
Abstract
Purpose:
This study aimed to investigate foot kinematics during gait in individuals with idiopathic clubfoot initially treated with the Ponseti method, focusing on clubfoot-specific deformities, to improve the understanding of posttreatment functional impairments.
Methods:
In this prospective cohort study, 23 patients with treated idiopathic clubfoot (34 feet) were compared with 15 age-matched healthy controls (30 feet). Gait analysis was performed using the Heidelberg Foot Model. To characterize residual clubfoot deformities, selected kinematic parameters included medial arch and subtalar angles, as well as intersegmental angles between hindfoot-shank and forefoot-hindfoot, based on more functional joint centers. Within the patient group, potential influence of additional surgical interventions was explored.
Results:
Compared with controls, treated idiopathic clubfoot exhibited significant reductions in hindfoot sagittal and transverse range of motion, forefoot sagittal range of motion, and medial arch mobility. Equinus deformity was not present posttreatment, as dorsiflexion metrics during stance did not differ significantly. However, plantarflexion range of motion during the transition to swing was reduced. In addition, treated idiopathic clubfoot showed persistent subtalar inversion and hindfoot varus, increased mid-stance adductus in both hindfoot and forefoot, and pronounced arch stiffness during transition to swing. Within the patient group, ankle and subtalar capsulotomy was associated with increased medial arch cavus.
Conclusion:
Patients with treated idiopathic clubfoot exhibit a functionally stiffer foot with altered alignment during gait, contributing to impaired limb advancement. The results expand the understanding of residual clubfoot deformities and highlight the importance of detailed functional assessment posttreatment, providing a foundation for future research.
Level of evidence:
Level II, prognostic study.
Introduction
Idiopathic congenital talipes equinovarus (ICTEV), commonly known as idiopathic clubfoot, typically presents with a combination of equinus, varus, supinatus, adductus, and cavus deformities. Recent perspectives on pathomechanics suggest that inversion would more accurately describe the deformity of the calcaneopedal unit, which results in varus, while cavus is often associated with forefoot pronation.1–4
Despite extensive research, the etiology and pathogenesis of ICTEV remain unclear, 5 making it impossible to base treatment directly on these factors. Consequently, established treatment methods focus on correcting functional deviations from the healthy foot. The gold standard for ICTEV management is the Ponseti method, 6 which involves serial manipulation and casting to gradually correct the deformities, followed by a Achilles tendon tenotomy and subsequent bracing to prevent recurrence.
There is currently no standardized definition of relapse, nor are there universally established guidelines for its management. In general, a repeated conservative approach following the principles of initial treatment is recommended, while surgical measures are adapted on an individual basis. 7
Since ICTEV treatment typically begins in infancy, untreated cases are becoming increasingly rare. This shift underscores the clinical importance of precisely analyzing the functional outcomes of treated ICTEV, which remain insufficiently understood and continue to pose challenges for further therapeutic decision-making. Gait analysis using multi-segmental foot models offers a valuable approach that contributes to a better understanding of functional deficits in treated ICTEV.8–13
The Heidelberg Foot Model, first introduced in 2006 14 and refined through the integration of more functionally relevant joint parameters,15,16 enables a detailed analysis of foot function. Accordingly, this study aimed to characterize residual deformities in idiopathic clubfoot initially treated using the Ponseti method, by analyzing gait kinematics with the Heidelberg Foot Model in comparison with controls, thereby contributing to a more comprehensive understanding of functional limitations following treatment. Furthermore, the study examines the potential impact of additional surgical interventions on foot kinematics within the ICTEV group.
Methods
This prospective cohort study was conducted with the approval of Ethics Committee of the Medical Faculty of the local university (reference number: S-636/2024).
In 2024, patients aged between 5 and 17 years with diagnosed ICTEV who met the inclusion criteria were identified during visits to the pediatric orthopedic outpatient clinic of the local university hospital (January–September 2024) and invited to participate in the study. Inclusion criteria were initial treatment during infancy, with or without subsequent surgical or conservative interventions, and no surgical procedures within the past 2 years. All eligible patients within the defined timeframe were contacted. Age-matched typically developing (TD) control participants were recruited from acquaintances.
Of the 71 contacted patients, 25 patients and their guardians provided written informed consent to participate. The remaining individuals declined or were unable to participate, mainly due to logistical and organizational constraints during the study period, including long travel distances, limited parking availability caused by renovation work at our institute, and restricted appointment times. To ensure homogeneity in initial treatment, two participants were retrospectively excluded due to non-Ponseti-based initial therapy. The final patient group consisted of 23 individuals (6 female, 17 male; 34 feet) with an average age of 8.4 ± 2.9 years (range: 5–15 years), a height of 135 ± 19 cm, and a weight of 33.2 ± 17.3 kg. Among them, 11 had bilateral involvement, and 12 (18 feet) had undergone additional soft tissue and/or joint-invasive surgical interventions following initial Ponseti treatment (for details, see Table 1). The control group comprised 15 individuals (5 female, 10 male; 30 feet) with an average age of 9.4 ± 3.5 years (range: 5–16 years), a height of 142 ± 21.5 cm, and a weight of 36.6 ± 17.7 kg.
Treatments received by the ICTEV patient group.
