
Abstract
Purpose:
To investigate the value of antero-posterior and lateral radiographs in predicting clubfoot relapse after treatment with the Ponseti method.
Methods:
This was a retrospective review of 104 children (157 feet) younger than 3 months of age with idiopathic clubfoot treated using the Ponseti method at our institution between January 2007 and December 2014. All patients underwent Achilles tenotomy and were divided into two groups according to the need for further surgery to correct the deformity: relapsed group (24 patients; 36 feet) and non-relapsed group (80 patients; 121 feet). All antero-posterior and lateral foot radiographs were performed less than 3 months after Achilles tenotomy. The talo-calcaneal (TC-AP) and talus-first metatarsal (TM-AP) angles were measured in the antero-posterior view, while the tibio-calcaneal (TIC-L), talus-first metatarsal (TM-L), and talo-calcaneal (TC-L) angles were measured in the lateral view. The multi-factor logistic regression model of the stepwise selection method was used to predict the relapse of clubfoot deformity from the potential predictive values.
Results:
The mean age at initial plain radiography examination was 99.45 ± 21.54 days. Differences in TC-AP, TM-AP, TC-L, and TIC-L between the two groups were statistically significant. However, only TM-AP and TIC-L were included in the “risk of relapse” formula using the multi-factor logistic stepwise selection method.
Conclusion:
Early antero-posterior and lateral radiographs in children younger than 3 months of age at initial Ponseti treatment have positive predictive value for relapse. Reduced TM-AP angle and increased TIC-L were associated with an increased risk of relapse.
Level of evidence:
level III.
Keywords
Introduction
Idiopathic congenital talipes equinovarus or idiopathic clubfoot (IC) is a complex but relatively common foot deformity with a prevalence of 0.5–6.8 per 1000 birth.1,2
The Ponseti technique has been widely recognized as the most effective treatment option for children with IC, with an initial correction rate exceeding 90% in most published studies.3–5 Percutaneous Achilles tenotomy is performed in most cases to correct the residual equinus at the end of the cast treatment. Children then wear foot abduction orthosis (FAO) until the age of 4 years to prevent recurrence. 3 Despite the excellent initial correction rates, relapse of the deformity is not uncommon, occurring in up to 67.3% of cases.4–6
The outcome of the Ponseti technique is primarily assessed with clinical and functional tools such as Dimeglio’s and/or Pirani’s clinical score systems.7,8 However, these clinical scoring systems are subjective and do not consider any imaging modality. 9 Imaging methods, such as radiography, are objective and relatively simple to obtain. Radiographs can show the anatomy, position, and interrelationships of the different bones of the foot. However, whether antero-posterior (AP) and lateral radiographs should be routinely performed in patients with IC remains controversial. Kang and Park 10 and Radler et al. 11 found that the lateral tibio-calcaneal (TIC-L) angle is a reliable prognostic indicator for percutaneous Achilles tenotomy. Shabtai et al. 12 reported that lateral radiographs with the foot in maximal dorsiflexion are the most useful for detecting abnormalities in Ponseti-treated clubfeet. Similarly, Li et al. 13 investigated the early radiographic changes in the lateral talo-calcaneal (TC-L) angle following Achilles tenotomy in children with IC. On the contrary, Richards et al. 14 reported that the standing TIC-L and TC-L angles on lateral radiographs in patients aged 18–24 months were not helpful in predicting future relapse. Moreover, according to Ponseti and colleagues,15–17 plain radiographs are not recommended for follow-up of patients treated with serial casting. On the other hand, Simons 18 highlighted the importance of plain radiographs to understand the anatomy of the clubfoot deformity and to evaluate the effect of its treatment.
The main goal of our study was to assess whether initial AP and lateral radiographs are predictive of clubfoot relapse requiring surgical intervention in children treated with the Ponseti method.
Materials and methods
Patients
This study was approved by the institutional review board of our institution (138A01).
All patients with IC treated at our institution between January 2007 and December 2014 were reviewed. All patients were admitted through a dedicated clubfoot outpatient clinic, and the following data were recorded: sex, age, race, side affected, family history, and associated congenital abnormalities. Only children with a confirmed diagnosis of IC younger than 90 days at the time of first cast application and who had not received any previous orthopedic treatment were included in the study, as well as patients who (1) had to undergo AP and lateral foot radiographs less than 3 months after Achilles tendon lengthening, (2) had to wear the FAO up to 4 years of age, and (3) had to have at least 7 years of clinical follow-up. Additional information such as the severity of the deformity according to Dimeglio’s and Pirani’s classification systems,7,8 number of casts, total time in cast, need for percutaneous Achilles tenotomy, adherence with post-correction brace, complications, relapses, and need for further surgical interventions was collected from the charts.
Exclusion criteria were positional clubfoot, non-IC, prior failed treatment, noncompliance with FAO requirements, and clinical follow-up of less than 7 years.
Treatment protocols
All patients were treated according to the Ponseti method. The cast was changed weekly in an outpatient clinic. At the end of cast treatment, if ankle dorsiflexion was less than 0°–5°, a percutaneous Achilles tenotomy under general anesthesia followed by 3 weeks of additional cast was performed. After completion of treatment, FAO was applied full-time to all patients; FAO treatment was subsequently adjusted to age and walking abilities of the patient as suggested by Ponseti and colleagues.15–17 In particular, the splints are worn 23 h a day for 3 months, and then the number of hours per day decreases by 4 h after 3 months over a period of six additional months; at this stage, FAO is worn during nighttime and naps (10–12 h/day) until the child is 4 years of age. All the patients were treated according to the same protocol by the same surgical team.
Brace compliance was assessed subjectively according to parents or guardian reports. In particular, patients younger than 12 months of age had a follow-up visit scheduled every 3 months (four reports about brace compliance per year), while patients older than 12 months of age had an appointment with the surgeon twice a year (two reports about brace compliance per year).
Although there is no agreement among scientists, in this study relapse was defined as the reappearance of any of the components of the clubfoot deformity, including equinus, forefoot adduction, hindfoot varus, or cavus, and the need for surgical intervention during the follow-up in or out of the bracing phase.
Plain radiographs
All AP and lateral foot radiographs were performed less than 3 months after Achilles tenotomy. In particular, an AP radiograph of both feet and a lateral radiograph of the foot and ankle with the foot in maximum dorsiflexion were performed in all patients (unilateral and bilateral cases).11,18
The AP radiograph of the foot was used to measure the talo-calcaneal (TC-AP) and talus-first metatarsal (TM-AP) angles, while the TIC-L, talus-first metatarsal (TM-L), and TC-L angles were measured in the lateral view (Figure 1). To identify the longitudinal axis of the talus, two points at the top and bottom edges of the bone were selected, and the midpoints between the top and bottom points were identified, as described by Li et al. 13 The longitudinal axis of the tibia, calcaneus, and first metatarsal was determined using the same method. 13 All angle measurements were performed using Auto CAD 2019 software Autodesk (San Rafael, USA).
