
Abstract
Purpose
Predictive factors for long-term outcome after in situ fixation for chronic slipped capital femoral epiphysis (SCFE) have so far not been systematically analysed. The aims of this study were to define predictors for long-term outcome and to assess the association between initial grade of slipping and post-slip deformities.
Methods
We studied 51 patients (60 hips) with chronic SCFE treated with in situ fixation. There were 31 males and 20 females with a mean age of 12.9 years. The mean follow-up was 39.0 years (21.1 to 56.8). Post-slip deformity was defined as abnormal alpha (a) angles in anteroposterior (AP) and lateral radiographs; AP angle of 74° and lateral angle of 63° were used as cutoffs between normal and abnormal α-angles. Harris hip score (HHS) less than 85 points was classified as a poor clinical outcome and osteoarthritis was a poor radiographic outcome.
Results
The mean slip angle was 31.7° (12° to 77°). The mean AP α-angle was 67.4° (36° to 111°) and the mean lateral α-angle was 57.1° (22° to 104°). Post-slip deformities developed in almost one-third of hips with a mild degree of slipping and in about half the hips with more pronounced degrees of slipping. The long-term outcome was good in 40 hips (67%) and poor in 20 hips. A small AP α-angle was the only independent prognostic factor for a good combined clinical and radiographic outcome.
Conclusion
Post-slip deformity, defined as an abnormally high AP α-angle, is the most important prognostic factor for poor long-term clinical and radiographic outcome in chronic SCFE treated with in situ fixation.
Keywords
Introduction
Fixation in situ has been considered the treatment of choice for chronic slipped capital femoral epiphysis (SCFE). The long-term outcome is usually good if serious complications like chondrolysis and avascular necrosis (AVN) of the femoral head are avoided.1–3 Although the rate of osteoarthritis (OA) increases with the severity of the slip, the OA rate is 15% to 25% and thus not negligible even in hips with a mild degree of slipping.2,3 One reason for the development of degenerative changes is cam-type femoral acetabular impingement (FAI), caused by post-slip deformity of the anterolateral femoral head-neck junction. The impingement between the acetabular rim and the prominent femoral metaphysis might lead to hip pain and reduced function and later development of OA.4–6 Although it would seem logical that a relationship existed between slip angle (SA) and post-slip deformity, Dodds et al 7 found that SA correlated poorly with both the anterior offset angle (a-angle) and clinical impingement. The femoral head and metaphysis undergo remodelling after SCFE,1,8,9 but there is no agreement as to the extent of remodelling. Wensaas et al 10 found a somewhat worse long-term outcome in hips with persistent post-slip deformities compared with hips in which the deformities had resolved. Thus, the associations between initial SA, post-slip deformities and long-term outcome needs further research.
In recent years, newer surgical techniques such as surgical dislocation and proximal femoral osteotomies have been proposed for moderate and severe SCFE with the purpose of avoiding post-slip deformity.11–13 Even in mild SCFE, open or arthroscopic osteoplasty of the head-neck junction has been suggested to avoid subsequent articular damage.13,14 However, no long-term studies exist to prove the benefits of these new methods. Before recommending surgical correction of minor anatomic deformities, the long-term outcome of untreated deformities should be established.
Predictive factors for good and poor long-term outcomes after treatment for SCFE have so far not been systematically analysed. Although most authors reported better radiographic outcome in hips with mild or moderate grade of slipping compared with the outcome after severe slipping,1–3 recent studies did not find any significant association between grade of slipping and clinical long-term results.15,16
Because we had retained the primary radiographs in patients who had undergone treatment for SCFE several decades ago, we were able to perform the present study. The aims were to answer the following questions:
What are the predictors for good and poor long-term clinical and radiographic outcomes after in situ fixation of chronic SCFE? What is the association between initial grade of slipping and post-slip deformities?
