
Abstract
Purpose:
The aim of this expert consensus study was to establish consensus on the treatment of different types of slipped capital femoral epiphysis and on the use of prophylactic screw fixation of the contralateral unaffected side.
Methods:
In this study, a four-round Delphi method was used. Questionnaires including all possible theoretical slip scenarios were sent online to 14 participants, experienced in the field of children’s orthopedics and in the treatment of hip disorders in children.
Results:
In-situ fixation was considered to be the first treatment choice in all types of mild slip scenarios and in moderate, stable ones. Performing in-situ fixation was not favored in moderate, unstable, and in all severe slip scenarios. In moderate to severe, unstable slip scenarios, there was consensus on the use of gentle closed or open reduction and internal fixation. Any consensus was not established in the optimal treatment of severe, stable slips. There was also consensus on the use of prophylactic screw fixation of the contralateral side in case of co-existing endocrine disorder and younger age.
Conclusions:
The establishment of consensus on the treatment of all types of slipped capital femoral epiphysis even among the experienced surgeons does not seem to be possible. The severity of the slip and stability of the slip are the primary and secondary determinants of the surgeons’ treatment choices, respectively. In-situ fixation is still the preferred treatment option in several slip types. Gentle capital realignment by closed or open means is recommended in displaced, unstable slips. Prophylactic screw fixation of the contralateral side is indicated under certain circumstances.
Level of evidence:
level V.
Introduction
Slipped capital femoral epiphysis (SCFE) is a major challenging pediatric hip disorder with a worldwide increasing incidence. 1 The aims of the treatment are early stabilization of the epiphysis on the femoral neck in order to prevent further slipping and avoidance of complications like chondrolysis, osteonecrosis of the femoral head (ON), cam-type femoroacetabular impingement (FAI), and finally osteoarthritis of the hip joint (OA). 2 SCFE was reported as the primary etiologic factor for OA in about 5% of the patients who had undergone total hip arthroplasty. 3 Therefore, an effective and successful initial treatment plays a key role in avoiding such serious complications. However, controversy still exists on the optimal initial treatment regimen in different types of slips.4,5 For example, it is generally agreed that in-situ fixation by screw is the treatment of choice in most of the mild and stable slips, whereas the optimal treatment for moderate to severe and unstable slips seems to be controversial particularly after the introduction of new, challenging surgical techniques of the hip joint.4,5 Moreover, a gradual decrease in the rate of in-situ fixation performed as the primary SCFE treatment as well as an increase in the rate of more complex repositioning surgeries have already been reported. 6
Up to date, several survey studies about the treatment of SCFE have been published.7–12 The results of these surveys revealed that there was considerable disagreement among the respondents on several aspects of SCFE treatment. However, to our knowledge, a Delphi consensus study on the treatment of all possible SCFE clinical scenarios has not been conducted, yet. We hypothesized that:
Hypothesis 1 (H1): Establishment of a wide consensus on the treatment of SCFE might help to develop a guideline for SCFE treatment in the daily clinical practice.
Therefore, the aim of this expert consensus study by the Delphi method was to establish as much consensus as possible on the treatment of different types of slips that could be seen in daily clinical practice as well as on the use of prophylactic screw fixation of the contralateral unaffected side, based on the reviews of the experienced orthopedic surgeons who were primarily involved in the treatment of pediatric patients.
Method
In this study, a four-round Delphi method was used in a single panel. 13 The contents of the methodology stages in this study were as follows:
Selection of the participants
A letter of invitation to participate in the consensus study on the treatment of SCFE was sent by e-mail to 22 experienced orthopedic surgeons whose daily clinical practice included mainly pediatric patients and who were active members of the Turkish Society of Children’s Orthopaedics. One week later, a reminder invitation e-mail was sent to the ones who had still not responded to the first e-mail. Among the invited 22 surgeons, 14 accepted to participate in the study. The number of respondents was considered to be sufficient according to the Delphi method. 13 Ten of 14 participants were academic staff at the university and 4 participants, working in their private clinics, worked as an academic staff at the university in the past. Expertise time as an orthopedic surgeon of the participants ranged from 15 to 31 years with a mean of 23 years.