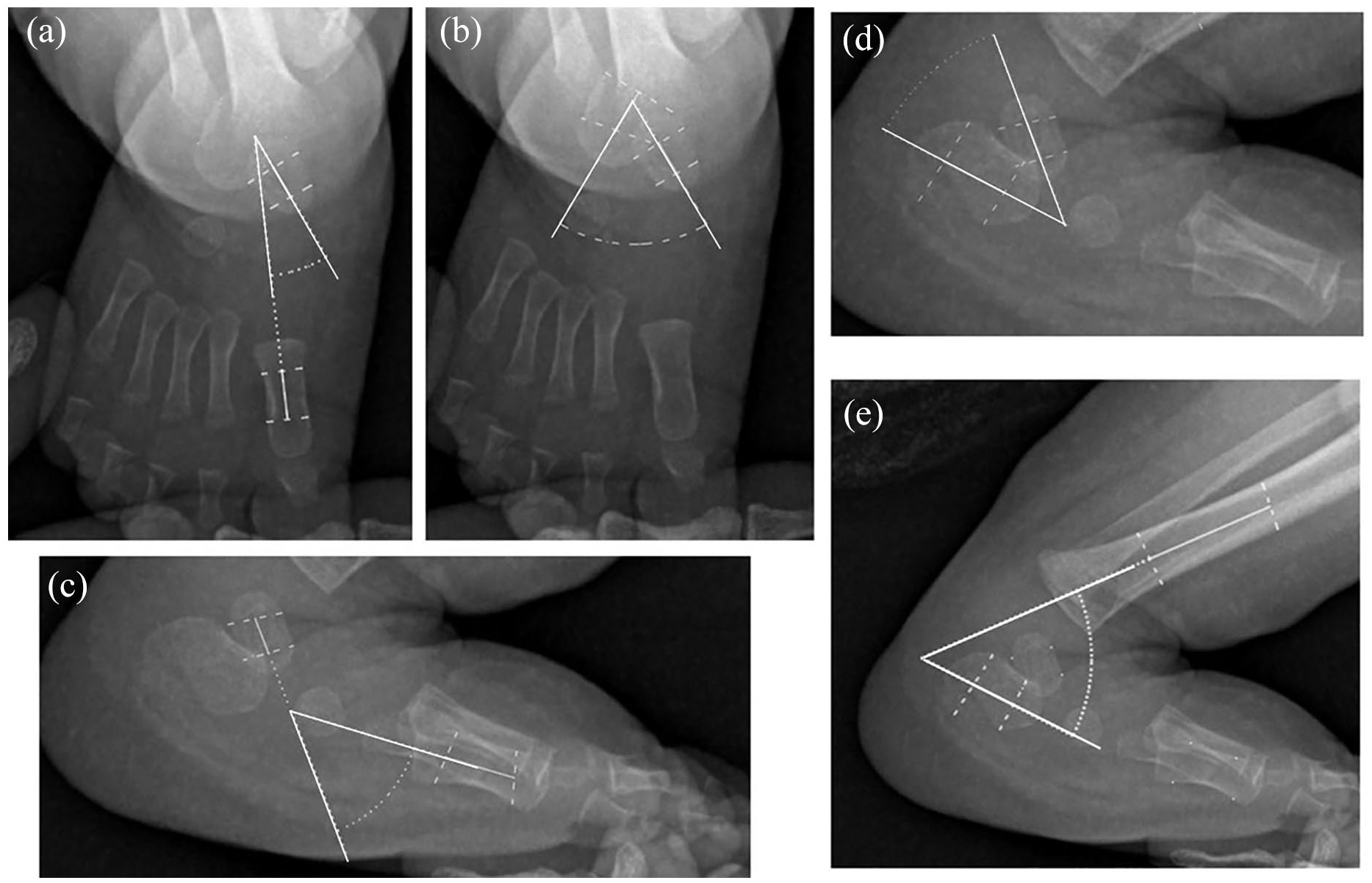
Radiographic measurements: (a) talus-first metatarsal (TM-AP) angle; (b) talo-calcaneal (TC-AP) angle; (c) talus-first metatarsal (TM-L) angle; (d) talo-calcaneal (TC-L) angle; (e) tibio-calcaneal (TIC-L) angle.
The angles (n = 5) of 30 randomly selected patients were measured at 3-week intervals by two independent observers who were not involved in the care of any of the patients (C.C.X. and J.C.L.). The intraclass correlation coefficients (ICCs) for correlated data were calculated to evaluate interobserver reliability at the first rating and intraobserver reliability between the first and second ratings. According to the usual recommendations, the concordance was examined as follows: <0.2, bad; 0.2–0.4, low; 0.4–0.6, moderate; 0.6–0.8, good; and >0.8, excellent.19,20
Statistical analysis
Statistical analysis was performed using SAS software (version 9.4; SAS Institute, Cary, NC, USA). Data are presented as mean ± standard deviation or median (interquartile range) according to the statistical distribution. Descriptive statistical analysis and testing for normal distribution using the Kolmogorov–Smirnov test were performed for both groups. The difference in each angle between the recurrent and non-recurrent groups was compared using t-tests or the chi-square test according to the statistical distribution. Unconditional logistics regression was used to evaluate the predictive value of the angles. Statistical significance was set at p < 0.05.
Results
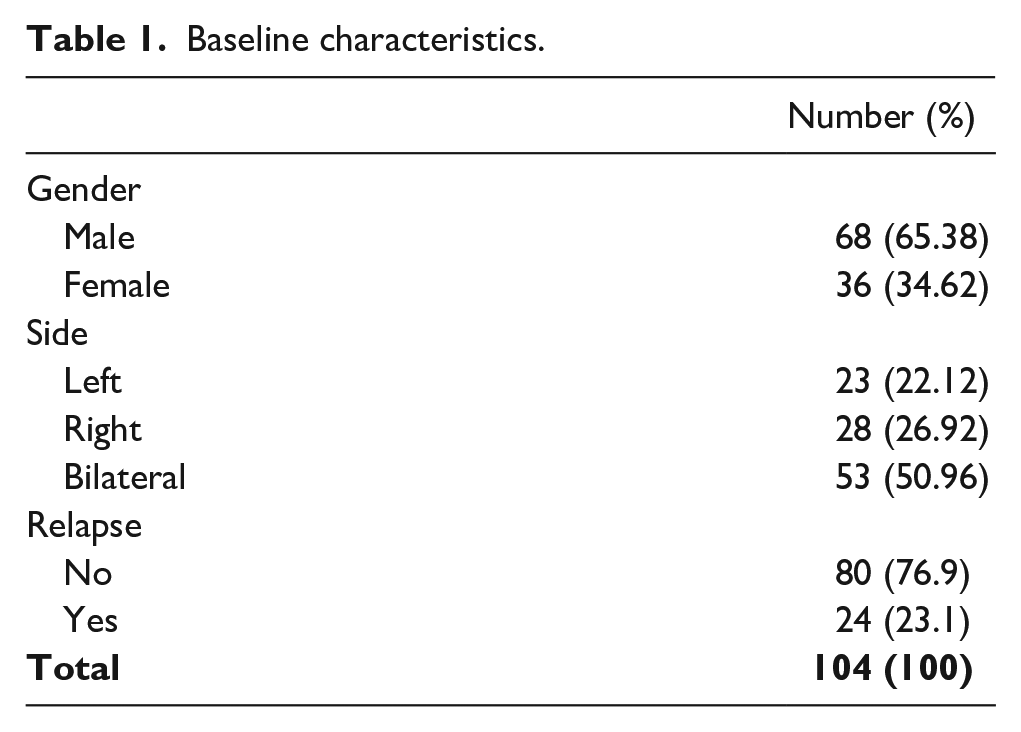
A total of 104 children with IC (157 feet) were included in the study. Figure 2 summarizes the flowchart of the case-selection process (Figure 2). There were 68 males (65.4%) and 36 females (34.6%), and the deformity was bilateral in 53 patients and unilateral in the remaining 51 (left 23, right 28) (Table 1).
