
Abstract
Purpose
Treatment of idiopathic clubfoot with the Ponseti method is now standard, but predicting relapse can be difficult. Most experts recommend bracing to the age of four years, but this can be challenging for families, and may not be necessary in all patients. The purpose of this study is to compare patterns of bracing and age of relapse to help determine if predictable patterns exist.
Methods
The 70 patients with idiopathic clubfoot treated initially with the Ponseti technique who had relapse of their clubfoot were identified. Relapse was defined as a return to casting or surgery due to recurrent deformity. Data collected included demographics, treatment and brace adherence. Patients who sustained initial relapse before the age of two years were compared with those who sustained initial relapse after the age of two years.
Results
In total 56% (39/70) had their initial relapse prior to age two years while 44% (31/70) were after age two years. Of the patients who relapsed prior to the age of two years, 28% (11/39) were adherent with bracing while 72% were non-adherent. For patients who initially relapsed after age two, 74% (23/31) were adherent with bracing while 26% were non-adherent (p < 0.001). Of those who had initial relapse prior to age two, a subsequent relapse was seen in 69% (27/39).
Conclusion
Patients with idiopathic clubfoot who experienced recurrence prior to age two years are significantly more likely to be non-adherent with bracing than those who sustain recurrence after age two. After initial relapse prior to age two, bracing adherence does not affect likelihood of subsequent recurrence.
Purpose
Treatment of idiopathic clubfoot by the Ponseti method is now standard, and most feet can achieve satisfactory initial correction using this technique. 1 However, subsequent treatment to maintain correction of the deformity with prolonged bracing can be difficult at times, 2 and recurrence rates requiring further procedures are 20% to 40% even in the best of hands.1,3–7
After initial correction, adherence with the foot abduction brace program is important. Ponseti himself changed his recommendations about the length of bracing during his career from two years 5 to six years,5,8 however, most practitioners are currently recommending bracing until age four.9–11 This can be challenging for some families, 2 and it is unclear whether it is necessary for all patients. Several previous studies have found that recurrence (or relapse) of clubfoot is most influenced by lack of adherence with the bracing programme,3,6,12,13 however, the factors that influence recurrence at varying ages have not been fully assessed. That is, does recurrence after the age of two years have different influences than recurrence prior to age two years?
The purpose of this study is to retrospectively review patients with idiopathic clubfoot who have experienced recurrence (or relapse) of their clubfoot after initial correction, to determine if factors predictive of recurrence change as the child matures. Specifically, we compared patients who had initial relapse prior to age two with those with initial relapse after age two. Furthermore, we wish to assess the influence of other factors, such as deformity triggering recurrence, brace used and treatment on age at recurrence.
Methods
This was a retrospective study of patients with idiopathic clubfoot who had sustained a recurrence of their clubfoot deformity. All included patients had initial clubfoot treatment using the Ponseti method started at our institution when they were less than four-weeks-old, and all had initial satisfactory correction of their clubfoot by casting and +/- tenotomy. Three different fellowship trained paediatric orthopaedic surgeons were involved in the care of these patients, and casting was done with direct involvement of the surgeon in all cases. Patients were identified through our clubfoot registry as treated for recurrence between 2006 and 2015. Recurrence or relapse was defined as return to casting or surgery after treatment of the initial deformity and initiation of bracing. Our department rate of relapse during this time is around 27% (based on internal quality monitoring records). If a repeat tenotomy was needed as part of the initial deformity correction this was not included as recurrence. Casting performed to maintain correction while awaiting a brace order was not included as recurrence. Surgery done to correct simple toe deformity was not included as recurrence. Recurrence, for the purposes of this study, was defined by patient, not by foot; because abduction bracing (or lack of bracing) applies to both feet equally. Exclusion criteria were: non-idiopathic clubfoot; bulk of treatment prior to recurrence at an outside institution; and clubfoot treatment initiated at over one year of age. If the patient had initial clubfoot treatment (e.g. the first one to two casts) at a different institution before transferring their care here, they were included; if their care was transferred here after more significant treatment from the outside institution then they were not included.
Initial demographic and treatment data on all patients were collected, including birthdate, gender, surgeon, side(s) of involvement, initial pre-treatment Dimeglio classification 14 (as available, from our institution only), date of tenotomy if done and type of initial brace. Also collected was the age at first recurrence, treatment for first recurrence, deformity triggering recurrence, treatment performed for recurrence, whether any subsequent recurrence or treatment was needed and age occurred and date patient was most recently seen. Age at initial recurrence was noted at the time of either placement of first corrective cast or scheduling for surgery. Subsequent treatments and ages occurred were also noted. If bilateral Dimeglio scores were noted, comparisons were drawn from the patient's greater (more severe) score.