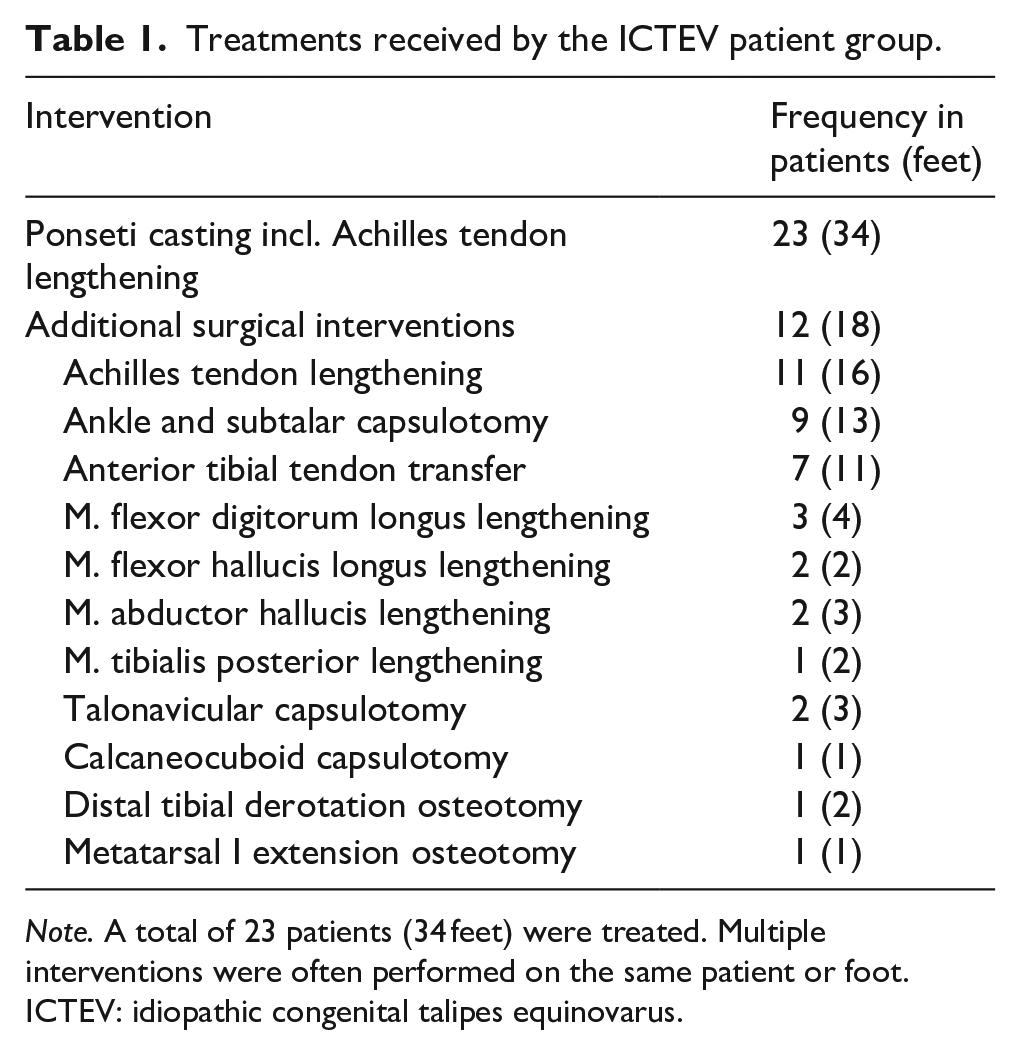
Note. A total of 23 patients (34 feet) were treated. Multiple interventions were often performed on the same patient or foot.
ICTEV: idiopathic congenital talipes equinovarus.
Study participants underwent gait analysis using the Heidelberg Foot Model, with motion captured using a 12-camera Vicon Nexus Motion System (Vicon; Oxford Metrics, Yarnton, England). Marker placement followed the previously established protocol, 14 with modifications introduced through the use of a new hindfoot alignment device. 17 Kinematic data were determined and visualized using Matlab (© 1994–2025; The MathWorks, Inc, Natick, MA, USA). ChatGPT (© 2018–2025; OpenAI, LLC, San Francisco, CA, USA) was used to assist with Matlab figure formatting.
To describe ICTEV-specific deformities, selected foot kinematic parameters included the medial arch (MA) and subtalar (ST) angles, 14 as well as intersegmental angles between the hindfoot and shank (Hf/Sh)—specifically flexion (Hf/Sh Flex), valgus–varus, and rotation—and between the forefoot and hindfoot (Ff/Hf), including flexion (Ff/Hf Flex), pronation–supination, and abduction–adduction. The intersegmental angles were defined based on functional joints: the Heel Rotation Center 16 and the Midfoot Joint Center. 15 Figure 1 schematically illustrates the application of these parameters in the context of clubfoot deformities. Further methodological details on the kinematic parameters are provided in the Supplementary Material.
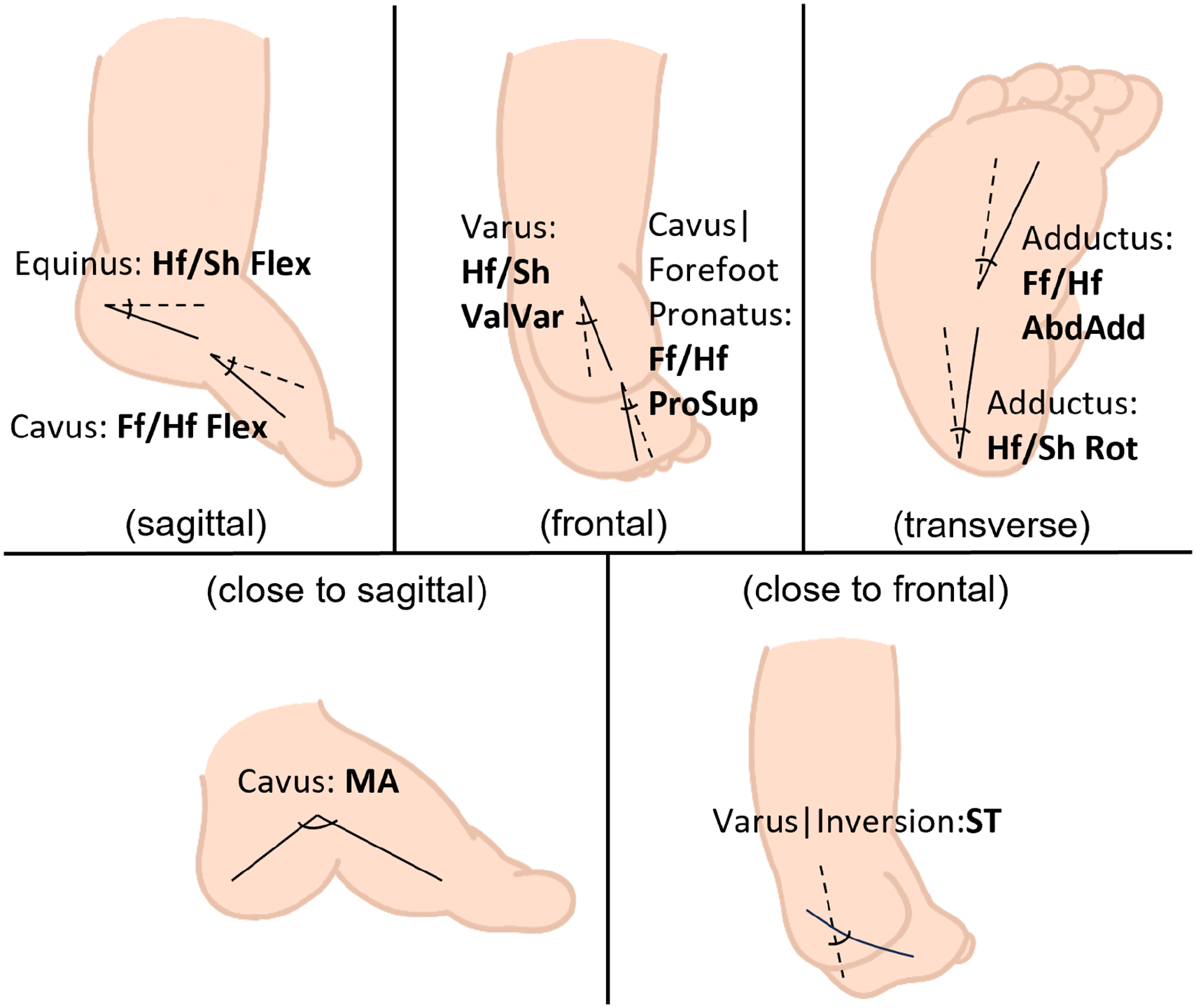
Kinematic parameters of the Heidelberg Foot Model selected to describe clubfoot deformities.Intersegmental angles between hindfoot and shank (Hf/Sh): Flexion (Hf/Sh Flex), Valgus-Varus (Hf/Sh ValVar), and Rotation (Hf/Sh Rot); Intersegmental angles between forefoot and hindfoot (Ff/Hf): Flexion. (Ff/Hf Flex), Pronation-Supination (Ff/Hf ProSup), and Abduction-Adduction (Ff/Hf AbdAdd); Medial Arch Angle (MA); Subtalar Angle (ST).
