
Abstract
Purpose:
We aimed to determine which variables were associated with persistent symptoms or need for further surgery in patients treated with in situ fixation for stable slipped capital femoral epiphysis. We hypothesized that patients with greater proximal femoral deformity would require revision surgical intervention.
Methods:
We prospectively collected data on stable slipped capital femoral epiphysis patients who underwent in situ screw fixation at a single institution. Demographic and radiographic information, as well as patient-reported outcomes, were collected.
Results:
Forty-six patients (54 hips) with an average follow-up of 3.5 years (range: 2.0–8.5) and mean pre-op Southwick slip angle of 40.5° ± 19.4° were studied. We observed one complication following the index procedure (2%). Twelve hips (22%) went on to have a secondary procedure 2.7 ± 2.2 years after the index surgery. Severe slips were 14.8× more likely to undergo a secondary procedure than mild and moderate slips (p < 0.001). We found no correlation between slip severity and patient-reported outcomes (p > 0.6). Hips requiring a secondary procedure had significantly lower Hip disability and Osteoarthritis Outcome scores (76.8 ± 18.4) at final follow-up compared to hips that did not require additional surgery (86.8 ± 15.7) (p = 0.042).
Conclusion:
With minimum 2-year follow-up, 22% of patients required a secondary surgery. Patient-reported outcomes did not correlate with slip severity, but were found to be significantly higher in slipped capital femoral epiphysis patients that did not require a secondary procedure. Prophylactic treatment of all slip-related cam deformity was not found to be necessary in this prospective cohort. Patients with moderate-to-severe slips may require secondary surgery.
Level of Evidence:
Level II
Introduction
Slipped capital femoral epiphysis (SCFE) is a commonly treated pediatric condition occurring in 1 in 10,000 adolescents in the United States. 1 SCFE is characterized by the posterior and inferior displacement of the femoral epiphysis on the metaphysis resulting in a varus, extension, and external rotation deformity of the proximal femur. 2 This condition may occur gradually and present in a chronic nature or may be associated with trauma and present acutely. Regardless, the proximal femoral deformity may result in the development of a cam lesion of the anterolateral proximal femur and subsequent femoroacetabular impingement (FAI).
Post-SCFE FAI has been demonstrated to result in both pre-arthritic dysfunction 3 as well as chondral damage 4 and ultimately secondary osteoarthritis of the hip. 5 SCFE is traditionally treated with in situ screw fixation to stabilize the capital femoral epiphysis and prevent further slip. However, given the concern regarding the consequences of post-SCFE FAI, recent studies have recommended that in addition to stabilization, slip-related cam deformity should also be treated acutely to correct FAI and to prevent degenerative changes leading to secondary osteoarthritis.6–9
In light of these current concepts, the purpose of this study was to prospectively evaluate radiographic, clinical, and patient-reported outcomes after in situ screw fixation for SCFE with a minimum of 2-year follow-up. We aimed to determine which radiographic or clinical variables were associated with persistent symptoms or need for further surgery. We hypothesized that patients with greater proximal femoral deformity (larger Southwick slip angle or larger alpha angle) would require further surgical intervention.
Methods
After obtaining institutional review board approval our department began a prospective SCFE registry of all consecutive patients starting in 2013. For this study, we queried this registry for all patients treated for a stable SCFE with in situ screw fixation and minimum 2-year follow-up. This query yielded 83 patients (99 hips). Thirty-two patients (39 hips) were excluded as lost to follow-up, these subjects were greater than 2 years from surgery, but had not come in for a clinic visit at 2 years or later. Five patients (six hips) were excluded for missing data. Stable SCFE patients were defined by their ability to weight bear on the affected limb, with or without crutches as per the traditional Loder classification. 10 Age, gender, side affected, duration of symptoms, revision procedures, and the Hip disability and Osteoarthritis Outcome Score (HOOS) as well as the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) were collected. Chronicity of symptoms were characterized as acute when duration of symptoms was less than or equal to 3 weeks prior to initial clinic visit; chronic when symptoms were present for greater than 3 weeks; and acute-on-chronic when symptoms were present for greater than 3 weeks, but presenting with a sudden exacerbation of pain.