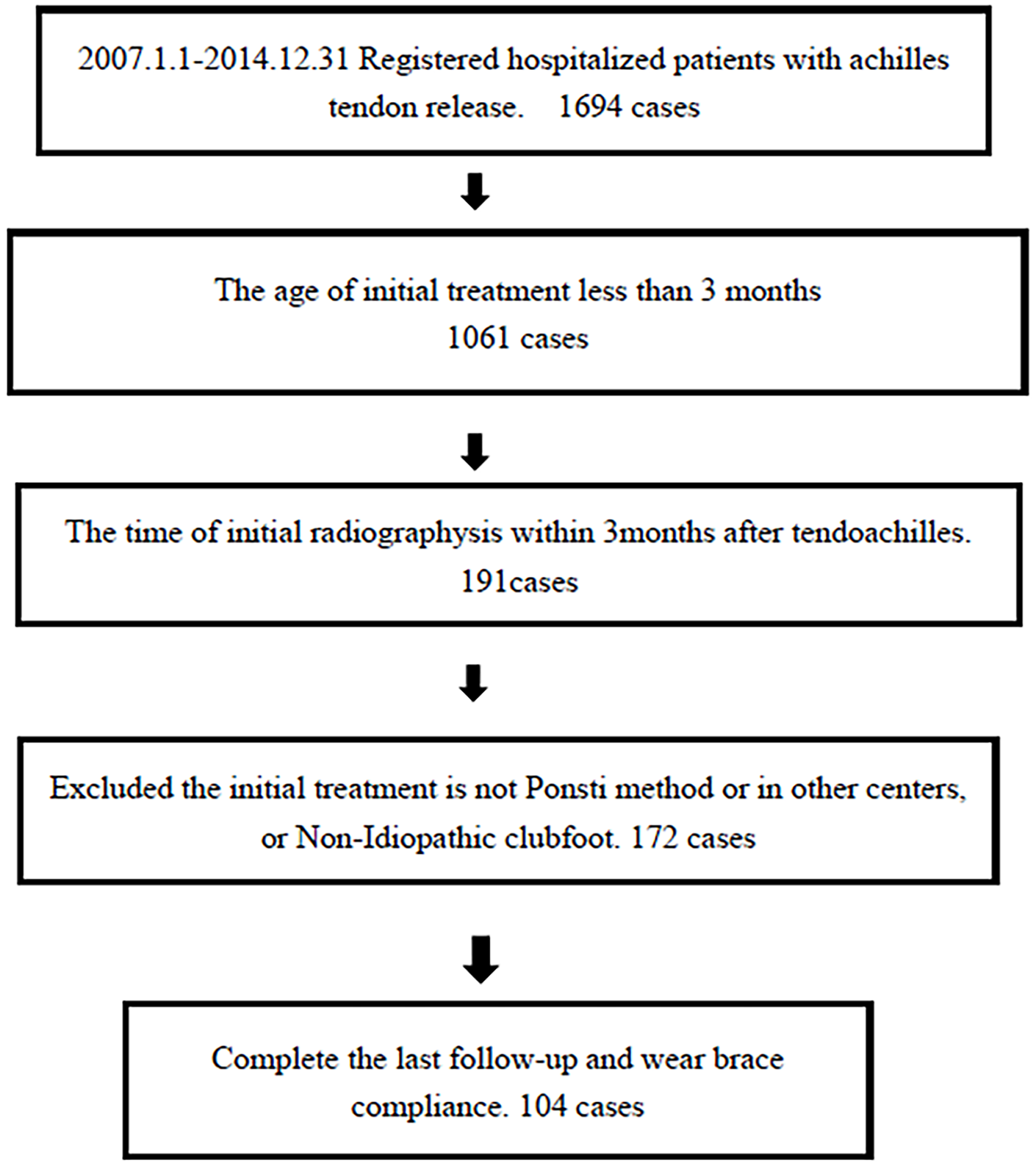
Flowchart of patients’ selection.
Baseline characteristics.
The mean age at the time of first cast was 10 days (range, 4–56 days), the mean Pirani score was 5.2 points (range, 4–6), and the mean Dimeglio score was 10.2 points (range, 8–18). The mean age at Achilles tenotomy was 58.02 ± 18.48 days (range, 28–98 days), while the mean age at initial AP and lateral foot radiographs was 99.45 ± 21.54 days (range, 55–150 days) (Table 2).
Comparison between the relapsed group and non-relapsed group (baseline characteristics).
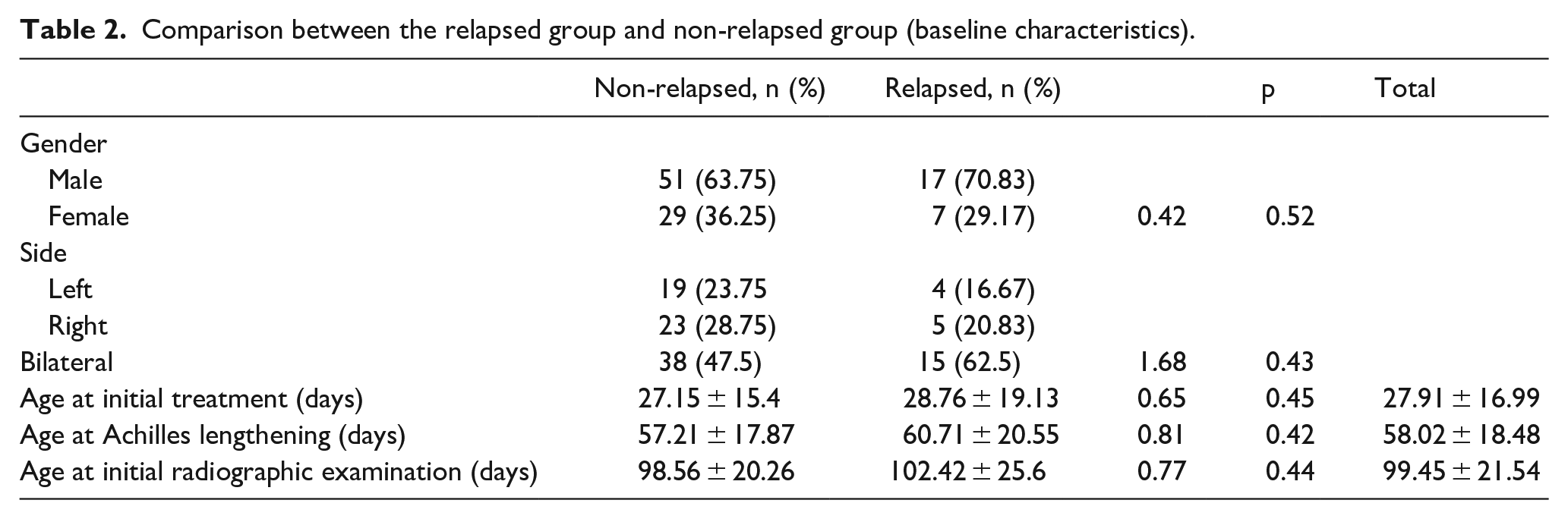
A total of 24 out of 104 patients (36 feet; 23.1%) relapsed (relapsed group) and required further surgery in order to correct the deformity. The mean age of patients at the time of relapse was 6.07 ± 1.85 years (range, 2.84–10.16 years). On the other hand, 80 out of 104 patients (121 feet; 76.9%) had no recurrence (non-relapsed group). There was no significant difference between the non-relapsed group and relapsed group in terms of sex, affected side, initial treatment age, age at Achilles tendon lengthening, or age at initial radiographic examination (Table 2). Table 3 highlights all patients who required further surgery to correct the deformity (Table 3); among patients with bilateral clubfoot, any case of bilateral relapse was recorded.