The gait cycle (GC) was normalized to subphases: loading response (LR, from foot strike to opposite foot off), mid-stance (MSt, first half between opposite foot off and opposite foot strike), terminal stance (TSt, second half between opposite foot off and opposite foot strike), pre-swing (from the opposite foot strike to foot off), initial swing (ISw, first third of the swing phase), mid-swing (MSw, second third of the swing phase), and terminal swing (final third of the swing phase).
To characterize foot motion in detail while ensuring robustness, all individual kinematic curves were visually inspected and compared. Depending on the curve profile and variability across subjects, representative features were extracted at distinct gait phases, including minimum, maximum, and mean values, where functionally meaningful motion and reliable curve morphology were present. Range of motion (ROM) was calculated either over the full GC or between specific local extrema, following the same criteria. Feature selection prioritized parameters with low pattern morphology variability and clear biomechanical relevance, covering sagittal, frontal, and transverse intersegmental angles, as well as MA and ST angles.
For group comparisons between individuals with ICTEV and TD controls, a Linear Mixed Model was applied using SPSS Inc., IBM, Armonk, NY, USA to account for the inclusion of both feet in healthy controls and bilaterally affected patients. In addition to the main analysis, the influence of frequently performed surgical interventions (Achilles tendon lengthening, ankle and ST capsulotomy, and anterior tibial tendon transfer) was also examined within the ICTEV group. To validate the model, residual distributions were assessed using the Shapiro–Wilk test and Q–Q-plots. Statistical significance was defined as p < 0.05. No adjustment for multiple comparisons was applied, as all kinematic parameters were predefined based on clinical and biomechanical relevance and were analyzed individually within a hypothesis-driven framework.
Results
Figure 2 illustrates the mean kinematic curves for all investigated parameters across the GC, with additional indicators showing statistically analyzed minimum, maximum, and mean values during specific gait phases. Figure 3 displays the ROM for selected gait parameters. The corresponding numerical results are summarized in Table 2.
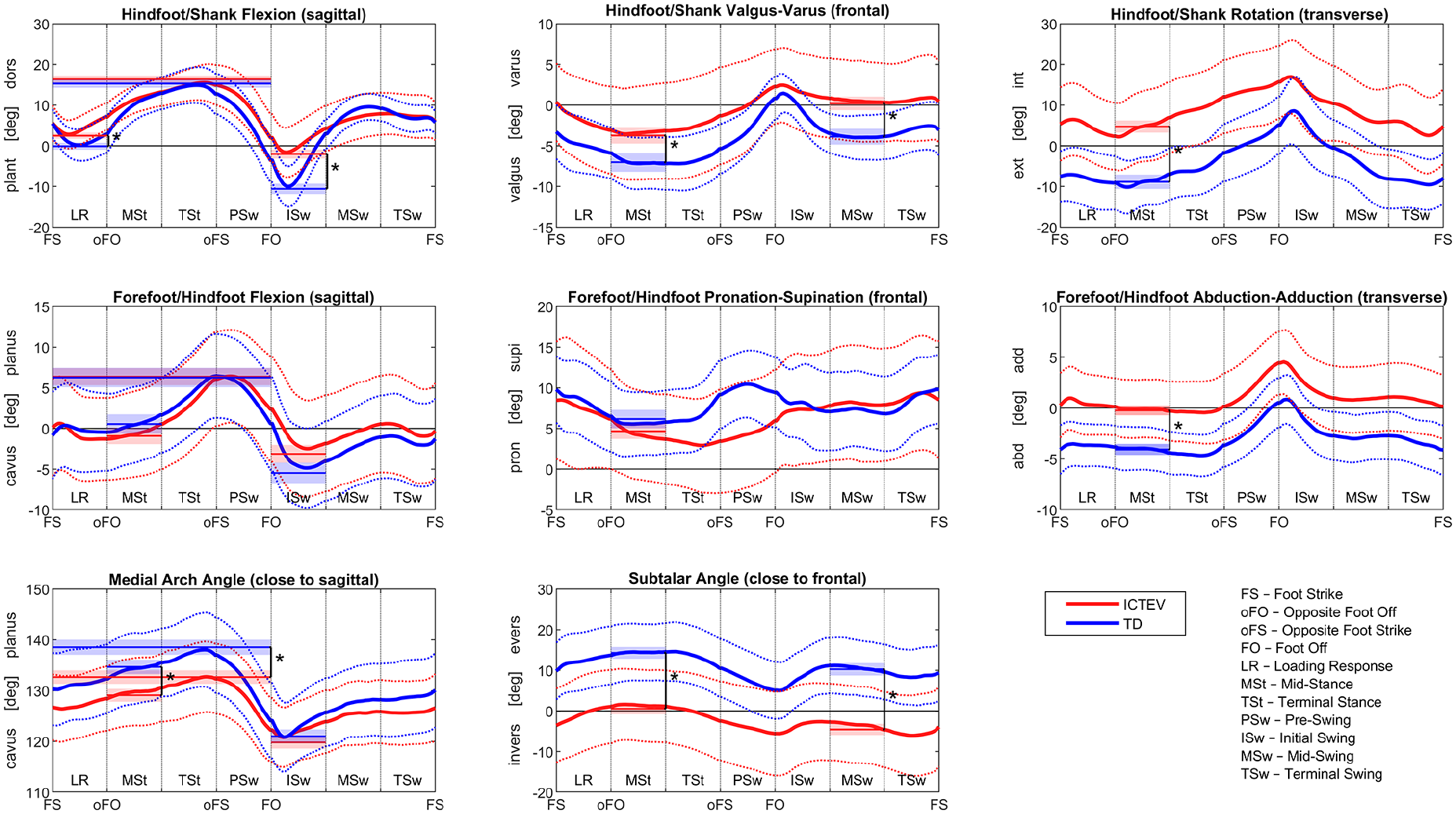
Kinematic patterns showing observed group means (solid lines) and standard deviations (dotted lines) for the ICTEV and TD groups. Thinner lines with shaded areas at the minimum, maximum, or mean values of specific gait phases represent estimated marginal means with standard errors from the statistical analysis. Asterisk (*) indicates statistical significance.