Patients and Methods
The study comprised 51 patients (60 hips) treated in our hospital for chronic SCFE with in situ fixation. There were 31 male (61%) and 20 female patients and their mean age at surgery was 12.9 years (8.8 to 16.7), 12.4 years in females and 13.3 years in males (p = 0.033). SCFE was unilateral in 42 patients and bilateral in nine patients (18%). In situ fixation was performed using screws or nail (usually two screws) in 30 hips and bone-peg epiphysiodesis (two allograft bone-pegs) in 30 hips. The SA was measured on the original pre-operative frog-leg lateral radiographs according to the head-shaft angle (SA) described by Southwick, 17 but the SA of the contralateral hip was not subtracted from the SA of the affected side.
At long-term follow-up, 38 patients were clinically and radiographically examined. Hip function in hips that had not undergone total hip arthroplasty (THA) was rated with Harris hip score (HHS), 18 which has a range from zero points (maximum disability) to 100 points (no disability). A HHS score of 85 points or above was classified as a good clinical result. The 13 patients who did not attend the radiographic examination were interviewed by telephone, using the HHS classification.
The long-term radiographic examination was performed with the patient supine and included anteroposterior (AP) and frog-leg lateral views of the pelvis and both hips. The AP radiograph was performed with both lower extremities placed parallel and with the patella pointing straight upward while the frog-leg lateral radiograph was taken with the affected extremity flexed at the knee 90°, the hip abducted 45° and the heel resting on the medial side of the contralateral knee. The film-focus distance was 115 cm. Evaluation of the post-slip deformity was done with measurements of the α-angles in the AP and lateral views.19,20 The measurements were performed by one of the authors (AW) and are shown in Fig. 1. The α-angle is the angle between a line connecting the centre of the femoral head (C) and the midpoint of the narrowest part of the femoral neck (A) and a line from the centre of the femoral head (C) to point B where the radius (r) of the femoral head deviates from the lateral (or anterior) outline of the metaphysis. We used normal α-angles from five previous studies on individuals without known hip disease to differentiate between normal and abnormal angles.10,20–23 The upper normal limit in each of these studies was defined as mean + 2 standard deviations (SD). The median value of the upper limits from the five studies was used as a cutoff for post-slip deformity, which was 74° for the AP α-angle and 63° for the lateral α-angle.
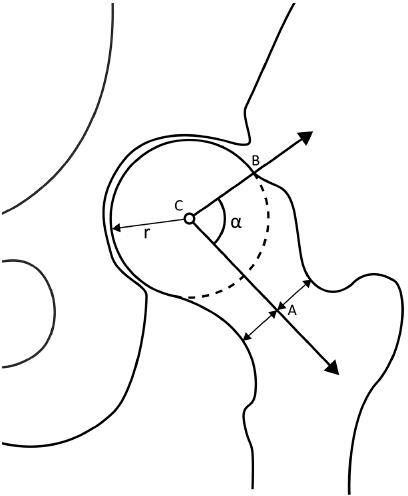
Schematic drawing, showing the anteroposterior α-angle. (
OA was defined according to Jacobsen and Sonne-Holm 24 as minimum joint space width less than 2.0 mm in the upper weight-bearing part of the hip joint. A good long-term radiographic outcome in hips with long-term radiographs was defined as no OA. A good combined clinical and radiographic outcome (all 60 hips) was defined as HHS ≥ 85 points and no OA or THA.
Statistical analysis
SPSS software (version 21) was used for the statistics (IBM, Armonk, NY, USA). Continuous variables were analysed using the independent samples t-test. Categorical data were analysed with the Chi-square test. Logistic regression was used for the analysis of predictive factors for good and poor long-term outcomes. Correlations were calculated with Pearson correlation coefficient (r). All tests were two-sided. Differences were considered significant when the p-value was below 0.05.
Results
The mean SA was 31.7° (12° to 77°). The grade of slipping was mild (SA < 30°) in 35 hips (58%), moderate (SA 30° to 49°) in 17 hips and severe (SA ≥ 50°) in eight hips. Females had significantly greater SA than males (38.8° vs 27.7°; p = 0.005).