Patients underwent in situ screw fixation with one or two screws the number of screws placed was based on the treating surgeon’s discretion. Radiographic data collected included the Southwick slip angle (SSA), the articular trochanteric distance (ATD), and the alpha angle. SSA and ATD were measured pre-operatively and at most recent follow-up. Alpha angle was measured on the most recent follow-up AP radiograph as well as the frog radiograph, if available. The treatment algorithm at this institution for stable SCFE is to treat them all with in situ screw fixation. In moderate and severe cases, the family is counseled that they may require an additional osteochondroplasty or corrective osteotomy. This additional procedure is performed, if symptoms dictate, at a later date after the SCFE has had time to heal. This approach has been adopted to decrease the likelihood of avascular necrosis (AVN).
Basic descriptive statistics are reported. Due to the differences in the cohort sizes between subjects that required a secondary procedure and those that did not, comparisons of categorical data between those groups were evaluated with the Mann–Whitney U test. Categorical data were evaluated with Pearson’s chi-square or Fisher’s exact test. The Wilcoxon signed ranks test was used to evaluate the change in patient-reported outcomes over time. Correlations between continuous variables were evaluated with Spearman’s rho (rs). Sex, age at initial surgery, body mass index at initial surgery, acuity, pre-operative SSA, and pre-operative ATD were tested for their relationship with revision surgery. Variables related to revision surgery at a significance level of p < 0.1 (acuity, pre-operative SSA, and pre-operative ATD) were included in a binary logistic regression model to determine predictors of revision surgery. Statistical analysis was conducted using SPSS (version 26; IBM, New York, NY). Statistical significance was defined as p < 0.05.
Compliance with ethical standards
Conflict of interest
Each author certifies that they have no commercial associations (e.g. consultancies, stock ownership, equity interest, and patent/licensing arrangements) that might pose a conflict of interest in connection with the submitted article.
Funding
No external funding was received for this study. This study was supported by our institution.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This study was reviewed and approved by our institutional review board.
Informed consent
All subjects included in this study underwent a formal consent process and written consent was collected from each patient.
Results
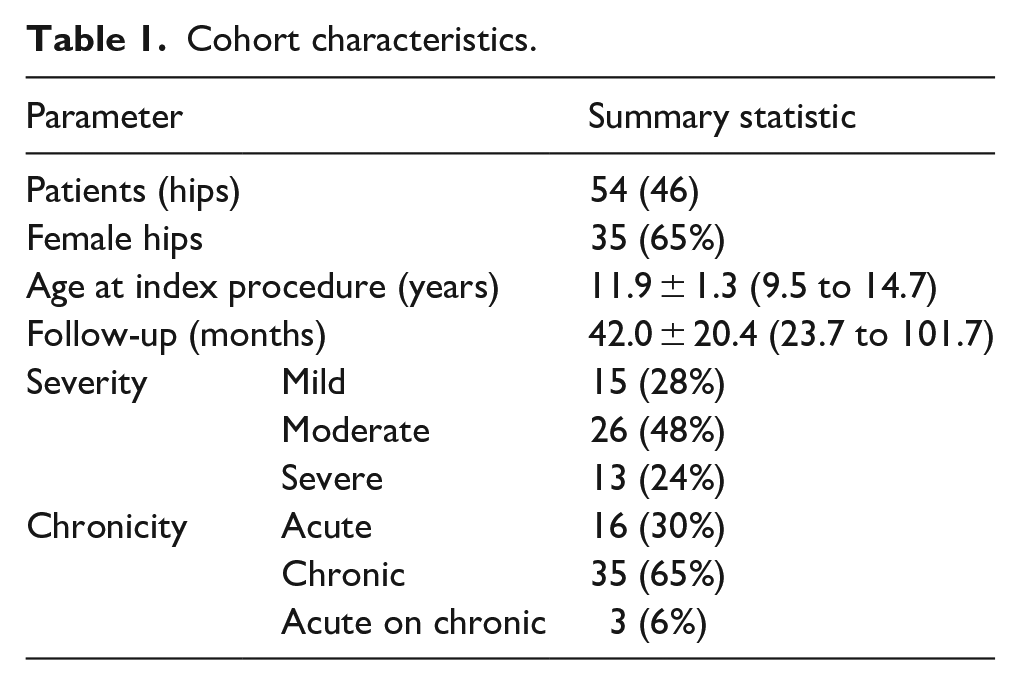
Fifty-four hips in 46 patients were studied. Thirty-five hips (65%) were in females. The index procedure was performed at a mean of 11.9 ± 1.3 years of age (range 9.5–14.7). Mean follow-up was 42.0 ± 20.4 months (range: 23.7–101.7). Cohort characteristics can be found in Table 1.