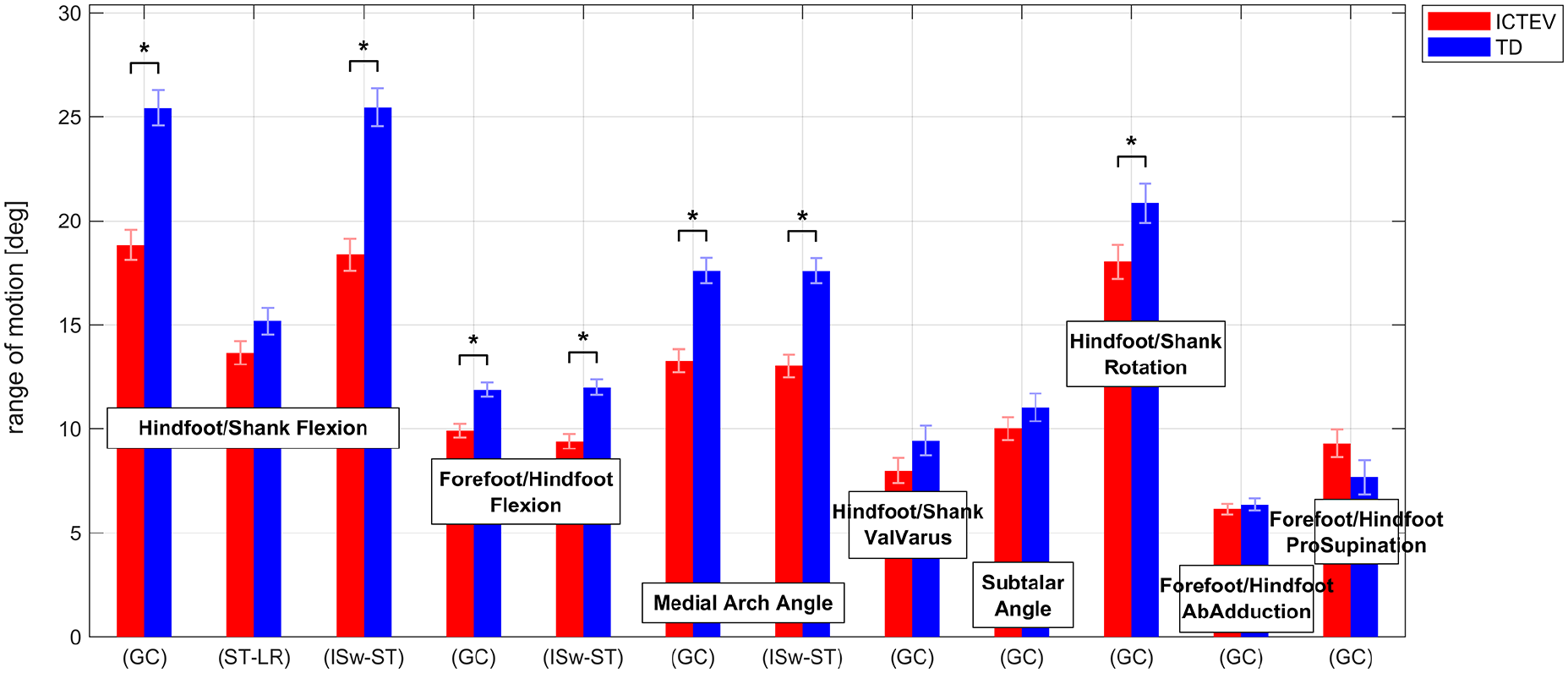
Range of motion during selected gait phases for kinematic parameters in the ICTEV and TD groups. Bars represent estimated marginal means with standard errors from the statistical analysis. Statistically significant differences are marked with an asterisk (*). Range of motion is calculated either over the full GC or within specific gait phases: from the minimum in LR to the maximum in ST and from the maximum in ST to the minimum in ISw.
Group comparisons between ICTEV and TD groups using a Linear Mixed Model.