Bracing adherence data was collected on all patients and was carefully assessed by the primary author based on the available clinic notes. ‘Adherence’ was defined as wearing the foot abduction brace without issues most of the time, as reported by the parents. ‘Difficulties’ with brace wear were noted and not considered adherence, were combined with ‘lack of brace wear’ which could be due to self-discontinuance of the brace, or as prescribed by the provider. As bracing non-adherence often occurs concurrently with relapse, it can be difficult to assign causality. For our cohort, if a patient was first identified as having difficulty with bracing at the same time as they were identified as having relapse, they were not considered ‘non-adherent with bracing’, provided they were otherwise adherent. Bracing adherence was assessed in intervals, and any significant time (more than a few days) out of bracing adherence was counted as lack of adherence for the whole interval. Intervals assessed were: up to six months, six to 12 months, 12 to 18 months, 18 to 24 months, 24 to 36 months and 36 to 48 months of age. Bracing recommendations during this time changed along with the recommendations of Ponseti5,8 from two years to four years of age. Thus, some patients stopped bracing at two years of bracing as per recommendations of the surgeon (the patients born prior to 2006) and some stopped bracing prior to age four years (patients born in 2006 or afterwards) despite recommendations of the surgeon to continue. Patients whose recurrence was treated with casting +/- tenotomy or tendo-Achilles lengthening (TAL) were returned to the bracing regime. Ongoing compliance with bracing after first recurrence was noted.
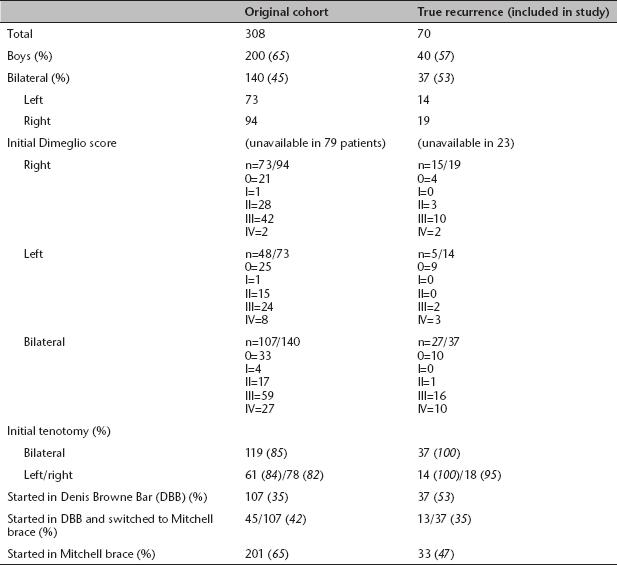
Recurrence was confirmed on all patients, and data was collected on those included. The initial query from the clubfoot registry of 308 patients with idiopathic clubfoot identified 91 patients with recurrence. After applying exclusion criteria and confirming true recurrence, 70 patients remained, which constitutes the cohort for the study. Comparisons between the initial clubfoot registry query and those identified with recurrence are noted (Table 1). Mean length of follow-up for the cohort is 8.0 years (standard deviation (sd) 3.0). Patients with initial recommendations of bracing to age two-years-old (born prior to 2006) were compared with those with initial recommendations of bracing to age four-years-old (born during or after 2006).
Comparisons between the original cohort of all idiopathic clubfoot patients and those with true recurrence. The true recurrence group constituted those that were primarily studied in this project.
Data were collected as dichotomous (gender), continuous (age, age at recurrence), categorical (surgeon, side, type of brace, adherence with bracing, deformity noted at recurrence, treatment for recurrence, pre-treatment Dimeglio score). Type of recurrence was divided as follows: patients who recurred prior to age two years but were adherent with bracing; patients who recurred prior to age two and had bracing challenges; patients who recurred after age two but were adherent with bracing at least up to age two; and patients who recurred after age two and had bracing challenges.
Data was compared using Excel (Microsoft, Redmond, Washington) and GraphPad Prism 6.0 for Mac OS (GraphPad Software, La Jolla, California). Fisher's exact test was used for dichotomous data, Student's t-test for continuous data and analysis of variance for multiple comparisons. Statistical significance was set a priori at p < 0.05, two tailed.