Cohort characteristics.
Patients had a mean pre-operative SSA of 40.5° ± 19.4° (range: 11°–101°) and final follow-up mean SSA of 27.2° ± 12.0° (range: 2°–59°). Two hips were excluded from final follow-up SSA and alpha angle measured on the frog view because they did not get a frog radiograph at that visit. Mean alpha angle measured on the frog lateral film at final follow-up was 68.5° ± 25.0° (range: 38°–124°) and mean alpha angle measured on the AP at final follow-up was 80.2° ± 23.2° (range: 37°–126°). Pre-operative SSA was correlated with SSA at final follow-up (rs = 0.32, p = 0.021), alpha angle at final follow-up when measured on both the AP radiograph (rs = 0.277, p = 0.044), and the frog radiograph (rs = 0.376, p = 0.006). Pre-operative SSA was inversely correlated with pre-operative ATD (rs = −0.338, p = 0.012). 89% (48/54) of hips had cam-type FAI defined as an alpha angle ≥ 50° at most recent follow-up.
The majority of hips in this cohort were treated with fully threaded screws (44/54). Three hips (7%) were treated with a partially threaded screw. Seven hips (13%) were treated with telescoping screws. Two hips treated with fully threaded screws were treated with two screws per hip, hips treated with partially threaded screws or telescoping screws were treated with one screw each. Both hips treated with two screws were severe chronic slips and both went on to have a subsequent Imhauser procedure. For one of these hips, the Imhauser procedure was performed approximately 7 months post in situ screw fixation. The other hip treated with two in situ screws underwent an Imhauser procedure 5.9 years post in situ screw fixation.
None of the hips in this cohort developed AVN. One hip (2%) developed symptomatic osteoarthritis (OA) following the initial procedure but has not undergone additional treatment (Figure 1). Mean HOOS and WOMAC scores at final follow-up were 84.6 ± 16.7 and 87.9 ± 14.8, respectively. There was no correlation between slip severity and patient-reported outcomes. SSA in degrees compared to the HOOS resulted in a correlation coefficient of rs = −0.009, p = 0.95, when compared to WOMAC the correlation coefficient was rs = −0.057, p = 0.684.
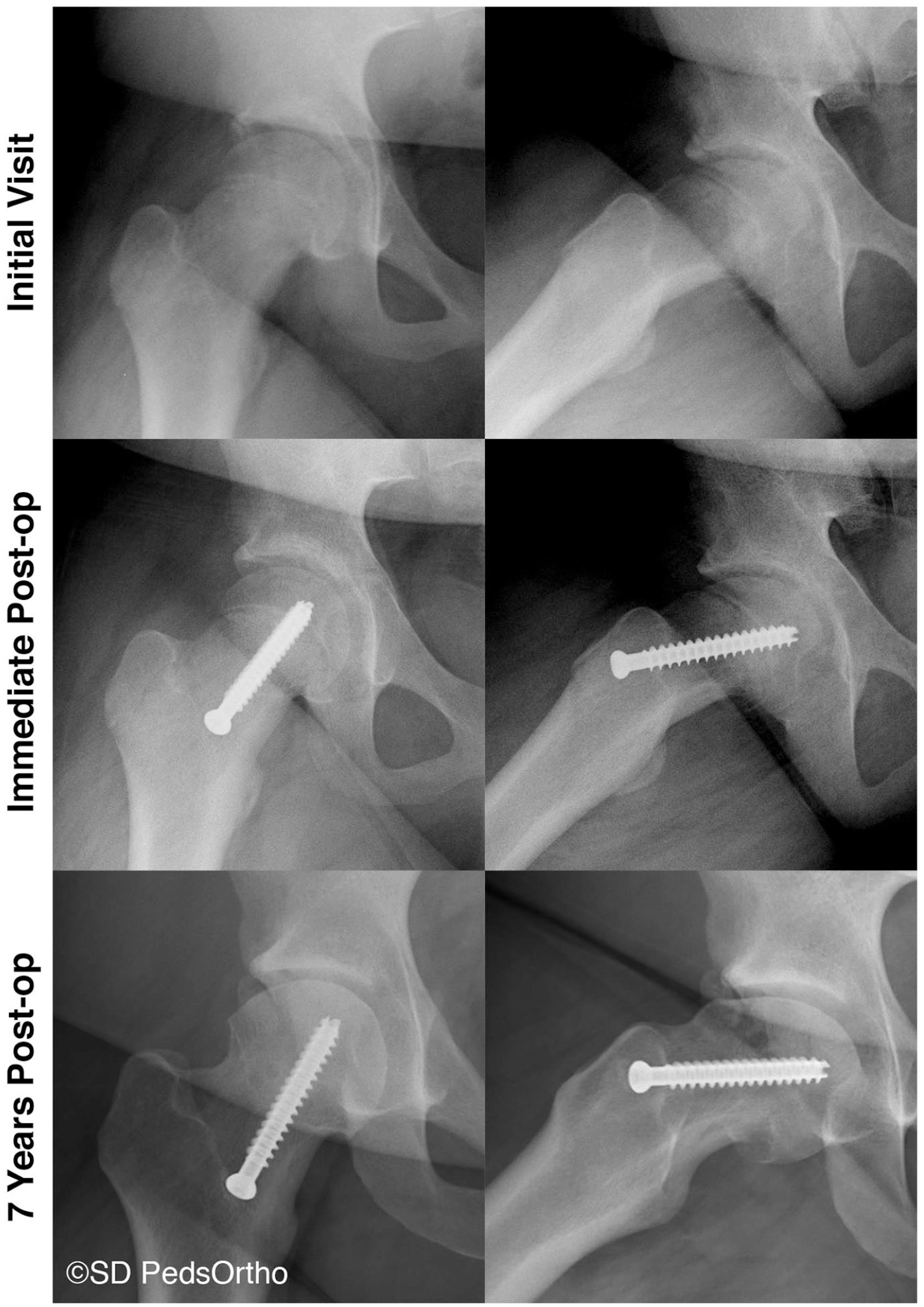
AP and frog radiographs of an 11.3-year-old female that went on to develop symptomatic osteoarthritis (daily pain that is not improved with NSAIDs or rest) following in situ screw fixation for a mild (pre-operative SSA measured at 34°) SCFE.