Preparation of the surveys in rounds
All the possible theoretical slip scenarios were defined based on the universally accepted classifications according to the degree of displacement of the proximal femoral epiphysis on the femoral neck, to the patient’s ability to bear weight and to the onset of symptoms. “Mild,” “moderate” and “severe” SCFE were defined as “Southwick’s head-shaft angle” difference between the affected and unaffected sides: <30°; or <1/3 slippage, 30°–50°; or 1/3 to 1/2 slippage and >50°; or >1/2 slippage, respectively. “Stable” and “unstable” SCFE were defined as “weight bearing possible with or without crutches” and “weight bearing not possible even with crutches due to sudden severe pain,” respectively. “Acute,” “chronic” and “acute on chronic” SCFE were defined as “slip causing pain <3 weeks,” “slip causing pain ≥3 weeks” and “sudden worsening of pain in a chronic case,” respectively.1,2 Then, all possible theoretical clinical scenarios were set up and the questionnaire was composed of four main titles like “mild SCFE,” “moderate SCFE,” “severe SCFE” and “prophylactic screw fixation of the contralateral unaffected side” (Tables 1–4).
The results in mild SCFE.
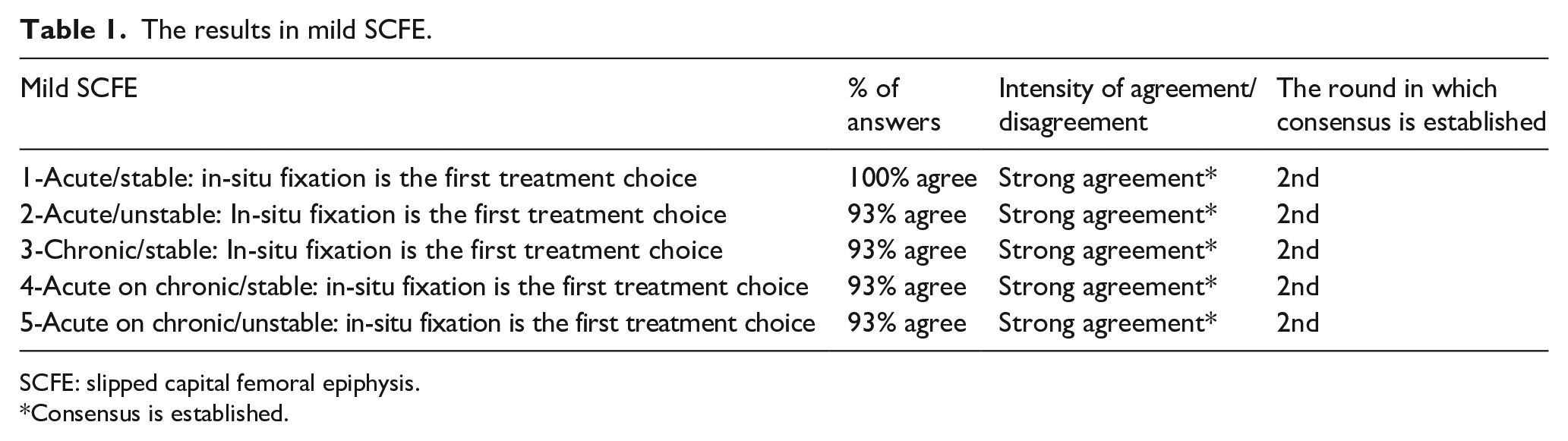
SCFE: slipped capital femoral epiphysis.
Consensus is established.
The results in moderate SCFE.