Results
Using our clubfoot database, 308 patients were initially identified as having idiopathic clubfoot treated using the Ponseti method. Of those, 70 patients were identified who sustained relapse of their clubfoot and met the inclusion criteria for the study. See Table 1 for comparisons between the original cohort and those studied in this paper for true recurrence.
For the 70 patients identified as having a recurrence, the mean age at initial recurrence was 31 months (sd 24). In all, 56% (39/70) sustained their first recurrence at or before 24 months of age at a mean age of 12 months (sd 5.8). In all, 44% (31/70) sustained their first recurrence after age 24 months at a mean age of 54 months (sd 16.8).
There was no significant difference in deformity triggering recurrence with regards to bracing compliance. For treatment of their initial recurrence, the cast only was done in 34% (24/70), tenotomy or TAL (with or without pre-operative casting) was done in 40% (28/70), anterior tibialis tendon transfer (with or without TAL and/or pre-operative casting) was done in 17% (12/70) while capsular release (medial and/or lateral) was done in 9% (6/70) (Table 2). Of this group of patients who sustained at least an initial recurrence, 51% (36/70) sustained a second recurrence (Table 2).
Initial treatment for recurrence in patients who had a second recurrence.
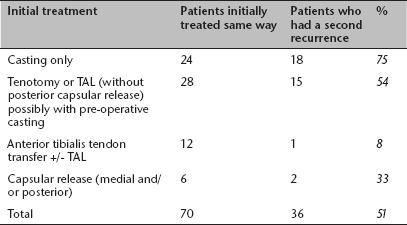
TAL, tendo-Achilles lengthening
Patients who sustained their first relapse prior to age two years were significantly different in bracing adherence than those who sustained their first relapse after age two years. Similarly, the deformity triggering recurrence (p < 0.001) and the treatment for recurrence (p < 0.01) were also different between the two age groups (Table 3). There was no difference in pre-treatment Dimeglio score. There was no difference in treatment for patients who complied with bracing compared with those who did not comply with bracing (chi-square, p > 0.05). There was no difference in age at first recurrence when stratified by the type of brace used or gender.
Comparison between patients who sustained initial recurrence before the age of two years with those who sustained initial recurrence after the age of two years. There was no difference in pre-treatment Dimeglio score between the groups.
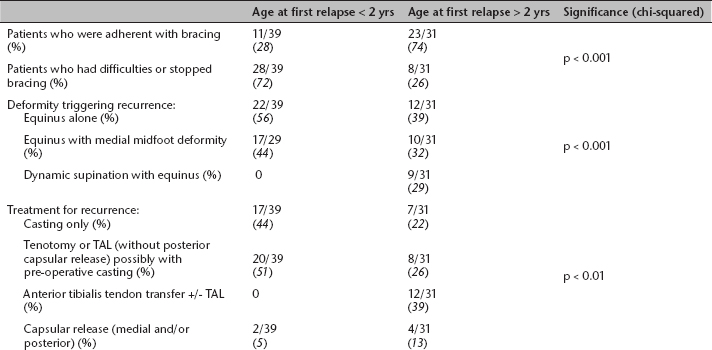
TAL, tendo-Achilles lengthening
Of those patients who had initial relapse prior to age two years, a subsequent relapse was seen in 69% (27/39). If a patient was adherent with bracing, subsequent relapse occurred in 64% (7/11), while if a patient was non-adherent with bracing, subsequent relapse occurred in 71% (20/28). This difference between groups was not statistically significant (p = 0.7).
Patients who were recommended to continue bracing up to two years of age (those born before 2006) were compared with those recommended to continue bracing up to four years of age (those born during or after 2006). There was a significant increase in recurrence rate in those initially prescribed bracing until only two years of age, but no difference in age at initial recurrence (Table 4).
Comparisons between patients who initially were prescribed brace treatment until two years of age and those who initially were prescribed brace treatment until four years of age.