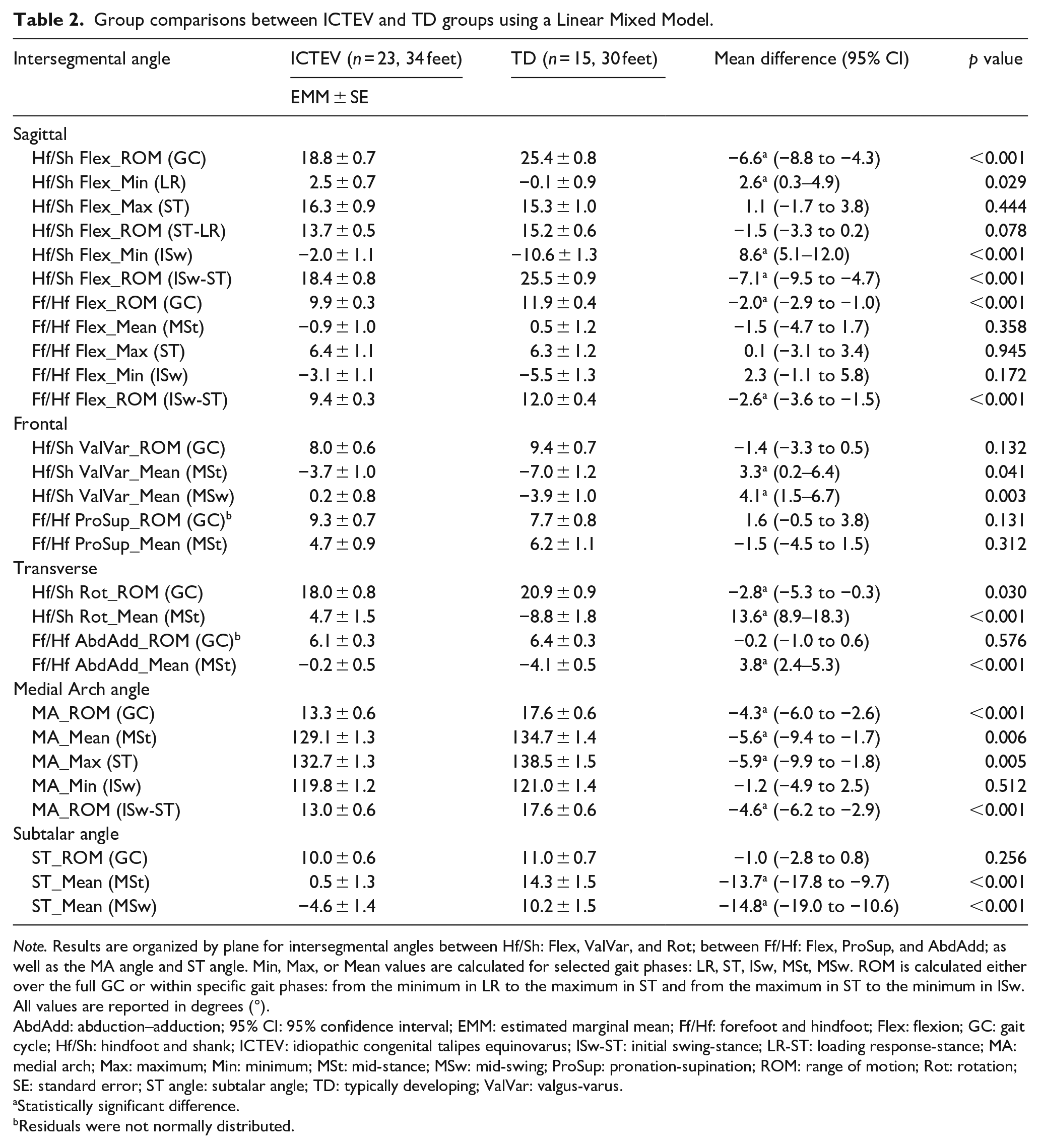
Note. Results are organized by plane for intersegmental angles between Hf/Sh: Flex, ValVar, and Rot; between Ff/Hf: Flex, ProSup, and AbdAdd; as well as the MA angle and ST angle. Min, Max, or Mean values are calculated for selected gait phases: LR, ST, ISw, MSt, MSw. ROM is calculated either over the full GC or within specific gait phases: from the minimum in LR to the maximum in ST and from the maximum in ST to the minimum in ISw. All values are reported in degrees (°).
AbdAdd: abduction–adduction; 95% CI: 95% confidence interval; EMM: estimated marginal mean; Ff/Hf: forefoot and hindfoot; Flex: flexion; GC: gait cycle; Hf/Sh: hindfoot and shank; ICTEV: idiopathic congenital talipes equinovarus; ISw-ST: initial swing-stance; LR-ST: loading response-stance; MA: medial arch; Max: maximum; Min: minimum; MSt: mid-stance; MSw: mid-swing; ProSup: pronation-supination; ROM: range of motion; Rot: rotation; SE: standard error; ST angle: subtalar angle; TD: typically developing; ValVar: valgus-varus.
Statistically significant difference.
Residuals were not normally distributed.
Equinus post-treatment
The ICTEV group demonstrated a significantly reduced ROM of the hindfoot in the sagittal plane throughout the GC compared with the TD group (p < 0.001).
During stance, the minimum Hf/Sh sagittal angle during LR was significantly higher in the ICTEV group (p = 0.029), indicating a more dorsiflexed hindfoot position. However, the maximum dorsiflexion achieved later in stance (Hf/Sh Flex_Max (ST)) did not differ significantly from the TD group (p = 0.444). The dorsiflexion ROM during stance (Hf/Sh Flex_ROM (ST-LR)) was also not significantly different (p = 0.078).
At the transition to the swing phase, the minimum Hf/Sh sagittal angle during ISw was significantly higher, indicating a less plantarflexed hindfoot position (p < 0.001). Similarly, the plantarflexion ROM during the transition to ISw (Hf/Sh Flex_ROM (ISw-ST)) was significantly reduced (p < 0.001).
Varus and Subtalar inversion post-treatment
The ROM of the hindfoot in the frontal plane throughout the GC and the ST ROM of motion did not differ significantly between the two groups (p = 0.132 and p = 0.256, respectively).
During MSt, the average Hf/Sh frontal angle in the ICTEV group was significantly higher than in the TD group (p = 0.041) and the average ST angle was significantly lower (p < 0.001), indicating a more varus and inverted position.
During MSw, the average Hf/Sh frontal angle was also significantly higher in the ICTEV group (p = 0.003), and the average ST angle was significantly lower (p < 0.001), indicating a more varus and inverted position.
Adductus posttreatment
The ICTEV group showed a significantly reduced hindfoot ROM in the transverse plane throughout the GC compared with the TD group (p = 0.030). The average Hf/Sh transverse angle during MSt was significantly higher (p < 0.001), indicating a more internal rotated or adducted hindfoot position.
The forefoot ROM in the transverse plane throughout the GC did not differ significantly between the groups (p = 0.576). However, the average Ff/Hf transverse angle during MSt was significantly higher in the ICTEV group (<0.001), indicating a more adducted forefoot position.
Cavus and forefoot pronatus post-treatment
Throughout the GC, the forefoot sagittal ROM and the MA ROM were both significantly reduced in the ICTEV group compared with those in the TD group (p < 0.001 and p < 0.001, respectively). The forefoot frontal ROM did not show significant difference (p = 0.131).