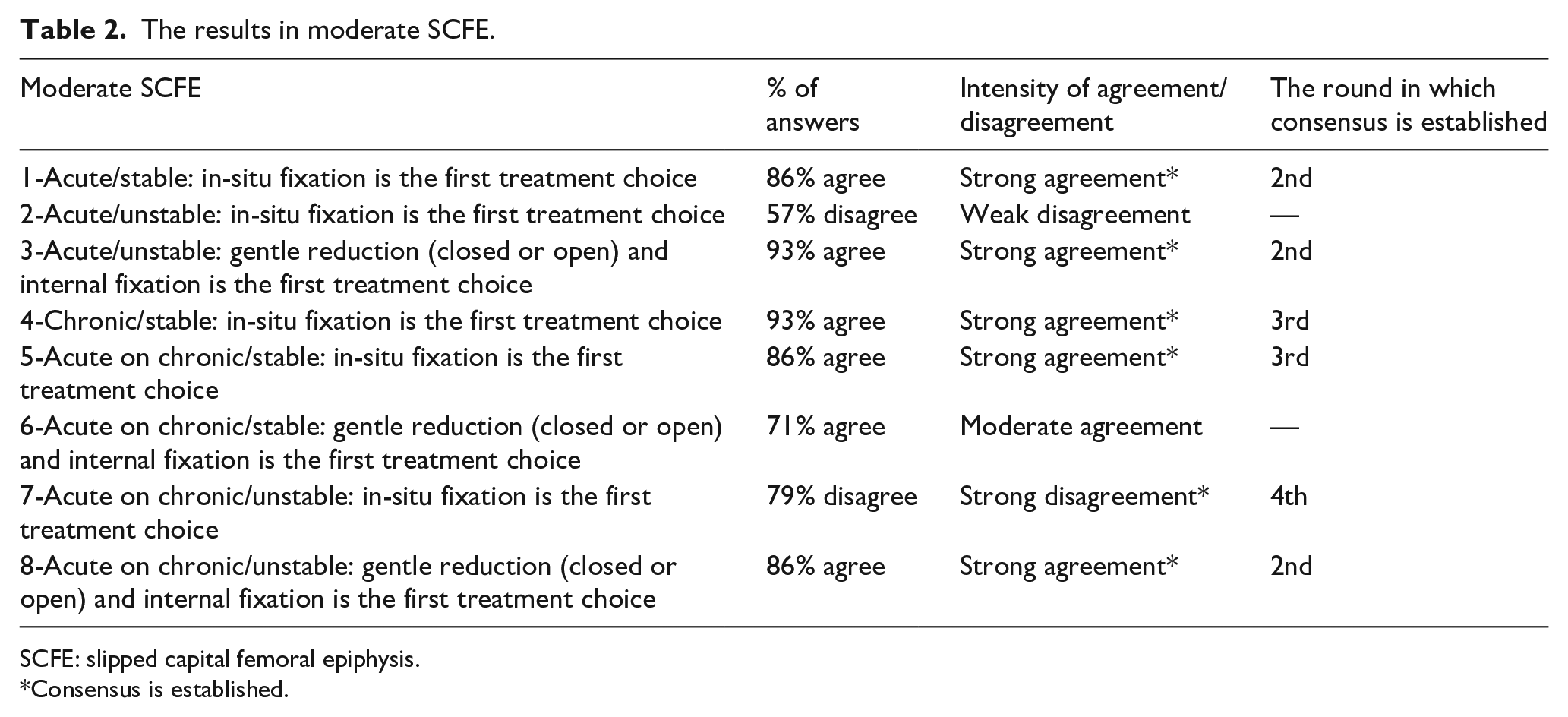
SCFE: slipped capital femoral epiphysis.
Consensus is established.
The results in severe SCFE.
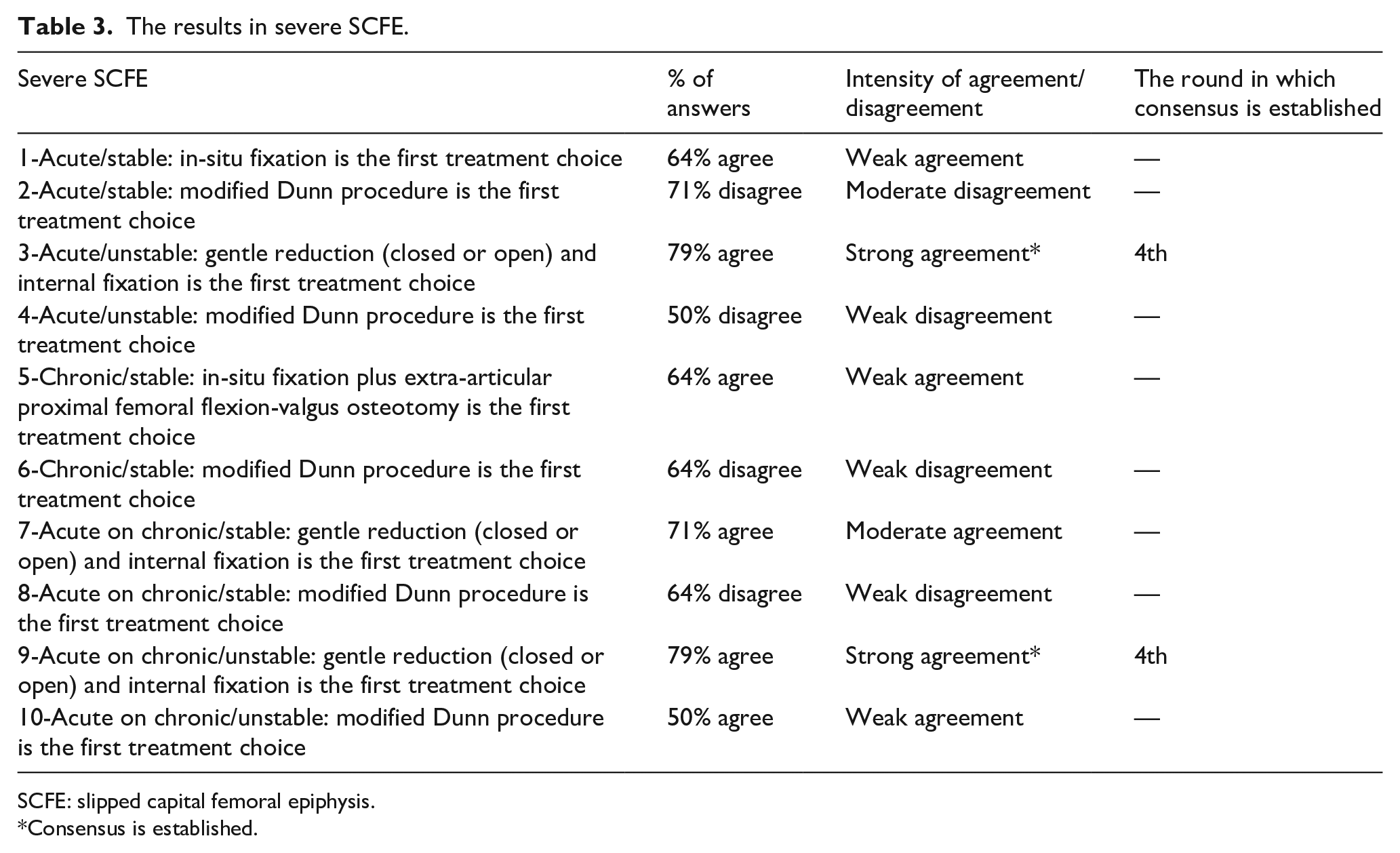