Patients with relapse.
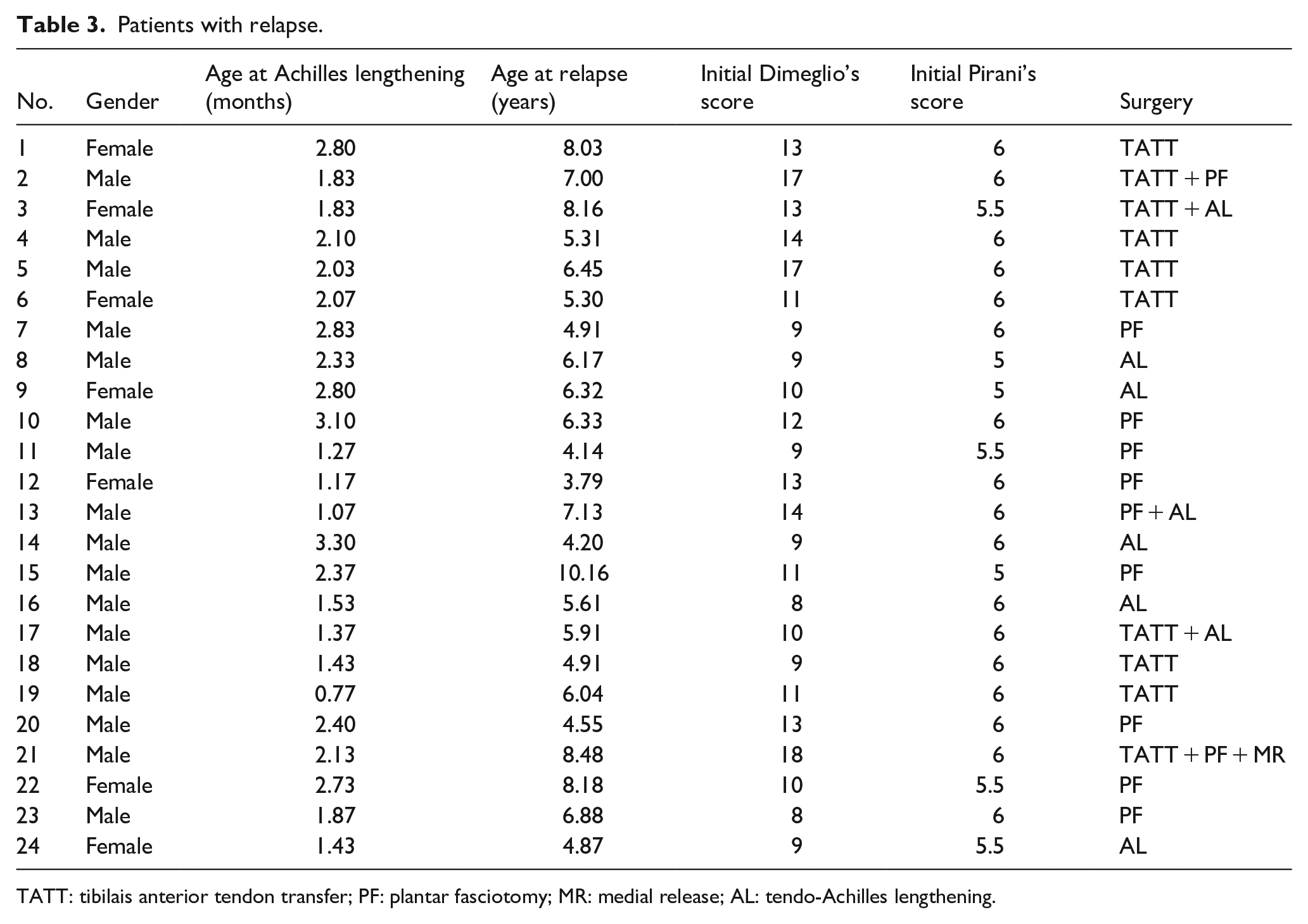
TATT: tibilais anterior tendon transfer; PF: plantar fasciotomy; MR: medial release; AL: tendo-Achilles lengthening.
The interobserver and intraobserver reliability of each angle was studied. The ICCs were rated “excellent” for most angles with regard to interobserver and intraobserver reliability.19,20 The ICC for intraobserver reliability was rated as “good” for the TC-L angle (0.79) and “excellent” for all other angles. The average ICC for the interobserver reliability was “excellent” for all angles except the TC-AP angle (good: 0.77) (Table 4).
ICCs for intra- and interobserver accuracy of radiographic measurements.
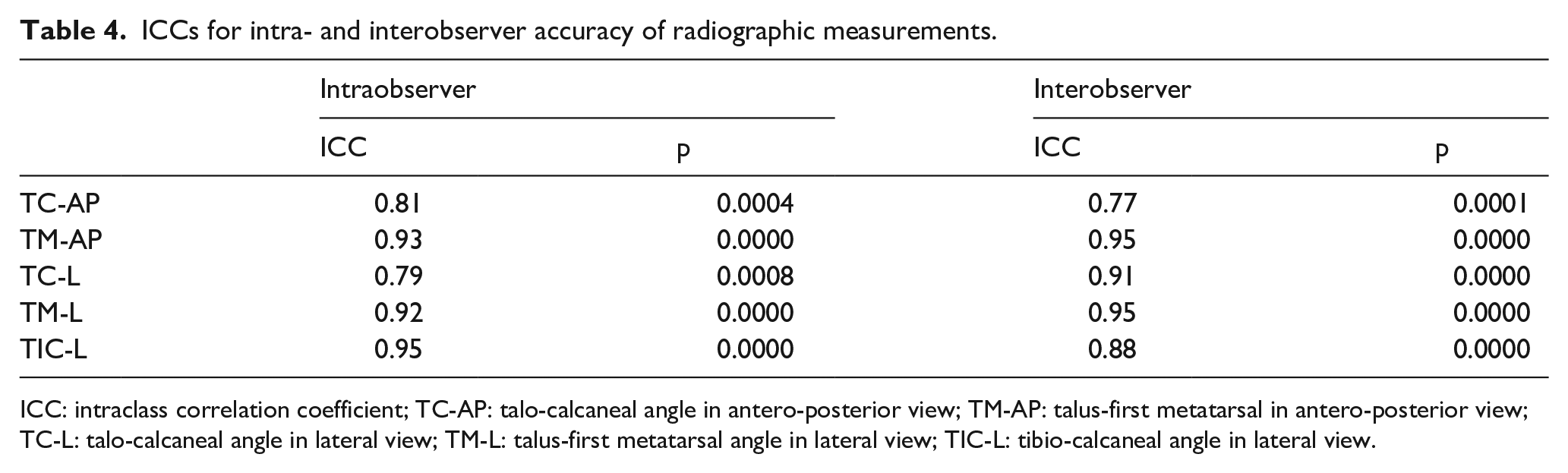
ICC: intraclass correlation coefficient; TC-AP: talo-calcaneal angle in antero-posterior view; TM-AP: talus-first metatarsal in antero-posterior view; TC-L: talo-calcaneal angle in lateral view; TM-L: talus-first metatarsal angle in lateral view; TIC-L: tibio-calcaneal angle in lateral view.