The mean follow-up time from index surgery to the present evaluation was 39.0 years (21.1 to 56.8). There were two serious complications, both in hips with severe grade of slip; one hip developed chondrolysis and the other developed avascular necrosis (AVN) of the epiphysis. In these two hips, α-angles were not measured. In the remaining 58 hips, α-angles were measured at the time of long-term follow-up in 37 patients (44 hips). In 12 patients (14 hips) who did not attend the long-term radiographic examination, the α-angles were measured on the last follow-up radiographs that had been taken during follow-up in adolescence (when the proximal femoral physis was closed) or young adulthood, at a mean age of 21.3 years (16.1 to 31.7). Nine hips lacked lateral radiographs at this follow-up.
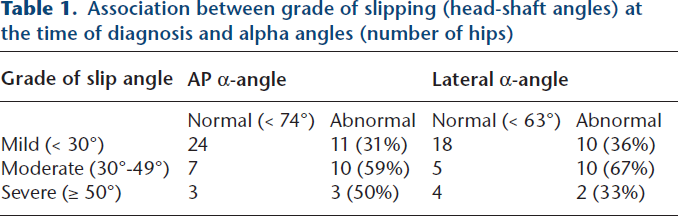
The mean AP α-angle was 67.4° (36° to 111°) and the mean lateral α-angle was 57.1° (22° to 104°). We found a significant correlation between the two α-angles (r = 0.53; p < 0.001). The mean AP α-angles in hips with mild slip, moderate slip and severe slip were 63.1°, 74.5° and 72.8°, respectively; the difference was not significant (p = 0.368). The mean lateral α-angles according to the same slip severity groups were 55.1°, 63.9° and 49.5°, respectively (p = 0.290). Abnormal AP α-angles occurred in 41% of the hips and abnormal lateral α-angles were seen in 45%. Approximately one-third of the hips with a mild grade of slipping had post-slip deformities, whereas this occurred in about half the hips with more pronounced degrees of slipping (Table 1).
Association between grade of slipping (head-shaft angles) at the time of diagnosis and alpha angles (number of hips)
Ten of the 60 hips (17%) had undergone THA. Of the patients who attended the long-term radiographic follow-up, five patients (six hips) had undergone THA, and of those who were interviewed by telephone, three patients (four hips) had THA. Of the 45 hips with long-term radiographic follow-up, OA was found in ten hips (22%) (Table 2). Although there was a trend to more frequent OA in severe slips compared with moderate and mild slips (43% vs 15% and 20%, respectively), the difference was not statistically significant. Table 2 shows that hips with abnormal AP α-angles (≥ 74°) had significantly more poor long-term outcomes (Fig. 2) compared with hips with normal AP α-angles (37% vs 8%). A similar trend occurred regarding the lateral α-angle.
Association between grade of slipping (head-shaft angles) at the time of diagnosis, α-angles and long-term radiographic and clinical outcomes
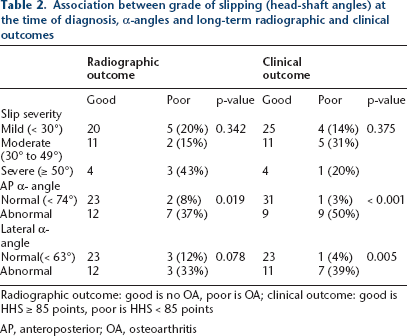
Radiographic outcome: good is no OA, poor is OA; clinical outcome: good is HHS ≥ 85 points, poor is HHS < 85 points
AP, anteroposterior; OA, osteoarthritis
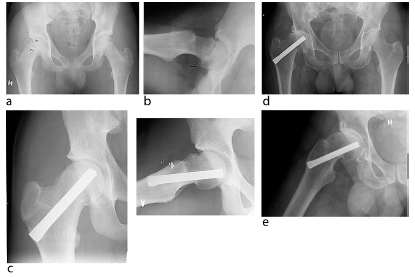
Radiographs of a male patient aged 16.7 years at primary treatment. (
Long-term clinical outcome in the 50 hips without THA was good (HHS ≥ 85 points) in 40 hips. There was no significant difference according to degree of initial slipping (Table 2). Hips with abnormal AP α-angle had significantly worse clinical outcome compared with hips with normal AP α-angle (50% vs 3% poor results). Abnormal lateral α-angles were also associated with worse clinical outcome (Table 2). The mean HHS of the 50 hips was 94.1 points (53 to 100), 67.8 points in patients with OA and 95.7 points in those without OA (p < 0.001). There was a very good correlation between HHS and OA (r = 0.67; p < 0.001). No hips with HHS ≥ 85 points had OA. There was agreement in 90% of the hips (good radiographic and clinical outcomes in 31 hips and poor outcomes in four hips). In four hips with discrepancy, the clinical outcome was poor (HHS 71 to 83 points) while the radiographic outcome was good (no OA).