Twelve hips (22%) went on to have a secondary procedure at an average of 2.7 ± 2.2 years after the index surgery (range: 0.2–6.5 years). These were performed to correct residual deformity or limited hip range of motion (ROM) and persistent pain due to impingement with activities of daily living. No visual analogue scale was used to quantify pain. Limited hip ROM was defined as <90° of hip flexion and <10° of internal motion. Of the 12 hips that went on to have a secondary procedure, four (33%) were moderate slips and the remaining eight (66%) were severe. Acuity, pre-operative SSA, and pre-operative ATD were entered into a binary logistic regression model which indicated that the only data point that we collected that was a significant predictor of a secondary procedure was pre-operative SSA, as pre-operative SSA increased, the likelihood of requiring a secondary procedure increased (Exp(B) = 1.08 (95% CI: 1.014–1.15) (p = 0.017)). Seven hips (13%) underwent an Imhauser intertrochanteric osteotomy to correct residual proximal femoral deformity. Five hips (9%) underwent an osteochondroplasty, four of these had a greater trochanter transfer at the time of the osteochondroplasty, three underwent a labral repair at the time of the osteochondroplasty. Hips that underwent a revision procedure had longer follow-up (54.4 ± 27.4 months vs 38.5 ± 16. months, p = 0.029), lower HOOS score (76.8 ± 18.4 vs 86.8 ± 15.7, p = 0.042), increased pre-operative Southwick angle (61.1° ± 21.7° vs 34.6° ± 14.1°, p < 0.001), decreased pre-operative ATD (11.8 ± 7.0 mm vs 21.2 ± 6.4 mm, p < 0.001, and increased alpha angle, as measured on the frog radiograph, at final follow-up (84.9° ± 25.0° vs 64.0° ± 23.3°, p = 0.028) compared to hips that did not require revision surgery. WOMAC was similar among hips that underwent a revision procedure (83.4 ± 16.1, range: 50–100) compared to those that did not (89.2 ± 14.3, range: 47.5–100) (p = 0.091). Hips that underwent a revision procedure saw a slight boost in HOOS and WOMAC scores from pre-revision to final follow-up, but this was not statistically significant (Table 2). Eight of the 12 hips that underwent a revision procedure were classified as severe slips; the remaining four were moderate slips. 83% (10/12) of hips that underwent a revision procedure had cam-type FAI at most recent follow-up. Mean SSA, ATD, and alpha angle for hips that underwent a revision procedure can be found in Table 3.