SCFE: slipped capital femoral epiphysis.
Consensus is established.
The results in prophylactic screw fixation.
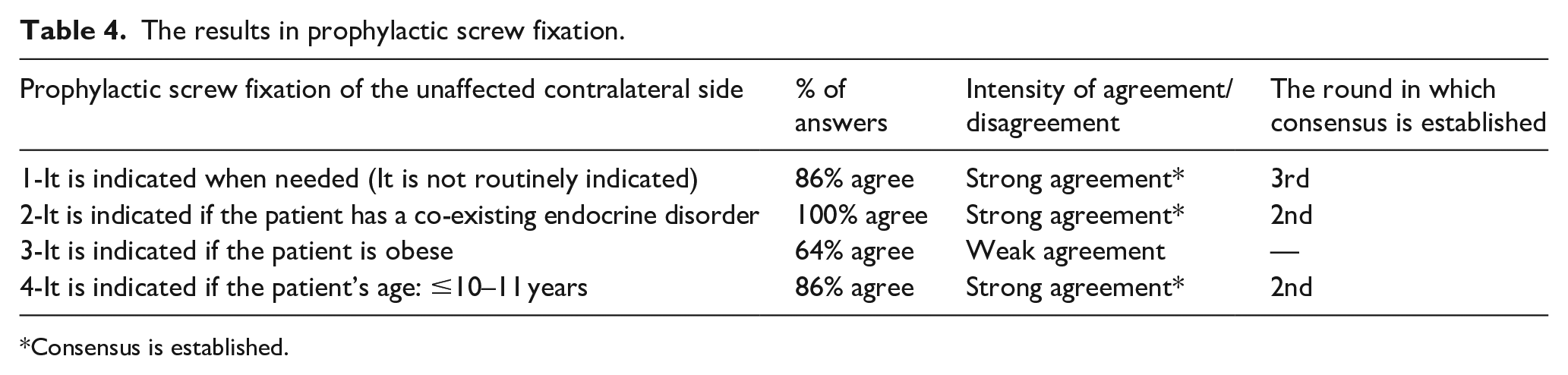
Consensus is established.
