; UHR, unilateral hip reconstruction.
p < 0.05.
Acetabular reconstruction has been proven to be a protective factor in our series in all groups. In the UHR group, 57.1% of relapsed hips had an acetabular osteotomy, compared with 74% of the non-relapsed hips (p = 0.01). In the BHR group, the results are more statistically significant; in the worse hip, 78.9% of the non-relapsed hips had an acetabular reconstruction compared to only 54% of the relapsed hips (p = 0.0003). In the better hip, 31.7% of the non-relapsed hips had an acetabular osteotomy compared to only 12.5% of the relapsed hips (p = 0.001). Odds ratios (ORs) show this protective effect; for the UHR group, the OR is 0.66 (95% CI 0.16–2.73), for the worse hip in the BHR group, the OR is 0.32 (95% CI 0.08–1.32), and for the better hip in the BHR group, the OR is 0.31 (95% CI 0.03–2.77).
Severity of disease was also found to have a predictive effect for relapse of hips in the UHR group—with a statistically significant difference between the proportion of GMFCS patients (78% GMFCS V in relapsed hips compared to 52.2% in the non-relapsed group, p = 0.0001).
Discussion
The aim of this study was to review outcomes in this large single-unit sample with unilateral and bilateral reconstruction cases to ascertain risk factors for recurrent instability and reoperation, and second, to assess how the less affected hip behaved following operative intervention in each group.
Previous studies have advocated an “à la carte” approach in regard to performing unilateral, or bilateral reconstruction, VDRO alone or in combination with pelvic osteotomy or additional soft-tissue procedures depending on intraoperative findings and patient factors and aimed to provide evidence to guide these preoperative and intraoperative decisions in patients with severe CP affecting the hips, and provide prognostic and predictive tools about the likely postoperative course.16,23
There is no clear consensus on the management of hip dysplasia in patients with CP regarding unilateral or bilateral surgery, though there does seem to be a trend toward bilateral surgery, as both hips are affected by the neuromuscular disease.21,23,24,35 It has been postulated that correcting the deformity in the more severely affected hip alone may increase the risk of progressive deformity in the contralateral hip by reversing the degree of pelvic obliquity and leading to further muscular imbalances across both hips. 23 Owers et al. 23 found a significant improvement in abduction, fixed flexion, and MP in patients treated with bilateral surgery at medium-term follow-up in comparison to patients’ preoperative clinical status. We found, similarly, that more patients who received bilateral reconstruction than UHR had an MP < 33% at their last recorded follow-up.
Hägglund 32 concluded that the high side of pelvic obliquity was associated with higher MP. This is intuitively sensible as the obliquity on the high side simulates an adducted lower leg causing increased adduction contracture and lateral migration of the femoral head. We found no correlation between pelvic obliquity measurements and severity of MP. We did find, however, improvement in pelvic obliquity, and thus sitting balance at last follow-up persisted in those patients who received a bilateral reconstruction. Restoration of the level pelvis, however, did not predict success or failure of the procedure. This is contrary to Shukla et al. 27 who conclude that the reversal of pelvic obliquity was a strong predictor for further hip instability postoperatively.
Our overall recurrence of instability rate in the UHR group was lower than others published. Not all hips with MP > 33% go on to reconstruction, but when revision reconstruction, proximal femoral excision, and reconstruction of the contralateral side in the case of UHR are combined, the reoperation rates differ significantly in our BHR and UHR groups; 13.5% and 43.6% respectively. The overall reoperation rate was 24%.
In our cohort of all operated hips (UHR and BHR), 38 of 135 hips (28%) had an MP of > 33% at last follow-up, with all patients being non-ambulatory, GMFCS IV or V, and 27% of this cohort having unilateral surgery. Studies with lower recurrent instability and reoperation rates tended to have population groups with a lower GMFCS overall, lower preoperative MP, higher rate of bilateral surgery, and higher rate of both acetabular and femoral surgery. Bayusentono et al. 36 had a reoperation rate of 6.5% following initial surgery, with all those undergoing further surgery being graded as GMFCS V. However, 89% of their patients underwent bilateral surgery. It was unclear the indication for reoperation, but they state they aimed for an MP of < 20%. Reidy et al. 37 had a 96.5% rate of MP < 33% after a mean of 5.4 years, with all patients undergoing both acetabular and femoral osteotomies and 42.5% of their population having bilateral surgery. Meanwhile, 27.5% of their population group were ambulatory, compared none of our population group. Huh et al. 16 reported postoperative MP > 30% rates of 33% and 38% for VDRO alone and VDRO combined with additional procedures in which 95% of their study group underwent bilateral surgery. Chang et al. 38 reported a 25% recurrent instability rate postoperatively (MP > 33%).
