
Abstract
Background: Historically, pediatric patients with myelodysplasia have been found to have a higher percentage of body fat than age-matched, healthy controls. This study examines the relationship between body fat percentage and age, sex, neurologic level, walking ability, and comorbidities in pediatric myelodysplasia patients.
Methods: A total of 91 patients underwent a thorough history and physical to document body fat percentage, neurologic level, and walking ability; a chart-review determined comorbidities.
Results: Females with myelodysplasia had significantly higher percent body fat than males (p = 0.02). Among females, body fat percentage increased with age (1.2% per year). Males who were community ambulators had lower body fat than those who were household ambulators or nonambulatory. In both sexes, those with mid/high neurologic levels had significantly higher body fat than those with low neurologic levels. There was no relationship between comorbidities and body fat.
Conclusions: In patients with higher neurologic levels and impaired walking abilities, treatment aimed at controlling obesity should be integral to the care of myelodysplasia patients.
Myelodysplasia, also called spina bifida cystica, results from incomplete closure of the neural tube during embryologic development. Due to subsequent neurologic impairment, myelodysplasia is one of the most common causes of locomotor disability in the pediatric population. 1 Previous studies by Hoffer and colleagues 2 have illustrated that most patients with myelodysplasia achieve their maximal ambulatory ability at 9 years of age and then gradually deteriorate in their walking ability. Reasons for this loss of ambulation are multifactorial and include the effects of concomitant deformities such as hip flexion contracture, scoliosis, and pelvic obliquity. 3 It has been hypothesized that functional deterioration is also associated with an increased energy requirement for ambulation accompanied by an increase in body weight during adolescence. 3
Pediatric myelodysplasia patients have a higher percentage body fat (%BF) than age-matched controls. 1 , 4 However, clear evidence for a relationship between body fat percentage and age, neurologic level, and walking ability in children with myelodysplasia is lacking. It has been documented in the literature that, in a healthy pediatric population, increased body fat is associated with multiple health risks, including an increased risk of hypertension, high cholesterol, non-insulindependent diabetes, and adult obesity. 5 This study specifically examines the relationship between body fat percentage and age, sex, neurologic level, walking ability, and comorbidities in pediatric myelodysplasia patients.
Materials and Methods
This study included 91 patients (36 male and 55 female) regularly followed in the Myelodysplasia Clinic (Table 1). The average age of the patients is 12.4 years (range: 8 to 20 years). In order to participate in this study, patients or their family members provided informed consent for a review of medical history, physical exam, chart review, and anthropometric measurements. This study was approved by the Institutional Review Board of Shriners Hospitals for Children, Los Angeles.
Demographic Data for Patients with Myelodysplasia

A thorough physical exam was performed in order to determine the clinical neurologic level of each patient at the time that his or her body fat percentage was assessed.
Neurologic level was defined as the lowest muscle group capable of antigravity contraction (grade 3). The patients were categorized by neurologic level as High (thoracic-L2), Mid (L3-L4), and Low (L5-sacral) as has been previously established. 3 Asymmetric paraplegia, with a disparity in the neurologic level between the two lower extremities of one individual, was recorded as that of the lowest level. 2 Patients were also classified by their walking ability. Each patient was designated as Community Ambulator, Household Ambulator, or Nonambulator. 2 Skinfold thickness measurements were taken using The Body CaliperTM (The Caliper Co., Littleton, CO) at the triceps and subscapular sites. 6 The %BF was then calculated using the formula described by Slaughter and coworkers. 7 Comorbidities were determined via a review of the patients’ medical records for the 12 months prior to individual skin fold measurements. The severity of pressure sores was determined according to The Merck Manual of Diagnosis and Therapy. 8
Statistical analysis included linear regression analysis and a two-sample Student’s t-test (Stata 7, StataCorp LP, College Station, TX). Statistical significance was defined as p < 0.05.
Results
Among pediatric patients with myelodysplasia, females had a significantly higher average %BF than males (31.6% versus 25.5%, p = 0.02), (Fig. 1). In all patients, regardless of gender, %BF was related to neurologic level. Female patients with Mid or High neurologic levels had an average %BF of 32.5%, while those with a Low level had an average of 28.6% (p = 0.047) (Fig. 1). Male patients with Mid or High neurologic levels had a higher %BF (28.0%) than those with a Low level (19.0%; p = 0.046), (Fig. 2).