Round 1 questionnaire included open-ended questions, and the respondents were asked to specify their first treatment choices in 15 possible theoretical SCFE scenarios as well as their preferences in prophylactic screw fixation of the contralateral side. Round 2 questionnaire included 27 multiple choice questions based on the data obtained in the first round and each including 5 responses according to the “5-point Likert-type scale” (strongly agree, agree, neutral, disagree, strongly disagree) 14 in 4 main titles (Tables 1–4). Threshold value for consensus was initially fixed. “Consensus (strong agreement or strong disagreement)” was considered to occur when at least 11 of 14 the Delphi panelists (≥79%) selected one of the highest two responses (strongly agree or agree) and the lowest two responses (strongly disagree or disagree) according to the “5-point Likert-type scale.” 14 “Moderate agreement/disagreement” and “weak agreement/disagreement” were considered to occur when 70% to 78% and 50% to 69% of the Delphi panelists chose one of the highest and the lowest two responses, respectively. In the third and fourth rounds, the respondents were asked whether or not they were willing to review their decisions for the items in which a consensus had still not been established. 13 In these rounds, the response categories were given as “agree-neutral-disagree” in a 3-point Likert-type scale. The consensus was determined according to the rule specified for Round 2.
Data collection and management
Questionnaires were submitted online to the respondents consecutively in each round. Study data were collected and managed using REDCap (Research Electronic Data Capture) tools15,16 hosted at the Ankara Yildirim Beyazit University Statistics Consultancy Application and Research Center. REDCap is a secure, web-based application designed to support data capture for research studies, providing (a) an intuitive interface for validated data entry; (b) audit trails for tracking data manipulation and export procedures; (c) automated export procedures for seamless data downloads to common statistical packages; and (d) procedures for importing data from external sources.15,16
Results
Among total 27 statements, consensus was established in the second round in 10 statements (Tables 1, 2 and 4), in the third round in three statements (Tables 2 and 4) and in the fourth round in three statements (Tables 2 and 3). A consensus was established in five of the five statements in mild slips in the second round (Table 1). A consensus was established in six of the eight statements in moderate slips, but the achievement of consensus in the moderate slip statements was not as rapid as the achievement in the mild ones (Table 2). Consensus was established in 2 of the 10 statements in severe slips in the fourth round (Table 3). Three of the four statements in the prophylactic screw fixation of the contralateral side achieved consensus (Table 4). A consensus established on the fact that, in-situ fixation was the first choice of treatment in all types of mild slip scenarios (Table 1). In moderate, stable slip scenarios, in-situ fixation was considered to be the first treatment choice, whereas in moderate, unstable slip scenarios, there was a consensus on the use of gentle closed or open reduction and internal fixation (Table 2). When the consensus levels on the treatment of severe slip scenarios were analyzed, consensus was only established on the use of gentle closed or open reduction and internal fixation in severe, unstable slip scenarios. No consensus was established in the optimal treatment of severe, stable slips and moreover a weak disagreement on the use of the modified Dunn procedure in all severe slip scenarios was observed (Table 3). There was a consensus on the statements that prophylactic screw fixation of the contralateral side was indicated when needed and co-existing endocrine disorder and younger age were the indications for this procedure (Table 4).
Discussion
Surgical treatment is indicated in SCFE, but the preferred treatment regimens have undergone considerable changes as the surgical techniques have improved. Thus, such innovations have raised the controversies regarding the best treatment approaches in different types of SCFE. 4 It has recently been stated that, one of the top research priorities of the pediatric orthopedic surgeons to clarify the confronting clinical dilemmas where evidence is lacking, is the field of SCFE. 17 The present study aimed to establish a consensus among experienced surgeons on the treatment of all possible theoretical clinical scenarios in SCFE, so that a surgical treatment guideline for SCFE might be developed.