The t-test results showed that TC-AP, TM-AP, TC-L, and TIC-L in the non-relapsed group were significantly different from those in the relapsed group. However, TM-L of the non-relapsed group was similar to that of the relapsed group (p = 0.42) (Table 5). Receiver operating characteristic (ROC) analysis showed that all angles except TM-L (p = 0.32) were predictive of relapse (Table 6).
Comparison of angles between the relapsed group and non-relapsed group.
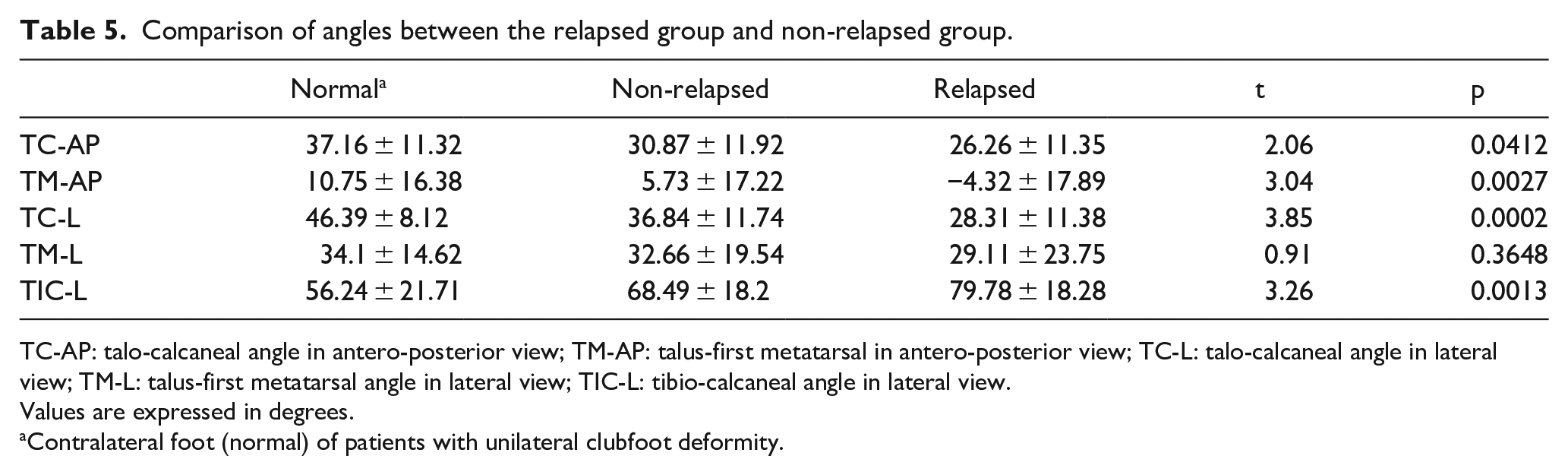
TC-AP: talo-calcaneal angle in antero-posterior view; TM-AP: talus-first metatarsal in antero-posterior view; TC-L: talo-calcaneal angle in lateral view; TM-L: talus-first metatarsal angle in lateral view; TIC-L: tibio-calcaneal angle in lateral view.
Values are expressed in degrees.
Contralateral foot (normal) of patients with unilateral clubfoot deformity.
Results of receiver operating characteristic analysis.
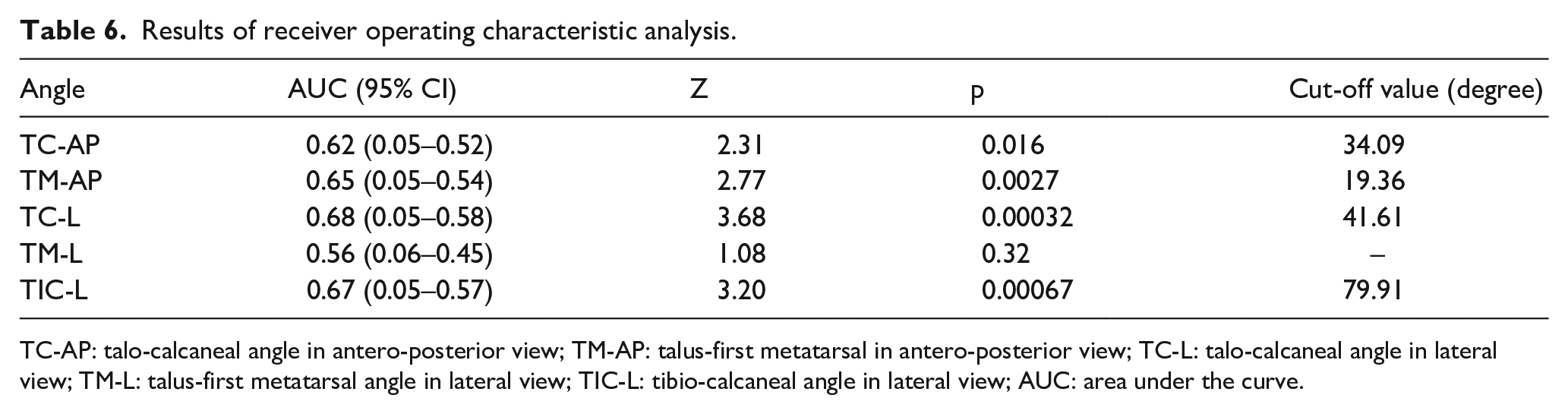
TC-AP: talo-calcaneal angle in antero-posterior view; TM-AP: talus-first metatarsal in antero-posterior view; TC-L: talo-calcaneal angle in lateral view; TM-L: talus-first metatarsal angle in lateral view; TIC-L: tibio-calcaneal angle in lateral view; AUC: area under the curve.