During stance, the average MA angle during MSt was significantly lower in the ICTEV group (p = 0.006), indicating a more cavus position regarding the MA, whereas the average Ff/Hf sagittal and frontal angles did not differ significantly between the groups (p = 0.358 and p = 0.312, respectively). The maximum MA angle achieved later in the stance phase (MA_Max (ST)) was significantly lower in the ICTEV group (p = 0.005), indicating a more cavus position regarding the MA, while the maximum Ff/Hf sagittal angle (Ff/Hf Flex_Max (ST)) did not show a significant difference (p = 0.945).
At the transition to the swing phase, the ROM from stance to ISw was significantly lower in the ICTEV group for both the forefoot sagittal plane (Ff/Hf Flex_ROM (ISw-ST), p < 0.001) and the MA (MA_ROM (ISw-ST), p < 0.001). However, the minimum Ff/Hf sagittal angle and the minimum MA angle during ISw were not significantly different between groups (p = 0.172 and p = 0.512, respectively).
Effect of frequent interventions
As shown in Table 3, only a limited number of kinematic angles were significantly affected by frequent surgical interventions within the ICTEV group. Individuals who had undergone ankle and ST capsulotomy demonstrated a significantly lower average MA angle during MSt (p = 0.013), a lower maximum MA angle during TSt (p = 0.007), and a lower minimum MA angle during ISw (p = 0.008), indicating a more cavus position of the MA. In addition, the average ST angle during MSt was significantly higher in this group (p = 0.033), suggesting a less inverted position.
Effect of frequent interventions on kinematic angles using Linear Mixed Model.
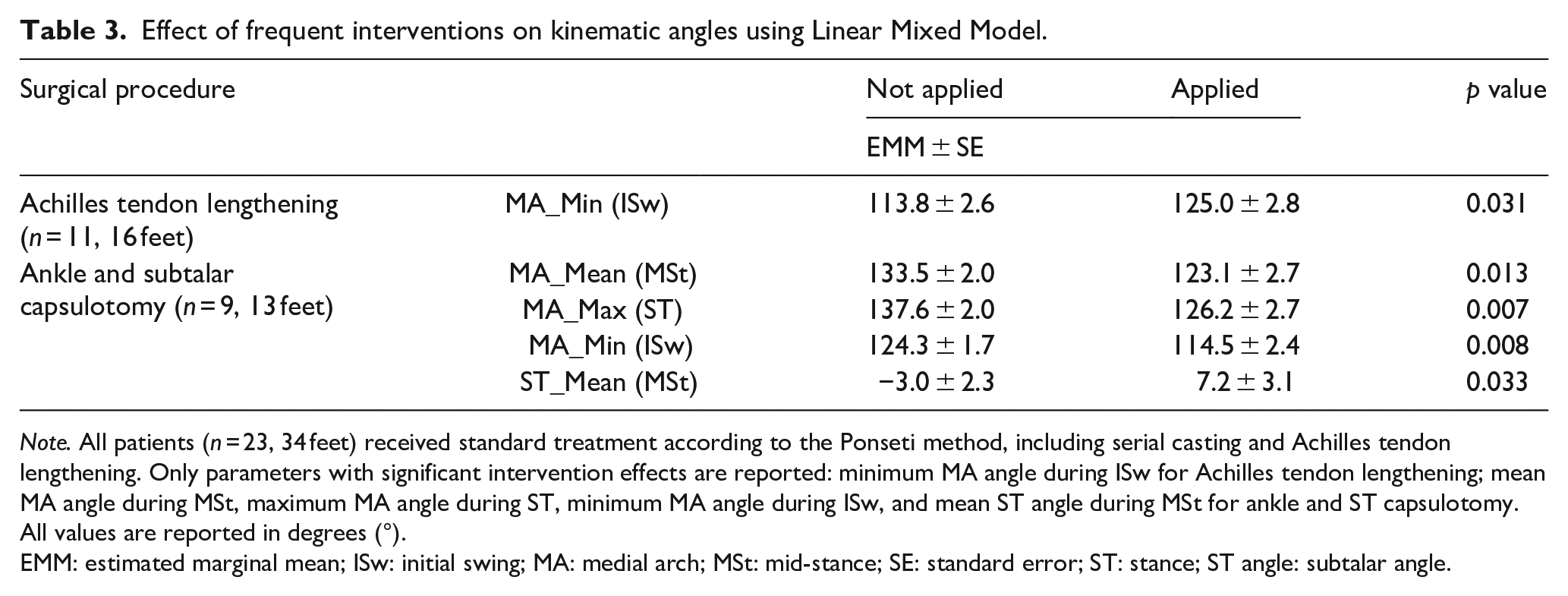
Note. All patients (n = 23, 34 feet) received standard treatment according to the Ponseti method, including serial casting and Achilles tendon lengthening. Only parameters with significant intervention effects are reported: minimum MA angle during ISw for Achilles tendon lengthening; mean MA angle during MSt, maximum MA angle during ST, minimum MA angle during ISw, and mean ST angle during MSt for ankle and ST capsulotomy. All values are reported in degrees (°).
EMM: estimated marginal mean; ISw: initial swing; MA: medial arch; MSt: mid-stance; SE: standard error; ST: stance; ST angle: subtalar angle.
Individuals who received Achilles tendon lengthening exhibited a less cavus position of the MA during ISw, as indicated by a significantly higher minimum MA angle (p = 0.031).
Discussion
ROM throughout the GC
Our study revealed significant gait deviations in individuals with treated idiopathic clubfoot across multiple aspects. Overall, treated ICTEV exhibited reduced ROM throughout the GC. Specifically, the ROM of the hindfoot in both the sagittal and transverse planes was reduced, while the hindfoot frontal ROM and ST ROM did not differ significantly from the controls. The forefoot sagittal ROM and MA ROM were both diminished. However, the forefoot frontal and transverse ROM did not show significant differences. As the residuals for these two parameters were not normally distributed, these nonsignificant results may be unreliable.
These findings expand upon previous studies that have investigated overall ROM deviations in treated ICTEV using the Oxford Foot Model. McCahill et al. 11 examined symptomatic ICTEV patients and found that those treated with surgical release (subsequent surgery included) exhibited reduced hindfoot ROM in the sagittal and frontal planes and increased hindfoot transverse ROM compared with controls. In comparison, ICTEV patients treated with the Ponseti method, including those who underwent additional soft tissue surgery, also showed an increase in hindfoot ROM in the transverse plane, but ROM in other planes did not differ significantly. Notably, forefoot ROM in their study did not show any significant differences in any plane for either ICTEV group. Focusing specifically on ICTEV patients treated with the Ponseti method, Grin et al. 9 found that those requiring additional treatments exhibited reduced hindfoot ROM only in the sagittal plane, while ROM in the other planes remained comparable to controls. Their study also reported no significant differences in forefoot ROM across any plane. Lööf et al. 10 similarly observed reduced hindfoot sagittal ROM in ICTEV patients treated with the Ponseti method, including cases with additional soft tissue surgery. In contrast, Mindler et al. 12 examined ICTEV patients treated with the Ponseti method, including those who underwent additional soft tissue surgery, and found a reduction in forefoot ROM only in the sagittal plane. Forefoot ROM in other planes and hindfoot ROM in all three planes, however, did not differ significantly from the control group.