It is controversial whether the results obtained from this consensus study are widely acceptable or locally adaptable, as several geographical, sociocultural, and economic factors may influence the attitudes of parents and patients. Besides, some surgeons may perform a limited range of treatment options, whereas some surgeons may have advanced training to perform even the most challenging surgeries. Moreover, a questionnaire alone may not precisely cover all the variables which a surgeon considers when planning the management of a patient. Finally, it might have been better not to combine closed or open reduction together in description of the reduction technique in the treatment alternatives as considerable debate on the use of particularly closed reduction still goes on. These factors may be considered as the limitations of the present study. However, the group of respondents in the present study was homogeneous as all the Delphi subjects were highly trained and competent within the field of children’s orthopedics and the treatment of hip disorders in children. The optimal number of respondents in a Delphi study is still controversial, but 10 to 15 respondents can be considered sufficient if the background of the Delphi subjects is homogeneous. 13 Besides, a four round-questionnaire was completely responded by all the attending respondents. These were the important strengths of the methodology in the present study.
Several survey studies about the management of SCFE are older than 10 years, so one can think that these surveys may not precisely reflect the opinions of the respondents about the current improvements in the SCFE surgery.8,10,12 In one Pediatric Orthopaedic Society of North America (POSNA) survey study, more than 80% of the respondents were in favor of performing in-situ fixation in acute unstable slips. 8 In another survey from Western Europe, while less experienced surgeons were found to be more prone to perform in-situ fixation, more experienced surgeons more commonly preferred proximal femoral epiphysis repositioning in acute unstable slips. 12 In an European Paediatric Orthopaedic Society survey study, a higher agreement in the treatment of the stable slips by in-situ fixation and higher variability in the treatment of the unstable slips were observed. 10 On the other hand, newer survey studies have somewhat similar conclusions with the older ones have had. In a recent POSNA survey, the treatment of SCFE was found to be significantly surgeon dependent. 11 British Society of Children’s Orthopaedic Surgery members were more prone to perform in-situ fixation in SCFE, but this preference was higher in mild slips. 7 A higher rate of agreement in the treatment of stable, mild/moderate slips by in-situ fixation, stable, severe slips by capital realignment procedures and a higher variability in the treatment of unstable slips were observed in a survey conducted among the members of the Pediatric Orthopaedic Society of India. 9 In this study, experienced surgeons could not achieve considerable agreement on the optimal treatment of all severe slip scenarios. However, respondents of the present survey strongly agreed on the optimal treatment of all types of mild and moderate slip scenarios. We observed that the severity of the slip was the first determinant of the surgeons’ treatment choices, followed by the stability of the slip.
Although SCFE is an important hip disorder, a high level of scientific evidence concerning its surgical treatment is limited. 5 In-situ fixation currently seems to be the most commonly preferred surgical technique in the treatment of almost all types of SCFE and has a grade B recommendation on the basis of level of evidence in the treatment of stable SCFE as well.4,18 Better long-term outcomes were observed in hips having an initial slip angle of 35° and less. 19 In-situ fixation was the primary treatment preference of the respondents in the present study in all types of mild slips and a rapid consensus was established on this issue. Besides, the use of in-situ fixation was strongly agreed in moderate, stable slip scenarios. However, the presence of moderate to strong disagreement on the use of in-situ fixation in moderate, unstable slips and avoidance of performing in-situ fixation in severe slips should be emphasized. The most reasonable explanation of these facts may be the presence of respondents’ doubts about the sufficiency of in-situ fixation alone to avoid further complications in remarkably displaced and unstable slips.
Gentle open reduction and internal fixation of unstable mild to severe slips were reported to be a safe procedure with acceptable clinical and radiological outcomes. 20 Gentle closed reduction followed by internal fixation was reported as a reasonable option in the treatment of unstable slips without significantly increasing the risk of ON. 21 In this study, there was a consensus on performing gentle closed or open reduction and internal fixation in moderate to severe, unstable slips, but this consensus could be established at the end of the fourth round of questionnaire. This finding may demonstrate first the respondents’ sensitivity for obtaining capital realignment to lessen the risk of complications such as FAI, ON, and OA in moderate to severe, unstable slips, and second, the difficulties to determine the optimal treatment in such kinds of slips.