Patient-reported outcome (PRO) scores in secondary procedure cohort.
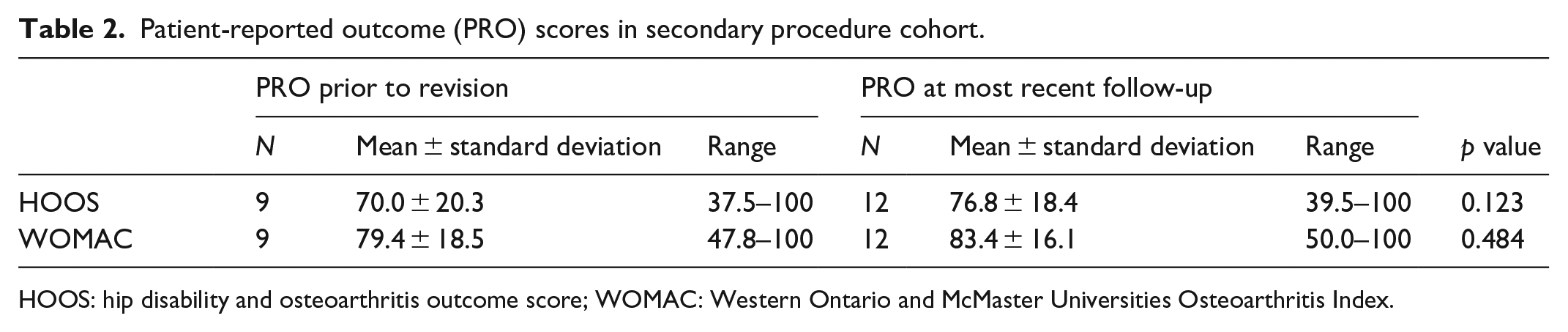
HOOS: hip disability and osteoarthritis outcome score; WOMAC: Western Ontario and McMaster Universities Osteoarthritis Index.
Radiographic measures for subjects that underwent a revision procedure.
SD: standard deviation.
Significantly lower than pre-operative (p = 0.003).
Significantly lower than pre-revision (p = 0.018).
Significantly higher than pre-revision (p = 0.045).
Six of the twelve hips that underwent a secondary procedure had a complication from the secondary procedure, four of which were grade III complications that required additional surgical intervention. There were three cases of implant failure (two underwent implant revision) (Figure 2), two cases of malpositioned implants, and one case of symptomatic implants, which were subsequently removed. Both malpositioned implants were instances of the blade plate perforating the proximal femoral cortex; in one case, this was noticed during the procedure and the blade plate was replaced with a locking plate; in the second case, the malpositioned implant was noticed during post-operative imaging and was sent back to the surgical suite for implant revision the following day.