Good combined long-term outcome (good radiographic and good clinical outcome and no THA; Fig. 3) occurred in 40 of the 60 hips (67%). There was no significant difference between hips that had been treated with screws or nails compared with hips that had been treated with bone-pegs (p = 0.392). Possible prognostic factors for good and poor combined long-term outcome are shown in Table 3. Using univariable logistic regression, these predictors for poor outcome were identified: female gender; right-sided hip; high AP α-angle; and high lateral α-angle. When the factors with a p-value less than 0.10 were analysed with multivariable logistic regression, a high AP α-angle was the only independently significant predictor for poor long-term outcome (Table 3).
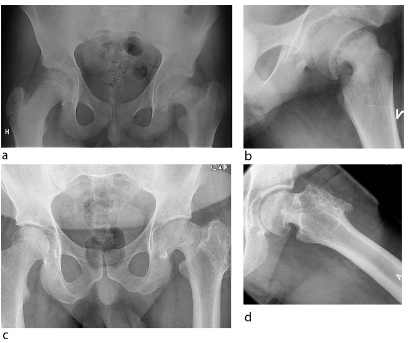
Radiographs of a male patient aged 14.0 years at diagnosis. (
Possible prognostic factors for long-term outcome (combined clinical and radiographic outcome) in all 60 hips, analysed with logistic regression
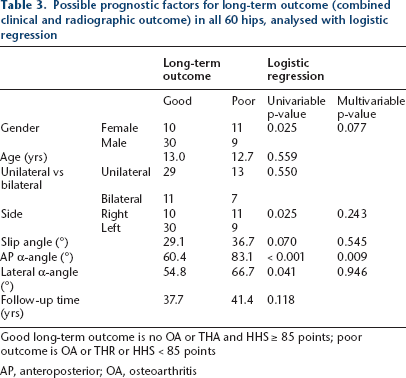
Good long-term outcome is no OA or THA and HHS ≥ 85 points; poor outcome is OA or THR or HHS < 85 points
AP, anteroposterior; OA, osteoarthritis
Discussion
The most important finding of the present study with 39 years of follow-up was that post-slip deformity, defined as an abnormally high AP α-angle, was the most important risk factor for poor clinical and radiographic outcome in chronic SCFE treated with in situ fixation. There was a trend to more frequent development of post-slip deformities in hips with severe and moderate initial SA, but abnormal AP α-angle occurred in almost one-third even in hips with a mild grade of slipping.
There were some limitations of the study. First, the small number of patients with a severe grade of slipping (eight hips, of which only six had available α-angles) reduced the reliability of the analysis of association between grade of slipping, post-slip deformity and long-term outcome (possible type-2 error). Second, long-term radiographs were not available in one-fourth of the patients. However, we think the long-term outcome was reliably calculated, since we used clinical outcome measured by HHS in patients without radiographs. This was done because there was a close association between clinical evaluation and radiographic results in patients who had both evaluations. Third, the reliability of using α-angles as predictors could be questioned, since there is substantial variation in the upper normal limit, defined as mean + 2 SD of the values in individuals without hip disease10,20–23 and a rather large inter-observer variation in measurements of α-angles has been reported. 10 The main strength of the study was the long follow-up period, which made it possible to obtain a reliable analysis of the frequency of OA and THA.