Percent body fat (%BF) by gender.
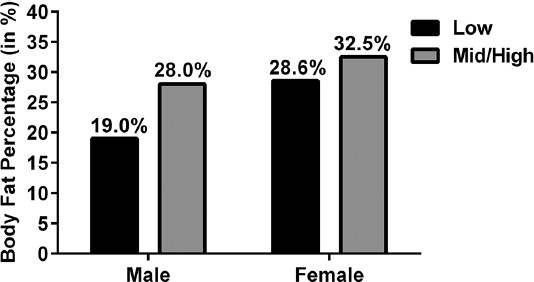
Percent body fat (%BF) by neurologic level and gender.
Among males, community ambulators had a lower average body fat (23.1%) than those who were household ambulators or nonambulatory (23.1% versus 31.7%, p = 0.05) (Fig. 3). This relationship was not seen in the female subgroup (Fig. 3). In males, there was no statistically significant relationship between %BF and age. However, in females, body fat increased with age, at an average of 1.2% each year (p = 0.001).
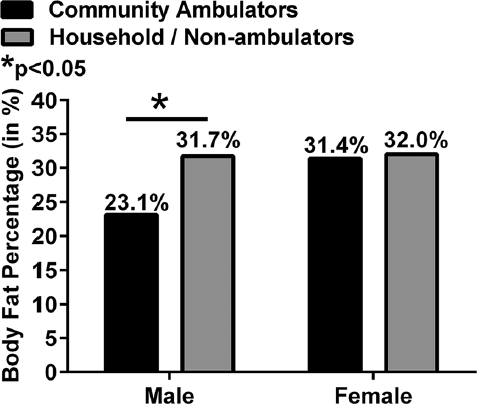
Percentage body fat (%BF) versus walking ability of patients with myelodysplasia.
Physical exam, laboratory studies, and chart reviews of the 12 months prior to the calculation of % BF revealed 70 comorbidities in 52 patients (Table 2). These conditions included pressure sores, urinary tract infections requiring antibiotic therapy, hip dislocations, postoperative infections, lower extremity fractures, and a suprapubic lipectomy performed to allow for urinary catheterization and maintenance of hygiene in a morbidly obese patient. Multivariate analysis of the data revealed no relationship between %BF and the presence or severity of comorbidities (p = 0.30).
Comorbidities Noted Within 12 Months of Skin-Caliper Testing

Stages of pressure sore formation were designated, using the suggested method from The Merck Manual of Diagnosis and Therapy. 8
Discussion
Childhood obesity has become one of the most important social health concerns of the industrialized world. 4 , 9 It has been documented that greater than 50% of obese children will carry their excess %BF into adulthood. In an otherwise healthy pediatric population, this elevated %BF increases the risk of hypertension, high cholesterol, non-insulindependent diabetes, and cardiovascular disease as adults. 4 About 60% of overweight 5- to 10-year-old children already have one associated cardiovascular risk factor (i.e., hyperlipidemia, elevated blood pressure, etc.). 9 In the pediatric myelodysplasia population, the specific relationship of %BF to these comorbidities has not yet been elucidated.
The measurement of %BF in children can be performed by a variety of methods, including hydrostatic weighing, radioisotope dilution, dual energy x-ray absorptiometry (DEXA), bioelectric impedance analysis, and skin fold measurements.10-12 In an examination of pediatric patients with myelodysplasia, Mita and colleagues 11 determined that values of %BF calculated using skinfold thickness measurements of the triceps and subscapular regions were highly correlated with those obtained with hydrostatic weighing, a technique often regarded as the gold standard for %BF measurements. When compared, skinfold thickness measurements and hydrostatic weighing yielded results that were within 2% to 3% fat for their subjects. Significant correlation of body fat measurements between the two methods has also been found in additional studies. We, therefore, chose to use triceps and subscapular skinfold measurements to determine the %BF of the patients in this study.