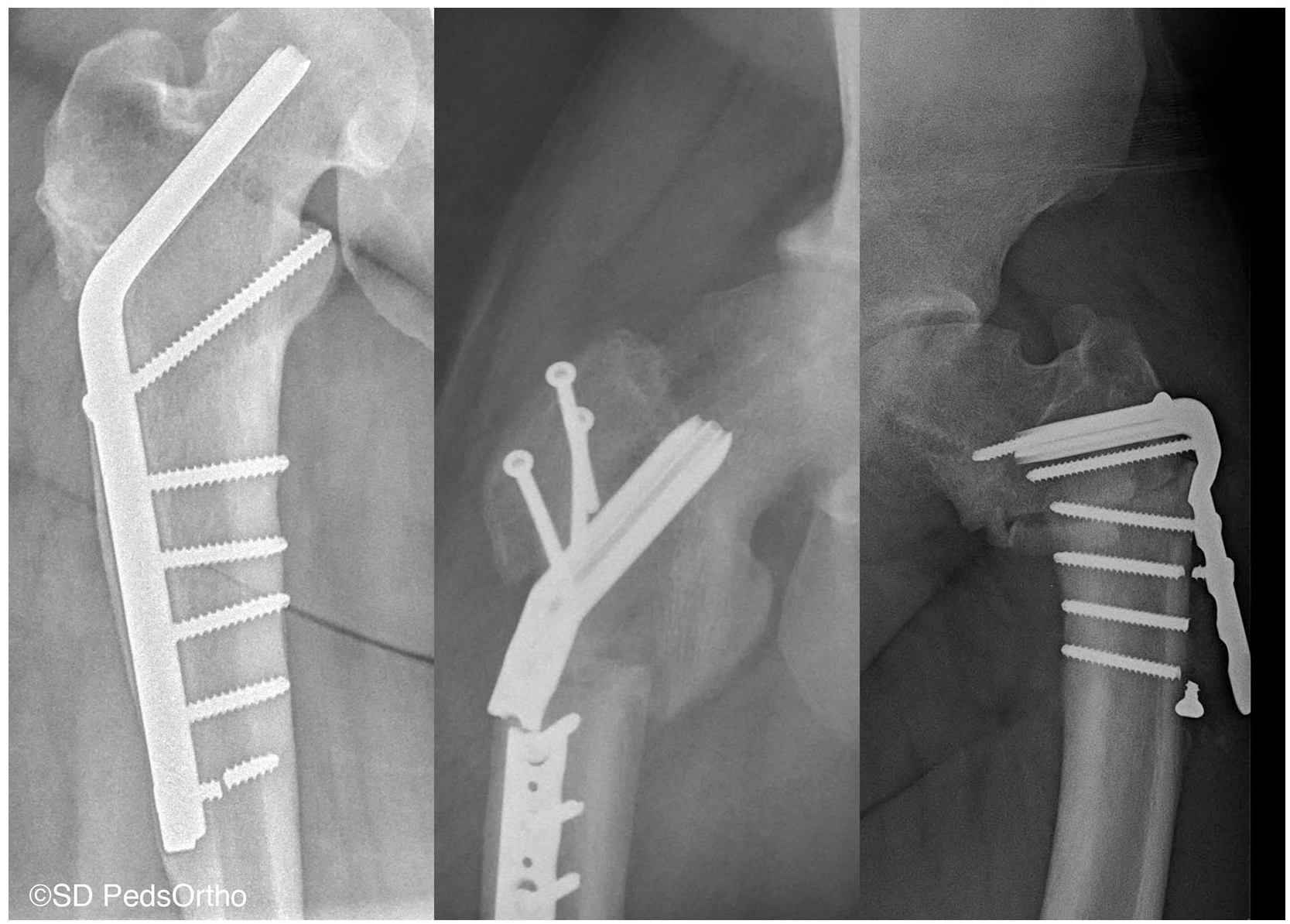
AP radiographs of the three implant failures in our cohort.
Discussion
In situ fixation has long been considered the preferred treatment for SCFE with historically favorable long-term outcomes. 11 While controversy exists around the optimal treatment of the unstable SCFE and attempts at realignment of the femoral epiphysis, stable SCFEs can be successfully treated with single screw in situ fixation with good function and low rate of complications. 12 Even at 18-year follow-up, mild and moderate SCFEs have been demonstrated to have good functional and radiographic outcomes. 3
There still remain, however, those SCFE patients that fail to do well after in situ stabilization. FAI is of concern, and it has been a well-established etiology of secondary hip arthritis that can lead to rapid joint degeneration and arthroplasty at less than 50 years of age. 13 The proximal femoral deformity introduced by SCFE results in a cam-type FAI and the potential for progressive articular damage leading to osteoarthritis. A case series described by Leunig et al. 4 documented labral and acetabular cartilage injury varying from chondromalacia to full-thickness cartilage loss in patients undergoing open treatment of SCFE. Some of these patients had only been symptomatic for a few weeks. Later data from their institution redemonstrated early cartilage damage in SCFE patients being treated with in situ screw fixation with concomitant arthroscopic treatment of the cam deformity. 7 Their conclusions were that early treatment of the cam deformity, even at the time of physeal stabilization, is advisable to prevent further chondral damage.