NS, not significant
Conclusion
Treatment of idiopathic clubfoot can be challenging. Long-term outcomes studies have shown the Ponseti method of treatment to be superior to prior surgical techniques, 15 which has resulted in the majority of providers who treat clubfeet switching to the Ponseti method. 1 While most patients with clubfeet can achieve satisfactory initial correction, maintaining that correction during early childhood can be challenging in some.4,13,16 Adherence with the foot-abduction brace has been shown in multiple studies to decrease likelihood of recurrence, however, adherence with bracing does not guarantee successful long-term correction.3,6,10,13,17 Despite adherent bracing, some feet seem almost destined to relapse, whereas poorly braced feet sometimes maintain correction over the long term. 18 The age of relapse as it relates to predictors of relapse or recurrence has not been previously studied; this is the first study assessing different patterns of recurrence of idiopathic clubfoot based on age. We found that patients who relapse under the age of two years were more likely to be non-adherent with the bracing programme, while patients over the age of two years who experienced relapse were more likely to be adherent with the bracing programme, despite being older and having had more time to develop an inconsistent pattern (p < 0.001). This study only assessed patients who had already sustained recurrence; our department recurrence rate was about 27% during this time, which is in line with published reports.1,4,6,19,20 We also found that pre-treatment Dimeglio score was not different in those patients who sustained relapse prior to age two years and those who sustained relapse after age two; furthermore, Dimeglio score was not different in patients who were adherent with bracing compared with those who were not. We did find also that patients whose initial physician recommendations were to brace for four years had a significantly lower recurrence rate than those who were told initially they were expected to brace until the age of two years.
Some authors have noted differences in recurrence based on age, typically based on presentation of that recurrence,10,21 however, data showing differential brace adherence had not been demonstrated. We had a relatively even distribution of gender in our study, which was somewhat surprising given the typically higher rate of idiopathic clubfoot in male children. Goldstein et al 13 noted that female gender was a risk factor for relapse, which may explain the gender equality in our study of patients who have relapsed.
Previous studies have noted recurrence rates after anterior tibialis tendon transfer (ATT) to be as high as 20%. 3 While our rate of recurrence after ATT is lower (8%), we did not perform ATT in patients under the age of two years, and younger age at ATT was found to be a risk factor for recurrence after that procedure. 3
Known predictors of recurrence after successful correction with the Ponseti technique include brace non-adherence,6,13 female gender, 13 higher initial pre-treatment Dimeglio score, 13 poor everter muscle activity, 22 and level of parental education. 12 Everter muscle activity was not reliably commented on in the clinical notes, thus could not be assessed in this study. Our study found no difference in pre-treatment Dimeglio score based on age at recurrence, or difference in pre-treatment Dimeglio score based on bracing adherence, however, this study was only of patients who had already sustained recurrence.
The primary weakness of this study was the retrospective nature. Bracing adherence (or not) was based on the established clinical notes and the best available interpretation of the medical record. Everter muscle function was not able to be assessed because it was not reliably commented on in the clinical notes, and the occurrence of relapse was based on the individual clinician's opinion and treatment plan at the time and not based on pre-established criteria. We also had changing treatment algorithms and expectations regarding bracing during this time. This study does include many idiopathic clubfoot patients who have sustained a recurrence, and we feel that this data is nonetheless valuable.
In the treatment of idiopathic clubfoot, there is often a discussion around whether lack of bracing adherence is because of the ‘foot’ or the ‘family’. While it is clear that bracing is important to the maintenance of correction of clubfoot,21,23 some clubfeet seem more ‘destined’ to recur 18 than others. While current recommendations for bracing are until the age of four years for all patients with idiopathic clubfoot,10,11 with a better understanding of the factors predictive of recurrence we may be able to customise treatment and lessen the bracing burden on patients and families for those less likely to recur. In the children who sustain initial recurrence under the age of two years, we found a high rate of subsequent, or second relapse (69%). This likely reflects that treatment for recurrence at the age of two years consists typically of repeat casting and possible tenotomy. Since this group had difficulties with bracing initially, it is not surprising they demonstrate such a high rate of subsequent relapse: perhaps in these cases the problem is most likely to be the foot, not the family or the brace. It is also surprising that subsequent relapse in this group seemed independent of bracing compliance, again suggesting that the foot itself may be the driver of recurrence. In our study, we found that initial Dimeglio score was not associated with recurrence. While the initial severity is one factor, perhaps more important is whether there is an ongoing driver of the deformity contributing to recurrence in some feet. Certainly, further exploration in this regard is warranted.
In conclusion, patients with idiopathic clubfoot treated with the Ponseti method who sustain recurrence prior to the age of two years are significantly more likely to be non-adherent with bracing than those who sustain recurrence after the age of two years. We found that after initial relapse prior to age two years, bracing adherence does not appear to affect the likelihood of subsequent recurrence. Bracing adherence as part of Ponseti treatment for idiopathic clubfoot remains important. Relapse prior to the age of two years appears to be more related to bracing adherence than relapse after the age of two years. Further work on identifying clubfeet that are at high or low risk to relapse may result in modifications of the bracing recommendations.
Footnotes
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.