The multi-factor logistic regression model of the stepwise selection method was used to predict the relapse of clubfoot deformity from the four potential predictive values21,22 (Figure 3), as TM-L angle (p = 0.32) was not predictive (Table 6). Among the four remaining parameters, only TM-AP (p = 0.033) and TIC-L (p = 0.015) were found to be predictive of relapse and could be included in the “risk of relapse” formula

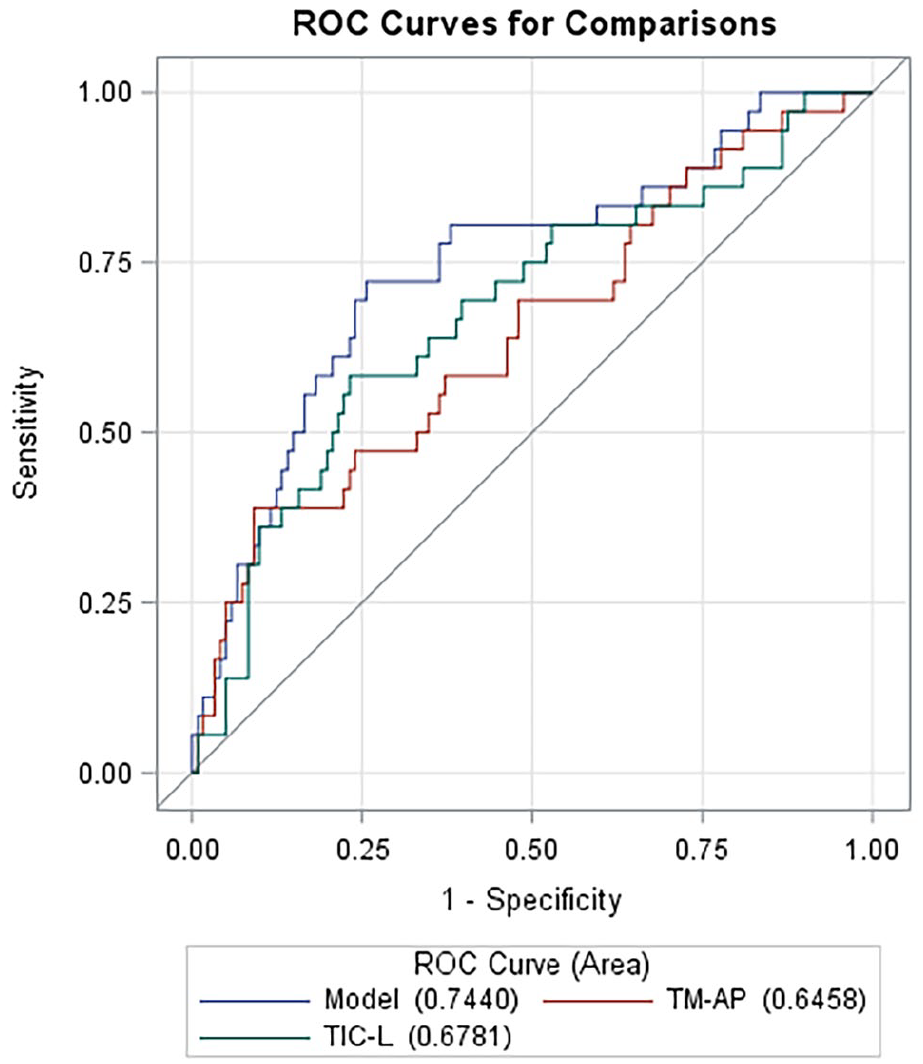
The receiver operating characteristic (ROC) curve after logistic regression model of stepwise selection.
Discussion
Clubfoot relapse after Ponseti treatment is not negligible. In our study, the overall rate of relapse was 24% with a male:female ratio of 1.89:1, which is similar to previously published reports.23,24
In previous reports, noncompliance to FAO treatment and high initial severity scores were predictive indicators of relapse.25,26 However, assessing FAO compliance and initial severity scores is subjective. 8 Radiographs can be routinely used in clinical practice and represent an objective evaluation method.
In our study, we found that early foot radiographs in children with IC treated using the Ponseti technique are predictive of relapse. The predictive value of early radiographs had also been investigated by Mishima et al., 27 although in their study they performed radiographs before Achilles tenotomy. In our study, we investigated the predictive value of five angles: TC-AP, TM-AP, TC-L, TIC-L, and TM-L.13,28 In particular, as shown by previous studies, the TM-AP angle can assess the severity of forefoot adduction; the TC-AP and TC-L angles can evaluate the position of the subtalar joint; the TM-L angle can estimate the severity of the midfoot cavus; and the TIC-L angle can evaluate ankle dorsiflexion.13,28,29 As a result, these five angular measurements summarize all the IC deformity components.3,7 According to our data, although TC-AP, TM-AP, TC-L, and TIC-L were significantly different between the non-relapsed and relapsed groups, TC-AP (p = 0.57) and TC-L (p = 0.19) had to be excluded because their p-value was >0.05, while only TM-AP (p = 0.033) and TIC-L (p = 0.015) could be included in the predictive formula using the stepwise selection method.21,22 Our analysis indicates that the TM-AP and TIC-L angles had positive predictive values for relapse (Figures 4 and 5). Although radiographs in 3-month-old patients may be objective but not always reproducible, our data showed similar inter- and intraclass reliability compared to previous reports (Table 7).30,31
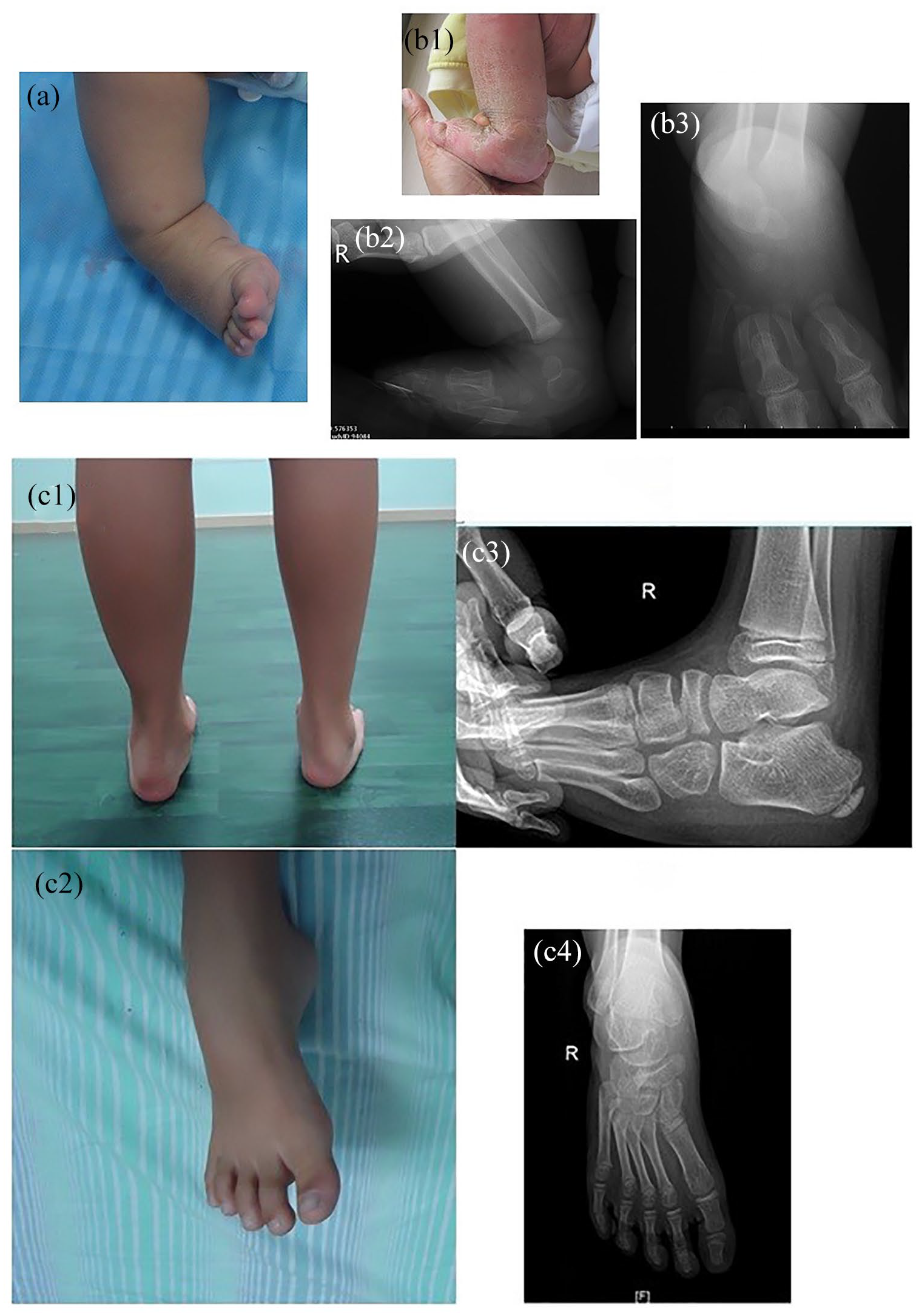
Patients with relapse: (a) right clubfoot, age 17 days, before treatment; (b) 3.4 months of age; (c) age 7 years.