Despite these findings, there has not been great evidence to predict development of FAI after SCFE. Dodds et al. 14 examined 49 hips at a mean follow-up of 6.1 years and reported on severity of slip and long-term rates of impingement. Although one-third of their group developed clinical impingement, they found no association of Southwick slip angle with clinical impingement or with alpha angle.
In our series, we show similar outcomes to previously published data on in situ screw fixation of SCFE with a minimum of 2 years of follow-up. Patient-reported outcome scores were overall favorable. Our institution typically follows the advice of Sikora-Klak et al. 15 when treating severe, stable slips, in that the slip is initially treated with in situ screw fixation and allowed to heal with a triplane proximal femoral osteotomy performed at a later date to address residual symptomatic deformity (Figure 3). This accounts for the majority of our 22% reoperation rate. Hips that required reoperation had a 10 point decrease in HOOS scores at final follow-up as compared to those who did not require reoperation (p = 0.042). Similarly, the patients that required reoperation had a nonsignificant, positive change from pre-operative to post-operative outcome scores. This potentially reflects that the patients that underwent a secondary procedure in this cohort presented with limitations related to their post-SCFE deformity that helped serve as an indication for deformity correction although our cohort of revised hips is likely underpowered to detect a statistically significant difference.
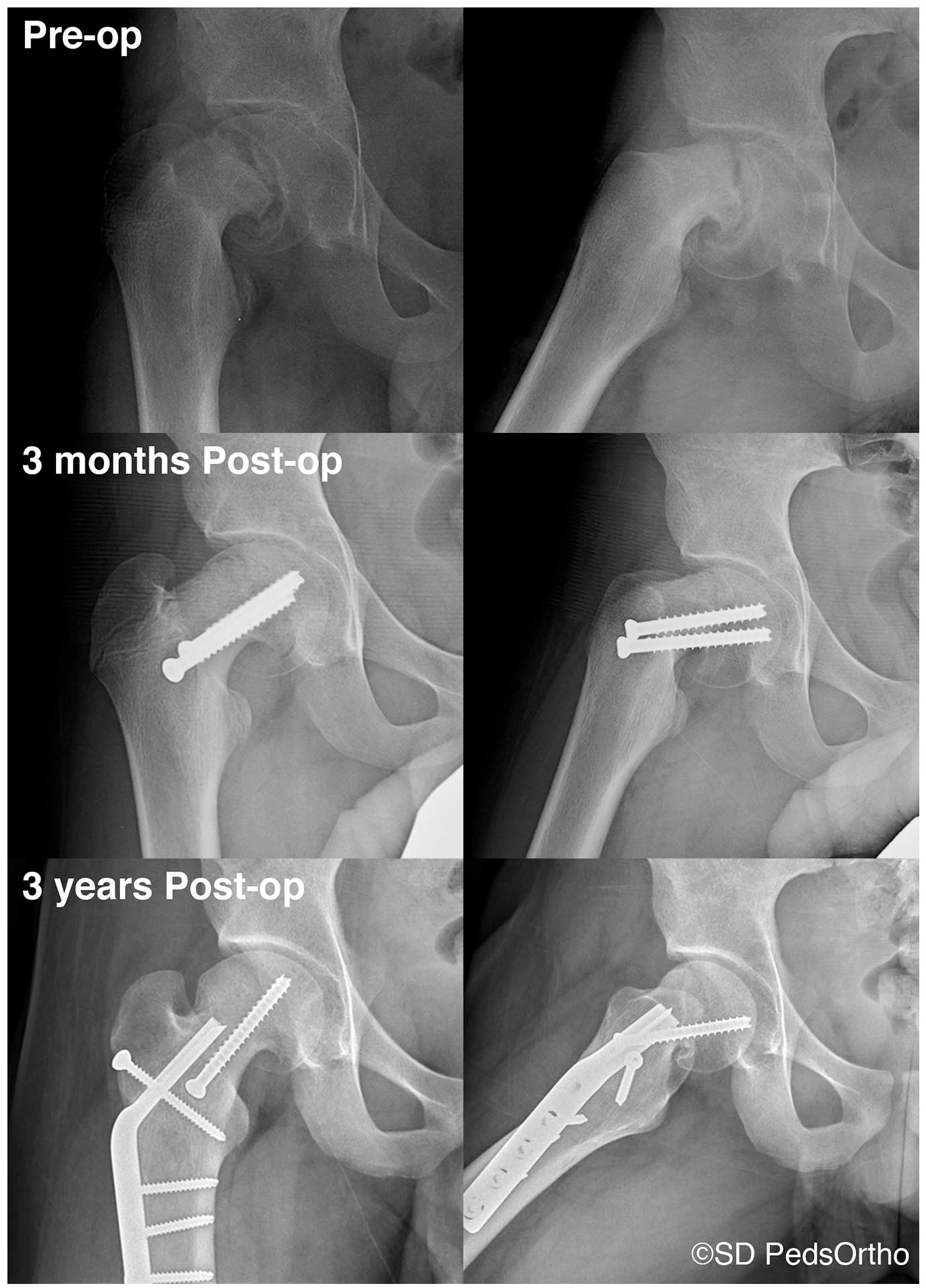
A case example of a 12-year-old male with a severe, stable, SCFE treated with in situ screw fixation and a subsequent triplane proximal femoral osteotomy performed seven months after the index procedure.