In addition to differences in patient cohort characteristics, the variability in results between our study and previous research may stem from different segment and joint definitions in the models applied. The key difference is that the Oxford Foot Model 18 excludes the midfoot or tarsal bones, defining the rearfoot by the calcaneus and the forefoot by the metatarsals, whereas the Midfoot Joint Center 15 is implemented in the Heidelberg Foot Model (details see Supplementary Material). Therefore, caution is warranted when comparing the results, which underscores the need for a more detailed analysis of specific deformities.
Plantarflexion deficit and heel rocker dysfunction
Building on the findings of overall ROM restrictions, a closer examination of deformities in treated ICTEV reveals persistent ST inversion along with varus, adductus, and cavus deformities. In contrast, equinus does not appear to be present, as maximum dorsiflexion and dorsiflexion ROM during stance do not differ significantly from controls. Instead, a notable finding is the reduced maximal plantarflexion and plantarflexion ROM during the transition from stance to swing. These findings are consistent with Lööf et al. 10 who reported no significant differences in maximal dorsiflexion but noted reduced maximal plantarflexion in ICTEV patients. In comparison, Grin et al. 9 observed no significant differences in both maximal dorsiflexion during stance and maximal plantarflexion. Similarly, Theologis et al., 13 using the Oxford Foot Model, found no significant differences in hindfoot dorsiflexion ROM in ICTEV patients treated with surgical release.
Since Achilles tendon lengthening is a well-established component of current ICTEV management, and residual equinus can be easily assessed in clinical settings, the equinus deformity—in terms of limited ankle dorsiflexion—appears to be effectively corrected. However, the insufficient plantarflexion kinematics observed in our study, accompanied by reduced kinetics as reported by Pierz et al. 19 and Wijnands et al., 20 may indicate underlying plantarflexor weakness. Although Achilles tendon lengthening is considered to cause plantarflexor weakness, there remains a lack of functional outcome evaluations in treated ICTEV to confirm this association. We propose that plantarflexor weakness is linked to clinically observed calf muscle atrophy, a primary characteristic of ICTEV that tends to persist or even worsen with growth and treatment. 21
Interestingly, our study also revealed excessive dorsiflexion during LR in the ICTEV group, accentuating the heel rocker mechanism. 22 This finding is particularly relevant since the Heel Rotation Center is implemented in the Heidelberg Foot Model to describe the heel rocker. 16 During weight acceptance, pretibial and inverting muscles act to restrain ankle plantarflexion and ST eversion. 22 Such heel rocker dysfunction may indicate overactivity of the tibialis anterior—a major pretibial muscle that also functions as an invertor—as well as other invertor muscles. This could be associated with the excessive inversion in the ICTEV group seen in the kinematic comparison (Figure 2).
Foot alignment and arch stiffness
In addition to LR, our results showed that treated ICTEV exhibited overall pronounced inversion with corresponding varus. However, Grin et al. 9 reported no significant differences in the mean hindfoot frontal angle during stance or swing when comparing ICTEV patients to controls. This discrepancy may arise because their parameters reflect hindfoot motion toward varus or valgus averaged over the entire stance or swing phase. In contrast, our study specifically assessed hindfoot varus during MSt and MSw, phases in which our dataset demonstrated relatively little variation in the frontal plane, ensuring the robustness of the chosen parameters for statistical tests.
This also applies to other MSt -specific parameters. MSt represents the first half of single limb support, during which the reference foot solely supports the body’s entire weight. Stability during this phase—particularly through a plantigrade foot support—is therefore crucial. 22 Based on the Midfoot Joint Center determined through functional calibration, 15 the orientation between the Ff/Hf could be more precisely assessed. Our study revealed that treated ICTEV patients exhibit increased forefoot adductus during MSt, along with hindfoot varus and adductus (i.e. internal rotation). This lever arm dysfunction within the foot, in combination with the altered hindfoot alignment, potentially impairs shock absorption in the midfoot, leading to instability, and compromised limb advancement. Supporting this, Wijnands et al. 23 and Zumbrunn et al. 24 reported impaired anterior-posterior balance control during single-leg standing in ICTEV patients.
Additionally, we found a pronounced cavus position in the MA during MSt in ICTEV patients compared with that in controls. In combination with Ff/Hf adductus, this could be necessary to maintain floor contact for greater stability, as excessive inversion and varus shifts weight laterally. When assessing cavus in the forefoot, no significant differences were found in the average position during MSt or the maximal achieved planus position during stance. However, this does not apply to cavus in the MA. In contrast, when examining the MA, both the average position during MSt and the maximal achieved planus position during stance were reduced, indicating a pronounced cavus position in the MA. Notably, the ROM required to form maximal cavus in the transition from stance to swing was significantly reduced for both, suggesting pronounced arch stiffness. The compromised compression and recoil “spring-like” mechanism of the foot arch 25 in treated ICTEV may impair energy storage and release, possibly contributing to inefficient push-off mechanics. The distinction between cavus in the MA and the forefoot may be attributed to the complex compensatory mechanisms of the forefoot, particularly through metatarsal alignment, as our study found that the forefoot remains similarly supinated and dorsiflexed during MSt compared with that in controls—supporting a correlation between forefoot supination and arch configuration. It should be noted that, due to the functional definitions of the Ff/Hf used in our study, supination and dorsiflexion of the forefoot may appear contradictory to more morphology-based descriptions.
Integrated understanding and management of deformities
Beyond the interplay between forefoot supination and arch configuration, we also proposed several additional correlations in the previous discussion, although formal interaction analyses were not performed. These include a general correspondence between increased ST inversion and hindfoot varus; the coordination between ankle and ST motion during weight acceptance, modulated by pretibial and invertor muscle activity; and a potential compensatory role of MA cavus, as well as Ff/Hf adductus, in response to inversion and varus during stance.