Rutz et al. 30 had a similar cohort to our study, with 121 patients GMFCS IV or V, with 47 undergoing bilateral surgery. At a mean of 7.3 years, only two patients required surgery for recurrent dislocation. All patients in their population underwent a pelvic osteotomy in the initial surgery. Only the preoperative MP had a significant impact on outcomes, according to an analysis of potential risk factors with the better outcomes in those with less MPs. The cohort had a preoperative MP of an average of 80% in all most affected side hips, similar to our cohort at 81%. Our reoperation rates are much higher, and this could be due to the individual threshold for reoperation, and that the only operation included in the reoperation statistic was a revision of an operated hip. In our study, “reoperation” also included the unoperated hip in UHR cohort. Other studies are more in line with our own findings. Ruzbarsky et al. 39 reported a complication rate of 47.6% which included subsequent instability of an untreated hip (MP > 60%). Shukla et al. 27 had a recurrent instability rate of 51% in patients undergoing unilateral surgery.
Minaie et al. 40 identified acetabular osteotomy and age above 6 years to be protective factors in prevention of relapse instability in all groups of hips reconstructed, which correlates with our results. We also found that surgery at a younger age, below 8 years, correlated with a higher percentage relapse. Due to the progressive nature of migration of the hip in CP, it is recommended that early intervention is performed and so while we would not advocate necessarily waiting till after the age of 8 years but it is important to accept a higher risk of failure and convey this in any discussion with family.
To reduce the occurrence of relapse of the hip following reconstruction, particularly in younger children who have a higher risk of relapse, an abduction brace could be considered, if tolerated, which has been supported in a recent randomized controlled trial. 41
In the literature, the definition of failure is variable. Reidy et al. 37 used an MP of < 30%, Huh et al. 16 used an MP of < 33%, Minaie et al. 40 used an MP > 50%, Ruzbarsky et al. 39 used an MP > 60%, whereas Kamisan and Thamkunanon 26 used an MP > 40%. We have chosen a less conservative MP of > 33% to represent relapse because of the progressive nature of hip deformity in CP. Once a hip is decentered or uncontained, the migration of the hip is very likely to worsening over time.
There are many different radiological parameters that can be used when assessing the hips of patients with CP. MP has been shown to be the most accurate measurement of hip instability in this population group 42 and is the most consistently used in studies of this nature. Difficulty in maintaining a standard radiographic position and plane due to asymmetric contractures, pelvic obliquity, and scoliosis in this cohort of patients makes the measurement of other parameters, such as center-edge angle (CEA), AI, and neck-shaft angle (NSA), difficult. 23 Furthermore, radiographs postoperatively are taken in a brace or hip spica, also affecting measurements; therefore, it was felt that the most useful radiographs for measurement would be those taken on the final preoperative clinic appointment and the last recorded follow-up clinical appointment, to ensure consistency of the record.
The Rutz et al. 30 classification can be used to classify the shape of the femoral head. Kasprzyk et al. 43 reported that while it is reliable (showing moderate-to-substantial intra- and interobserver reliability (mean κ = 0.64 and mean κ = 0.5, respectively)), clinical utility of this classification system is yet to be established in the literature. This radiological classification system was therefore not used in our study. Of note, Rutz et al. 30 found that femoral head shape was not an independent predictor of outcome of reconstruction. Recent papers Kasprzyk et al. 43 and Ulusaloglu et al. 44 report that the grade of femoral head shape was significantly associated with increasing MP.
Computerized tomography (CT) was not routinely used in this cohort due to radiation risk. Some authors advocate the use of CT when planning hip reconstruction surgery.30,42 Chung et al., 45 however, reported physical examination to determine femoral anteversion and the NSA can likely replace CT examination, rendering the radiation exposure harder to justify.