The mean AP α-angle in hips that had been treated for SCFE with fixation in situ was 67° in the present study, which is considerably less than 86° reported by Fraitzl et al. 6 Since both studies contained most hips with mild slips, we see no obvious reason for this discrepancy. A better accordance occurred in the lateral α-angle, as the present mean value in hips with previous SCFE was 57°, which is similar to the 55° and 59°, respectively, reported by Fraitzl et al 6 and Dodds et al. 7 Previous studies have not provided information about the frequency of post-slip deformities.6,7,25 Although there was a trend to more frequent post-slip deformities after moderate and severe grades of slipping in the present study, the differences were not statistically significant, which is in agreement with Dodds et al, 7 who found that the SA correlated poorly with the lateral α-angle and FAI at the six-year follow-up. We found a surprisingly high frequency of abnormal AP α-angles (31%) even in hips with mild slips. Since all patients had femoral head-neck abnormalities at the time of primary treatment, the post-slip deformities must have improved significantly in the hips with normal α-angles. This is in accordance with previous studies that reported a considerable potential of remodelling after SCFE, involving both resorption of the supero-lateral prominent part of the metaphysis and reduction in SA.1,8,9
Most patients have a good clinical outcome after in situ fixation of SCFE. In previous studies containing a mixture of acute and chronic slipping, the mean HHS was 96.6 points after a mean follow-up time of six years 7 and 85 to 90 points after 16 to 20 years.15,16 We had a mean HHS of 94 points after a much longer follow-up. This high score would naturally have been lower if the pre-operative HHS of the ten hips with THR had been available. There was no significant association between SA severity and clinical outcome (HHS), which confirms the experience of previous studies with mean follow-up of 16 to 20 years.15,16 Previous long-term studies have not included α-angles, which were significant predictors for poor clinical outcome in the present study. Studies with a shorter follow-up (6 to 14 years) confirm the importance of post-slip deformity as risk factor for pain, dysfunction and clinical signs of FAI.6,7,25
When comparing the frequency of OA, only studies with follow-up of more than 20 years should be considered. In the present study, the frequency of OA in hips with fixation in situ was not higher after moderate slipping than after mild slips (15% vs 20%). Similar experience has been reported by others.1,2,26 In severe slips, our OA rate of 43% is in accordance with previous reports,1,27 but the small number of patients with severe slips could make these results less reliable. Abnormal AP α-angle was associated with poor radiographic outcome, indicating that post-slip deformities could be more important for the development of OA than initial degree of slipping.
For an adequate analysis of long-term outcomes, both clinical and radiographic results should be evaluated, as was done in the present study. Pain and reduced function are the most important reasons for poor clinical outcome, and these factors can be evaluated in a telephone interview. It seemed that the main reason for some patients not wanting to take radiographs was that they had high HHS scores and thus little or no complaints regarding their hips. Since we found a very good accordance between clinical and radiographic results in the other patients, we think clinical evaluation with HHS provides a realistic estimate of outcome. The advantage was that we obtained long-term outcome in 100% of the patients. The combined outcome analysis revealed that SA was not a significant predictor for outcome. When the possible prognostic factors were tested in multivariable analysis, only AP α-angle remained a significant risk factor for long-term outcome.
What is the clinical significance of the present findings? We think all hips with chronic (stable) slips, at least those with SA less than 60° should be treated with in situ fixation, because these hips have a good long-term outcome with an OA rate of approximately 20%. Patients with hip complaints, positive clinical FAI signs and high α-angles after in situ fixation should be considered for reconstructive surgery, according to recently developed techniques.14,28 However, long-term results are required to prove the benefits of such surgery and our present results would be valuable for comparison.
In conclusion, the answers to the questions in the introduction are:
Post-slip deformity (abnormally high AP α-angle) is the most important prognostic factor for poor long-term clinical and radiographic outcome in chronic SCFE treated with in situ fixation. Post-slip deformities develop in almost one-third of hips with a mild degree of slipping (< 30°) and in about half the hips with more pronounced degrees of slipping.
Footnotes
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
The authors have no conflicts of interest or funding to disclose.
All patients gave their informed consent prior to inclusion in the study, which was approved by the Regional Ethical Committee and Data Inspectorate.