Indicative of greater slip severity in the reoperation group, post-operative alpha angles were significantly higher compared to patients who did not require reoperation. This is likely reflective of the limited capacity of the Imhauser procedure to affect intracapsular deformity. 9 It is possible that a subcapital realignment, such as the modified Dunn procedure, would be more beneficial in this group of severe, stable slips. Lerch et al. reported on long-term outcomes following the modified Dunn procedure in severe SCFE, noting excellent patient-reported outcomes (HHS: 94, HOOS: 91, UCLA: 8) at 9 years follow-up. 16 However, this comes with an increase in complexity, and a concern for osteonecrosis. The authors in the above study demonstrated a low AVN rate of 5%, although other studies report much higher AVN rates of 23–29%.15,17,18 There is some thought that this is related to the surgeon’s experience with the procedure. 17 If a low rate of osteonecrosis can be managed, the modified Dunn procedure allows for significantly greater improvement in post-operative deformity, comparable to the contralateral, normal hip, and should be considered in the context of severe slips.16,18,19
This study has some limitations. There is no adequate control group. Although we do compare cohorts of patients who did and did not require reoperation, this group was small and likely underpowered to detect differences in outcomes. In addition, although our overall cohort was large, this was divided into groups with varying degrees of severity and chronicity, making comparisons difficult. We report on medium term follow-up of average 3.5 years. It is likely that increasing the length of follow-up would result in additional patients requiring reoperation. Similarly, we have a 39% loss to follow-up rate, which may underestimate the number of hips requiring additional procedure. In addition, one of the concerns with delaying acute correction of a moderate or severe slip is the development of early degenerative changes. Our follow-up of 4 years is likely too short to identify early degenerative changes and hip survivorship.
However, despite these limitations, our study demonstrates that the majority of children with stable SCFE can be managed with in situ pinning with excellent patient-reported outcomes at mid-term follow-up. Severe slips were more likely to require revision surgery for deformity correction and symptomatic FAI. Prophylactic treatment of all slip-related cam deformity was not found to be necessary in this prospective cohort. Long-term follow-up in a larger cohort of severe stable slips is required to identify the group of patients who are likely to benefit from acute deformity correction.
Footnotes
Authors’ Note
This study was conducted at the Rady Children’s Hospital-San Diego, Encinitas, CA, United States.
Author contributions
C.A.D., J.D.B., and V.V.U. contributed to study design; C.A.D., R.B., S.G.B., and J.D.B. contributed to data acquisition; J.D.B. contributed to analysis; and C.A.D. and V.V.U. contributed to interpretation of data. All authors were actively involved in the drafting and revision of the manuscript and have provided final approval for its submission.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: C.A.D., R.B., S.G.B., and J.D.B. have nothing to disclose. V.V.U. has the following disclosures: DePuy, a Johnson & Johnson Company: Paid consultant; EOS Imaging: Research support; Imagen: Stock or stock Options; nView: Research support; Orthofix, Inc.: Paid consultant; OrthoPediatrics: IP royalties, Paid consultant, and Research support; and Wolters Kluwer Health—Lippincott Williams & Wilkins: Publishing royalties, financial, or material support.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Division of Orthopedics, Rady Children’s Hospital-San Diego. No external funding was received for this study.