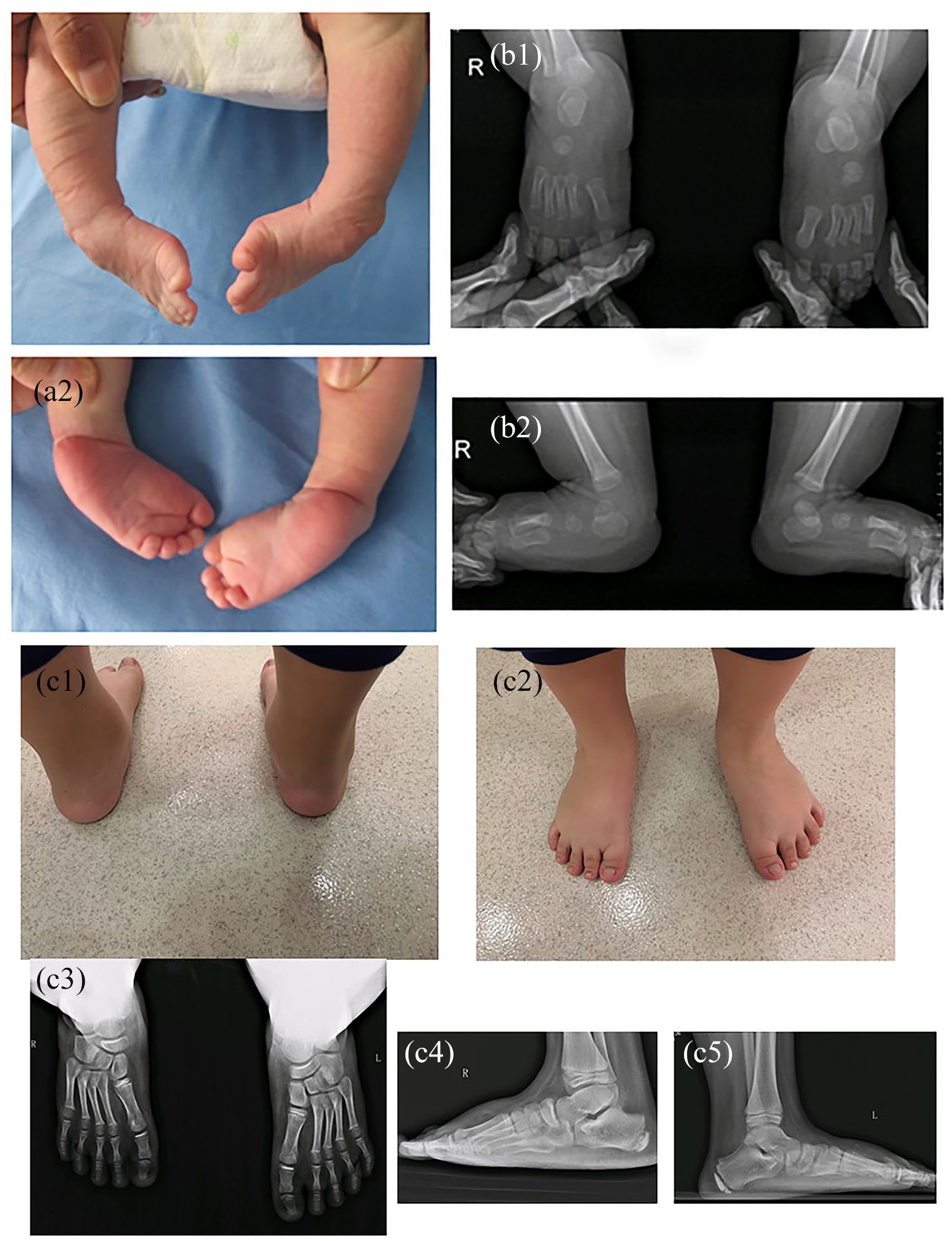
Patient without relapse: (a) bilateral clubfoot, age 3 days, before treatment; (b) 2.4 months of age; (c) age 8 years.
Intra- and interobserver reliability: comparison with previous reports.