This is the first study to comprehensively evaluate the kinematics of posttreatment idiopathic clubfoot deformities using a foot model with functional joints for gait analysis. By distinguishing individual deformity components and associating them with specific gait phases, our findings underscore the complexity of residual abnormalities following ICTEV treatment. Although the deformities are analyzed separately, it is important to recognize that they are interdependent and kinematically coupled—a principle central to the Ponseti method, particularly in its simultaneous correction of cavus, adductus, and varus prior to addressing equinus. 6 This integrated approach, however, is not consistently applied in the context of additional interventions for managing residual or recurrent deformities. Therefore, assessing both individual procedures and their combinations is crucial for understanding their biomechanical impact.
Since our study was not specifically designed to systematically evaluate the effects of different interventions or their combination, we analyzed the influence of the most commonly performed procedures. Notably, patients who had undergone ankle and ST capsulotomy exhibited a pronounced cavus in the MA. The reduced ST inversion during MSt may appear contradictory to our earlier interpretation. However, kinematic parameters associated with functional joints did not differ significantly with respect to intervention status, suggesting that the increased MA angle may reflect a structural alteration rather than a functional change. From a morphological perspective, comparable findings have been reported radiologically. Compared with individuals initially treated with the Ponseti method, Church et al. 26 reported a pronounced cavus based on an increased talo–first metatarsal angle in individuals who initially underwent posteromedial release, while a reduced calcaneal pitch angle suggested a less cavus configuration; however, no statistical analysis was provided for the latter. They also noted an increased anteroposterior talo–first metatarsal angle, indicative of greater first metatarsal adductus—an observation not confirmed by Ferrando et al., 27 who specifically investigated posterior release. Our results also showed that individuals with additional Achilles tendon lengthening displayed a pronounced cavus position of the MA during ISw. However, this isolated finding, like the reduced inversion angle during MSt, may not reflect a functionally relevant or clinically meaningful difference.
In contrast to the study by Mindler et al., 28 who reported notable effects of anterior tibial tendon transfer—particularly during the swing phase—using the Oxford Foot Model, our results did not reveal significant differences. This discrepancy mainly stems from the underrepresentation of certain gait subphases in our analysis. While multi-segment foot models offer new insights into foot function, they also present challenges due to the extensive number of potential parameters that can be analyzed. Although we aimed to characterize treated ICTEV as comprehensively as possible by including and interpreting a broad range of parameters, certain values—especially within the swing phase—could not be robustly extracted or analyzed due to technical constraints and variability within the patient cohort. These limitations may have obscured relevant intervention-related effects.
As with the unresolved inconsistencies regarding pathogenesis, it remains unclear how structural deformities and/or muscle imbalances specifically contribute to the development of residual or recurrent components and ultimately to the functional gait deficits observed in our study. Further studies are needed to systematically assess the role of surgical interventions and their biomechanical consequences in posttreatment gait patterns.
Study limitations
In addition to the model- and cohort-related aspects discussed above, several further factors contribute to the heterogeneity of the patient group. First, we included both unilateral and bilateral cases, yet potential impairments from an affected contralateral limb in bilateral cases may lead to differences between these subgroups. Additionally, our patient cohort spans a wide age range, and previous studies suggest growth-associated changes in gait patterns.29–31 Furthermore, we did not account for relapse or overcorrection, as carried out in studies such as Grin et al., 9 McCahill et al., 11 and Böhm et al., 8 to avoid bias arising from the lack of a standardized definition and assessment criteria for these conditions, thus to provide a broader overview of gait function of treated ICTEV. Given our limited sample size, incorporating additional covariates such as laterality, age, detailed treatment variables, or current clinical status into a Linear Mixed Model was not feasible.
Conclusion
This prospective cohort study investigated foot kinematics during gait in individuals with idiopathic clubfoot initially treated with the Ponseti method, providing important prognostic insights into posttreatment foot function. The findings revealed alterations in foot alignment and mobility, particularly affecting plantarflexion, midfoot stability, and arch stiffness, impairing limb advancement during gait. By deepening the understanding of residual deformities, this study establishes a foundation for future research projects to enhance treatment strategies. To support the development of more function-oriented management approaches, future studies should integrate biomechanical and other basic science research to elucidate underlying mechanisms, alongside clinical investigations to assess therapeutic relevance.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521251369353 – Supplemental material for Kinematic characterization of residual deformities in idiopathic clubfoot initially treated with the Ponseti method: Gait analysis using the Heidelberg Foot Model
Supplemental material, sj-pdf-1-cho-10.1177_18632521251369353 for Kinematic characterization of residual deformities in idiopathic clubfoot initially treated with the Ponseti method: Gait analysis using the Heidelberg Foot Model by Qiuyue Chen, Firooz Salami, Cornelia Putz and Sebastian I Wolf in Journal of Children's Orthopaedics
Supplemental Material
sj-pdf-2-cho-10.1177_18632521251369353 – Supplemental material for Kinematic characterization of residual deformities in idiopathic clubfoot initially treated with the Ponseti method: Gait analysis using the Heidelberg Foot Model
Supplemental material, sj-pdf-2-cho-10.1177_18632521251369353 for Kinematic characterization of residual deformities in idiopathic clubfoot initially treated with the Ponseti method: Gait analysis using the Heidelberg Foot Model by Qiuyue Chen, Firooz Salami, Cornelia Putz and Sebastian I Wolf in Journal of Children's Orthopaedics
Footnotes
Acknowledgements
We thank all participating children and their families for their time and cooperation, as well as the team at the Heidelberg Motion Lab for their support during data acquisition. We also acknowledge the use of ChatGPT to assist with language refinement and Matlab figure formatting. References were managed and formatted using Zotero. All AI-assisted output was critically reviewed and verified to ensure its accuracy. For the publication fee we acknowledge financial support by Heidelberg University.
Author contributions
QC and SIW made substantial contributions to the conceptualization and methodology of the study. QC conducted the investigation, performed the analysis, and prepared the original draft of the article. FS contributed to the methodology and to the review and editing of the article. CP contributed to the investigation and participated in article review and editing. SIW supervised the project and contributed to the review and editing of the article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical considerations
This study was approved by the Ethics Committee of the Medical Faculty of Heidelberg University (reference number: S-636/2024). All procedures were conducted in accordance with the Declaration of Helsinki and institutional guidelines for human research ethics.
Consent to participate
Written informed consent to participate in the study was obtained from all participants and/or their legal guardians prior to data collection.
Data availability statement
Data may be requested from the corresponding author in anonymous format.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.