Kamisan and Thamkunanon 26 report 33.3% of patients had contralateral hip subluxation in the UHR cohort, compared to 35.1% in our cohort (their threshold for subluxation was slightly higher at 40% MP). Of their unilateral reconstruction group, the contralateral hip subluxed during follow-up in 21.6% of patients, compared with 20.8% in our cohort. 26 Our findings in the UHR group strongly support those of Kamisan and Thamkunanon. 26 They report only one recurrent instability of 42 patients (2.4%), and no recurrent instability in the less affected hip in the BHR group. Our results show a 16.3% recurrent instability rate of the less affected hip in BHR group. This difference may be explained by our lower threshold for the definition of subluxation, 33% MP versus their 40% MP; a longer follow-up of a minimum of 4 years in our group versus an average of 38 months in their UHR groups and 40 months in their BHR group; and the larger sample size of our cohort.
The decision to proceed to an open reduction was made intraoperatively on EUA if it was found that the hip did not reduce well into the acetabulum. This was uncommon. The rate of open reduction in hip reconstruction in CP is not well documented in the literature and practice is varied. Of comparable studies, Kamisan and Thamkunanon 26 use the same criteria for proceeding to open reduction but do not state their open reduction rate. Rutz et al. 30 also performed open reduction only when necessary and did not state the rate of open reduction in their cohort, but did use open versus closed reduction within their cofounders group for statistical analysis. In our cohort, and in the cohorts reported on by Kamisan and Thamkunanon 26 and Rutz et al., 30 open reduction was not found to be a risk or protective factor for relapse of femoral head migration. Open reduction could be considered a marker of severity in our cohort, correlating well with higher MCPHCS with all hips requiring an open reduction having an MP of over 100% preoperatively. Rutz et al. 30 had a much lower reoperation rate in a similar population group to the current review, and open reduction rates are potentially another cause for this. A larger cohort, however, would be necessary to assess whether an open reduction is truly protective for relapse following hip reconstruction.
Limitations of this study include its retrospective nature, lack of functional scores used, or preoperative and postoperative pain scores. However, this is one of the largest series in the literature, with all cases using the same preoperative and intraoperative treatment algorithm.
Conclusion
This study is to date the largest involving hip reconstruction of pediatric CP patients using a reproducible treatment algorithm, comparing UHR and BHR. It adds to a growing body of evidence that bilateral surgery may lead to both a decreased incidence of postoperative recurrent hip instability and reoperation.
Decision-making between UHR and BHR should be made in conjunction with carers and the child as far as possible. We advocate that discussion should be formalized when MP is > 33%. If the contralateral hip has an MP of > 33%, both hips should be reconstructed. If the contralateral hip has an MP of < 33%, pelvic obliquity and adduction contracture should be taken into consideration to make a decision regarding whether to proceed with UHR or BHR. Severity of disease and age at the time of surgery should also be considered when counseling the patient and carers. Our data reveal that reconstruction is best performed after 8 years of age, to decrease the risk of recurrent instability. Our data also strongly suggest that there should be a low threshold for the use of an acetabular osteotomy.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521231196846 – Supplemental material for Hip reconstruction in cerebral palsy: Lessons from a single center and 137 hips
Supplemental material, sj-pdf-1-cho-10.1177_18632521231196846 for Hip reconstruction in cerebral palsy: Lessons from a single center and 137 hips by Anoushka Ayub, Christy Graff, Lajos Maurovich Horvat and Claudia Maizen in Journal of Children’s Orthopaedics
Footnotes
Acknowledgements
The authors thank Dr Anna Bridgens and Dr Babar Kayani for their contribution to this article. They also thank Mr John Paterson for his significant contribution.
Author contributions
A.A. (FRCS, MSc) contributed in data acquisition, analysis and interpretation of data, and writing of the article. C.G. (MHMSc, FRCS) involved in study design, data acquisition, analysis and interpretation of data, and writing of the article. L.M.H. participated in data analysis and interpretation of data. C.M. contributed in study design, data analysis, and writing of the article.
Data availability
Raw data are readily available through the first author and corresponding author on request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical statement
No ethical application was needed due to the retrospective nature of the study.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.