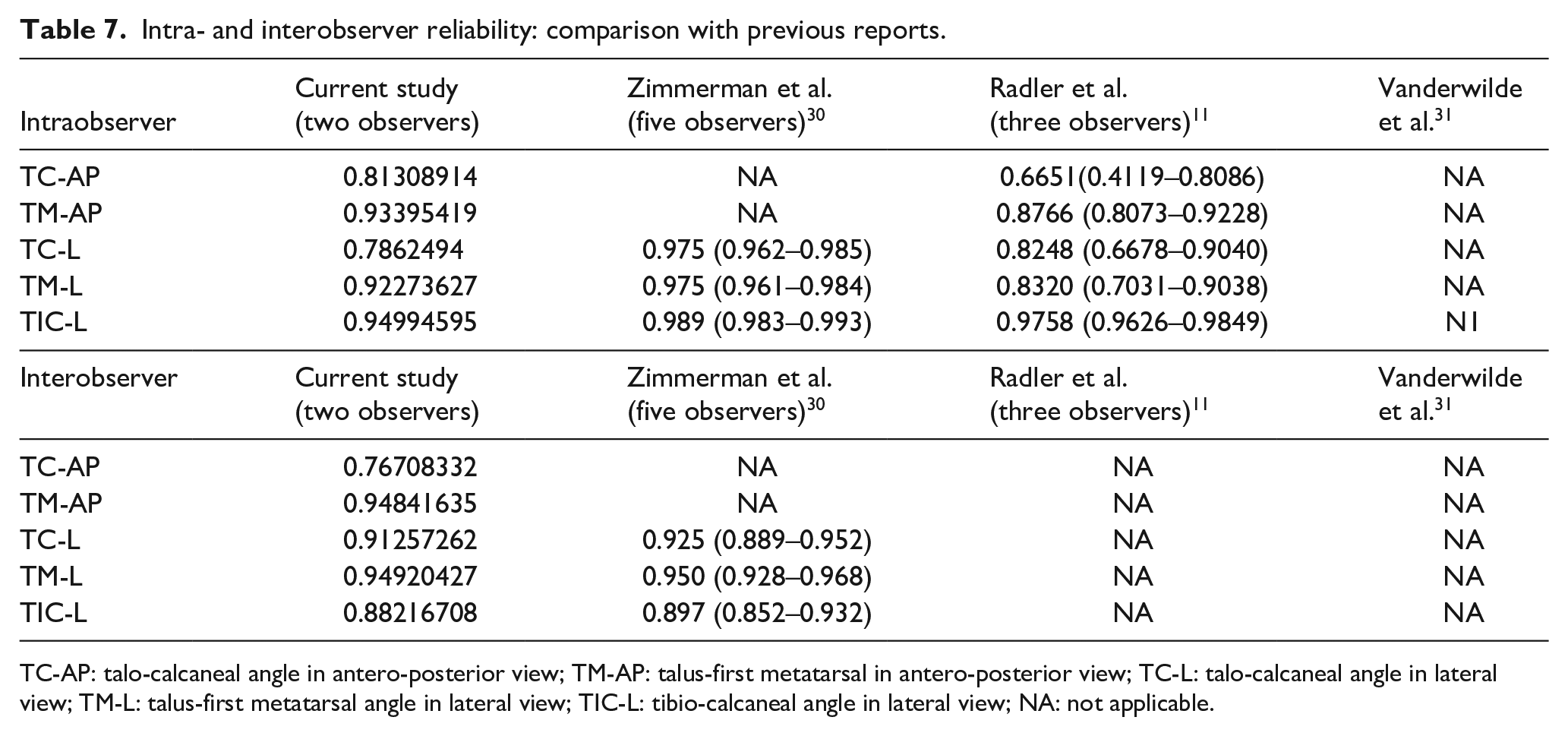
TC-AP: talo-calcaneal angle in antero-posterior view; TM-AP: talus-first metatarsal in antero-posterior view; TC-L: talo-calcaneal angle in lateral view; TM-L: talus-first metatarsal angle in lateral view; TIC-L: tibio-calcaneal angle in lateral view; NA: not applicable.
The TM-AP angle in the relapsed group (−4.25° ± 4.25°) was smaller than that in the non-relapsed group (5.79° ± 0.79°), and it was even smaller than that in normal feet (10.75° ± 0.75°). We found that the risk of relapse increased with a reduction in the TM-AP angle. It is possible that soft tissues are stiffer in the relapsed group than in the non-relapsed group, although all patients were placed at 60° or more of abduction during cast and FAO treatment. We also found that TIC-L is more objective than ankle dorsiflexion angle in assessing the severity of equinus, as shown by Kang and Park. 10 According to our results, the risk of relapse was proportional to TIC-L values. Based on the representation of the angle, we can infer that the hindfoot varus, forefoot adduction, and ankle dorsiflexion are important parameters to assess during follow-up of patients treated by the Ponseti method.
According to the previous study, the degree of plantar deviation of the talar head and neck had no significant difference between normal foot (−14.7° ± 9.1°) and clubfoot (−15.6° ± 13.3°) being accessed by three-dimensional magnetic resonance imaging (MRI). 32 Howard and Benson 33 found that AP projections of the nucleus of the talus show deformity of that bone as well as subtalar malalignment. The TC-AP and TC-L angles somehow represent the relationship between the talus and the calcaneus. We found both angles were reduced in IC compared to normal feet; moreover, both angles were smaller in the relapsed group than in the non-relapsed group. However, in the process of logistic regression analysis, neither of them was included in the predictive formula, indicating that both TC-AP and TC-L had little value in predicting the relapse of the deformity. In a previous study, Li et al. 13 also found that TC-L did not significantly change after Achilles tenotomy. Therefore, it is possible that once good initial correction is achieved, assessing hindfoot deformity may not be the most important parameter to assess in order to predict a possible relapse. However, this conclusion needs to be supported by stronger data. Particularly, we found TC-AP and TC-L were significantly different between the relapsed and non-relapsed groups, although they could not be included in the “risk of relapse” formula. Therefore, studies with a higher number of patients exploring the value of TC-AP and TC-L in predicting clubfoot relapse are needed.
The TM-L angle represents the midfoot cavus; in our study, we could not identify any significant TM-L angle difference between the non-relapsed and relapsed groups. Early assessment of the TM-L angle may have limited value in predicting the risk of relapse; this is probably related to the fact that the foot arch has not completed its development at an early age.34,35
Although this study evaluated the risk of relapse using AP and lateral foot radiographs, it was noticed that the risk of relapse was higher in patients with poor brace compliance. Obtaining foot radiographs 3 months after Achilles tenotomy may aid in emphasizing the importance of FAO for a patient at risk of relapse, as well as the need of regular follow-up visits, especially during brace treatment.
We encountered some limitations in the analysis of our results, including its retrospective design and the exclusion of several cases due to the lack of initial radiographs and/or loss to follow-up. Moreover, the sensitivity and specificity of the predictive formula (area under the curve (AUC) = 0.7383) (Figure 3) were not excellent, so the value of the predictive formula may be relative. However, this is the first study to assess the predictive value of AP and lateral radiographs of a large cohort of patients with IC, treated by the Ponseti method by the same surgical team, with a mean follow-up of 7 years. These results should be considered preliminary, and a prospective study is needed to confirm the predictive value of the initial AP and lateral radiographs in patients with IC.
Conclusion
Initial AP and lateral radiographs have satisfactory predictive value for assessing the risk of relapse in children with IC treated using the Ponseti method. The measurement of the angles reflects the severity of the deformity, while the TM-AP and TIC-L angles are the key indicators for estimating the risk of relapse and the need for additional surgery. It appears that a reduction in the TM-AP angle and an increase in the TIC-L angle are associated with an increased risk of relapse.
Footnotes
Author contributions
JCL: Manuscript preparation, Study design, Performed measurements, Patient follow-up, Statistical analysis. CCX: Patient follow-up, Performed measurements. YQL: Patient follow-up, Statistical analysis. YZL: Patient follow-up. HWX: Study design, Reviewed the final manuscript, Approved the final version. FC: Study design, Reviewed the final manuscript critically for important intellectual content, Approved the final version.
Compliance with ethical standards funding statement
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. The study was approved by our institution’s Ethical Committee of Scientific Research.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by funds from Guangzhou Institute of Paediatrics/Guangzhou Women and Children’s Medical Centre (NO: Pre-NSFC-2018-010).
Informed consent
Informed consent was obtained from all individual participants included in the study. All parents consented to and were informed that data concerning this study would be submitted for publication.