The modified Dunn’s procedure 22 is an innovative surgical technique, which has raised discussions about the optimal treatment of particularly moderate and severe slips. No significant difference was found between the modified Dunn procedure and the in-situ fixation regarding the short-term clinical outcomes in patients with moderate or severe slips. Although significant improvement can be observed in radiological outcomes, controversy still exists whether or not better outcomes can be obtained in stable and unstable slips, and additionally the number of long-term follow-up studies is very limited in this novel surgical technique.4,23,24 Modified Dunn procedure was only taken into consideration in severe slips by the respondents in the present study, but a weak to moderate disagreement on the use of this procedure in all severe stable and unstable slip scenarios was observed. Therefore, respondents of the present study seem to be influenced from the limited current scientific evidence about the wider use of modified Dunn procedure in severe type of SCFE.
Femur intertrochanteric flexion and valgus osteotomy is an option in the treatment of chronic, stable, moderate to severe slips. Satisfactory results with low complication rates were previously reported. 25 In this study, a weak agreement on the use of this technique in severe, chronic, stable slips was observed. The respondents do not seem to be in favor of using this technique in the treatment of any type of slips.
The use of prophylactic screw fixation of the contralateral unaffected hip is still debatable. Obesity, younger age, endocrine abnormalities, and several radiographic indicators have commonly been considered as the risk factors for the development of subsequent slip in the contralateral hip and prophylactic screw fixation of the contralateral hip has usually been recommended under such certain circumstances. 26 In the published surveys, less than one-third of the respondents preferred prophylactic screw fixation of the unaffected contralateral hip at the same session.7–10,12 In this study, prophylactic screw fixation was only preferred when needed and the existence of an endocrinopathy and younger age were the indicators of prophylactic screw fixation which the respondents had reached a consensus. These findings are compatible with the existing knowledge in the literature.
Conclusions
We conclude that the establishment of consensus on the treatment of all types of SCFE even among the experienced surgeons does not seem to be possible. Severity of the slip and stability of the slip are the first and second determinants of the surgeons’ treatment choices, respectively. Consensus exists on the optimal treatment method for mild and moderate SCFE. In-situ fixation is still the preferred treatment option in several SCFE scenarios including all types of mild SCFE as well as the stable type of moderate SCFE. However, its use is not favored in moderate, unstable and in all types of severe SCFE. Capital realignment by gentle closed or open reduction followed by internal fixation is the first treatment choice in the moderate to severe, unstable SCFE. No consensus exists on the optimal treatment method of severe, stable SCFE. Consensus exists on the fact that; prophylactic screw fixation of the contralateral hip is not routinely indicated but should be performed in patients having endocrine disorders and aging at or younger than 10–11 years.
Footnotes
Acknowledgements
The authors gratefully thank the respondents who have seriously contributed to the present study by kindly answering all the questionnaires with great caution. The list of respondents: Hüseyin Arslan, MD, Diyarbakir; Emel Gönen Baş, MD, Istanbul; Fuat Bilgili, MD, Istanbul; Emre Çullu, MD, Aydin; Muharrem Inan, MD, Istanbul; Önder Kalenderer, MD, Izmir; Volkan Kilinçoğlu, MD, Gaziantep; Nusret Köse, MD, Eskişehir; Kaya Memişoğlu, MD, Kocaeli; Bartu Sarisözen, MD, Bursa; Hakan Şenaran, MD, Konya; Muharrem Yazici, MD, Ankara; Timur Yildirim, MD, Istanbul; Güney Yilmaz, MD, Ankara.
Author contributions
D. Karagüven: Acquisition of data; drafting the work and revising it critically for important intellectual content; gave final approval of the version to be published; agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
P. Demir: Acquisition, analysis, and interpretation of data; revising it critically for important intellectual content; gave final approval of the version to be published; agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
S. Yüksel: Design of the work, acquisition, analysis, and interpretation of data; revising it critically for important intellectual content; gave final approval of the version to be published; agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
H. Ömeroğlu: Conception and design of the work, interpretation of data; drafting the work and revising it critically for important intellectual content; gave final approval of the version to be published; agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Ethical approval
The present study was approved by the Ufuk University Faculty of Medicine Ethics Committee (approval number: 23.01.12.01./10). All procedures performed in this study were in accordance with the ethical standards of the institutional ethics committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. This is a survey study that has been based on theoretical clinical scenarios and does not include any patient data. Any written informed consent provided from the patients is not available.
Declaration of conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.