In healthy children, %BF increases in the first year of life, then declines to its lowest point by the age of 6 to 7 years. 13 After the age of 2 to 3 years, healthy males tend to have a lower %BF than age-matched females. Female body fat gradually increases throughout adolescence, while the percentage body fat in males peaks at 12 to 13 years and then declines through the remainder of the teenage years. The patients in this study followed a similar trend. We found that males with myelodysplasia had a significantly lower average %BF than females with the same disorder (25.5% and 31.6%, respectively), which mirrors the relationship seen between the sexes in healthy pediatric controls. Female myelodysplasia patients had an average increase in %BF of 1.2% per year, while males showed no such increase. In previous studies comparing the %BF of males and females with myelodysplasia, no significant difference was noted. 1 , 14 However, these studies did not use skin fold measurements, which are the best alternative to the gold standard in determining %BF.
The increasing prevalence of obesity in children without myelodysplasia has been linked to the more sedentary lifestyle of today’s youth compared to that of previous gen- erations. 9 If a relative lack of activity is associated with an increase in %BF in otherwise healthy children, it is plausible that myelodysplasia patients, who are more sedentary due to their inability to ambulate, will be at risk for increased %BF for this reason. According to Asher and associates, 3 neurologic level was the single most important factor in determining the walking ability of myelodysplasia patients (i.e., those with higher level of neural involvement will have less functional walking ability). We specifically and individually investigated the relationship between %BF and neurologic level as well the relationship between %BF and ambulation classification.
Previous studies evaluating the relationship of body fat to neurologic level have yielded mixed results. Roberts and coworkers 1 and Bandini and colleagues 15 found no significant difference in body fat between the different neurologic levels, although their results indicated that all neurologic levels had a higher %BF than age-matched healthy controls. Shepherd and associates 16 compared %BF of patients with myelodysplasia to that of age-matched controls, reporting that only patients with Mid or High neurologic levels had significantly greater %BF than that of the healthy controls. Those with Low neurologic levels demonstrated no such increase. Mita and colleagues 11 also noted a trend toward an increase in body fat with higher neurologic level, although this relationship did not achieve statistical significance. Our data shows a clear relationship between %BF and neurologic level. Both males and females with a Low neurologic level had a significantly lower %BF than those with Mid or High levels (Fig. 2).
A trend toward increasing %BF with decreasing walking ability has been noted in previous studies. Shepherd and as- sociates 16 found that nonambulators had significantly higher body fat than age-matched controls, while more ambulatory patients showed no such difference. Similarly, Asher and associates 3 noted that increased body weight was a negative prognostic indicator of whether patients with high-level myelodysplasia would be able to walk. The results of Mita and colleagues 11 also indicated a trend toward increased body fat percentage in nonambulators relative to ambulators, but this result was not statistically significant. In our study of %BF and walking ability, we found that males who were community ambulators had a significantly lower %BF than those who were household ambulators or nonambulatory (Fig. 3). As confirmed by Mita and colleagues, 11 these results indicate that the obesity seen in certain myelodysplasia patients is at least partly due to the physical inactivity related to their paralysis.
Our hypothesis that increased body fat would be associated with increased orthopaedic comorbidities was not substantiated by this study. Body fat was not related to the incidence or the severity of the comorbidities identified in our patients. We believe this lack of correlation may be due to the study’s incomplete follow-up. If our patients’ progress was followed for a longer period of time, perhaps the comorbidities would be a more significant factor with regard to body fat percentage. Their severity may change over time, which may also be noted if the follow-up period was prolonged. To our knowledge, no previous studies have been performed to evaluate the relationship of %BF or obesity to comorbidities in patients with myelodysplasia. Further investigation into the health effects of elevated %BF on patients with myelodysplasia should be continued with special attention paid to extending the follow-up time period.
Conclusions
Pediatric patients with myelodysplasia have a higher %BF than healthy children of the same age. In addition, within a population of patients with myelodysplasia, it appears that %BF increases with age and decreased activity level. In both the female and male patients, those with Mid or High neurologic levels had increased %BF, compared to those with Low neurologic levels. These results suggest that appropriate nutritional guidance and physical therapy training programs aimed at controlling obesity should be instituted early and should become a regular part of the care of patients with myelodysplasia. Further prospective studies evaluating the effects of such programs remain to be performed.
Footnotes
Conflict of Interest Statement
None of the authors have a financial or proprietary interest in the subject matter or materials discussed, including, but not limited to, employment, consultancies, stock ownership, honoraria, and paid expert testimony.